What antibiotic is preferrable for huge ascities
Reading File
Finding Sources
Finding Sources
Searching PubMed
spontaneous bacterial peritonitis antibiotic treatment
Reading File
Reading File
Reading File
Loading Image
Here is a full answer based on authoritative textbook sources.
Antibiotic Treatment for Ascites with Suspected Infection (SBP)
"Huge ascites" in the context of antibiotic therapy almost always points to Spontaneous Bacterial Peritonitis (SBP) - the most common and serious infectious complication of cirrhotic ascites.
Diagnosis First
SBP is diagnosed by diagnostic paracentesis. The threshold for starting antibiotics is:
- Ascitic fluid PMN (neutrophil) count ≥ 250 cells/mm³
- Even if cultures are negative (up to 60% of SBP cases are culture-negative)
Most common causative organisms: E. coli, Klebsiella, streptococci, enterococci. - Bailey and Love's Short Practice of Surgery, 28th ed., p. 1111
Antibiotic Choice - Based on Acquisition Setting
The algorithm below (from Sleisenger & Fordtran's Gastrointestinal and Liver Disease) guides empirical therapy:
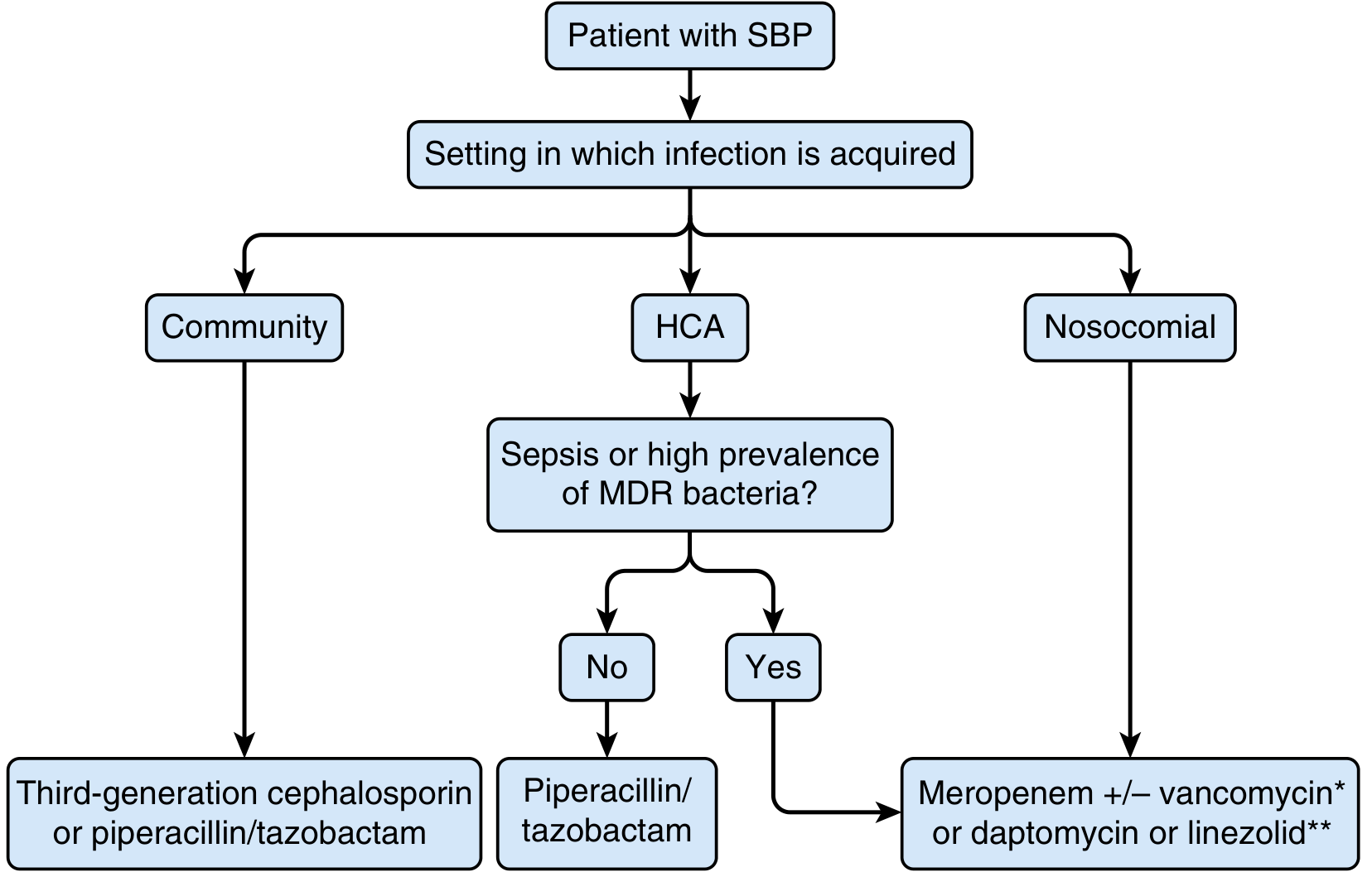
| Setting | First-Line Antibiotic |
|---|---|
| Community-acquired | 3rd-gen cephalosporin (e.g., cefotaxime) or piperacillin/tazobactam |
| Healthcare-associated (HCA), no sepsis, low MDR area | Piperacillin/tazobactam |
| HCA with sepsis or high MDR prevalence; Nosocomial | Meropenem ± vancomycin* or daptomycin/linezolid** |
* Use IV vancomycin in areas with high MRSA prevalence
** Use daptomycin or linezolid in areas with high vancomycin-resistant enterococci (VRE) prevalence
First-Line (Community-Acquired SBP)
Cefotaxime 2 g IV every 8 hours for 5 days is the standard regimen.
- It covers gram-negative enteric organisms (the main culprits)
- Avoids aminoglycoside nephrotoxicity, which is a concern in cirrhotic patients
- Source: Rosen's Emergency Medicine, 10th ed., p. 1235 and Bailey & Love's Surgery, 28th ed.
Alternatives for community-acquired SBP:
- Amoxicillin/clavulanic acid (oral or IV)
- Quinolones (ciprofloxacin) - particularly when oral therapy is appropriate
Key Adjunct: Albumin Infusion
Intravenous albumin (1.5 g/kg on day 1, then 1 g/kg on day 3) is given alongside antibiotics in SBP to prevent hepatorenal syndrome, especially in patients with:
- Serum creatinine > 1 mg/dL
- BUN > 30 mg/dL
- Bilirubin > 4 mg/dL
This combination (cefotaxime + albumin) significantly reduces mortality. - Sleisenger & Fordtran's Gastrointestinal and Liver Disease
Prophylaxis After an Episode
Once a patient recovers from SBP, long-term secondary prophylaxis is warranted:
- Norfloxacin or trimethoprim-sulfamethoxazole (daily oral)
- Goldman-Cecil Medicine also notes prophylaxis for patients with low ascites protein (< 1.5 g/dL) to prevent first-episode SBP
Monitoring Response
Repeat paracentesis at 48 hours after starting antibiotics. If PMN count does not decrease by ≥ 25%, consider treatment failure and switch antibiotics (especially consider MDR organisms). - Sleisenger & Fordtran's, p. 1807
Summary: For a patient with large ascites and suspected SBP, start cefotaxime 2 g IV q8h empirically (community-acquired) paired with IV albumin. Escalate to piperacillin/tazobactam or meropenem for healthcare-associated or nosocomial infections, especially if MDR bacteria are a concern in your region.
This is a shared conversation. Sign in to Orris to start your own chat.