


1000812912.jpg
+2 more
Explain
analyse_media
analyse_media
analyse_media
Here is a full explanation of all three images. These are DICOM plain radiographs of a 35-year-old patient (KASBE /35Y) showing a right proximal femur fracture managed surgically.
Image 1 & 2 - Pre/Peri-operative AP Pelvis and Right Femur (with external hardware)
These two views are essentially the same projection at slightly different zoom levels, captured intra-operatively or in a staging phase.
Key findings:
- Right proximal femur: Severe, highly comminuted and displaced fracture of the intertrochanteric/subtrochanteric region, with significant shortening, varus collapse, and fragmentation of the greater trochanter. The femoral head is still seated in the acetabulum.
- No internal fixation yet: No permanent orthopaedic implant is inside the bone at this stage.
- External devices visible:
- Surgical drains (loop-shaped radiopaque tubes) - likely Jackson-Pratt or Hemovac drains in the soft tissues around the right hip/thigh, suggesting a prior procedure or infection control
- IV/monitoring catheter overlying the medial thigh
- A Foley catheter balloon is likely visible in the pelvis
- Proximal femoral bone shows cortical thickening and sclerosis, suggesting a chronic process (possibly prior osteomyelitis or previous Girdlestone resection arthroplasty where the implant was removed due to infection)
The combination of absent hardware + drain tubes + sclerotic/distorted proximal femur strongly suggests this patient has a history of periprosthetic joint infection with implant removal (Girdlestone procedure), and is now presenting with a new or residual fracture.
Image 3 - Post-operative AP Right Hip and Proximal Femur (with implant)
This is the definitive post-operative radiograph after surgical fixation.
Key findings:
- Implant: Cephalomedullary nail (Gamma Nail / Proximal Femoral Nail)
- A long intramedullary nail runs down the femoral shaft
- Two large parallel lag screws extend from the nail laterally through the femoral neck into the femoral head (the characteristic "dual screw" pattern)
- Screws appear center-center positioned in the femoral head - ideal placement with no cut-out
- A distal interlocking screw is visible at the bottom of the nail
- Fracture alignment: Good. The neck-shaft angle is anatomically restored, no varus deformity
- Healing signs: Bony callus formation at the fracture site - indicating active, progressing bone healing
- Pelvis and left hip: Intact, normal alignment
- No hardware failure: No screw cut-out, nail breakage, or implant migration
Summary - Clinical Story
| Phase | Findings |
|---|---|
| Pre/peri-op (Images 1-2) | Comminuted right intertrochanteric/subtrochanteric fracture, no internal fixation, surgical drains present, chronic bony changes suggesting prior infection/Girdlestone |
| Post-op (Image 3) | Successful fixation with a cephalomedullary nail (Gamma-type), good alignment, early callus formation, hardware intact |
Diagnosis: Right comminuted proximal femoral fracture (intertrochanteric ± subtrochanteric) in a 35-year-old, with likely background of chronic infection/prior implant removal, treated with intramedullary cephalomedullary nailing.
This is a complex case in a young patient (35Y), where the surgical goal is fracture stabilization and restoration of hip biomechanics while managing the background of chronic bone disease or prior infection.
Explain and interpret
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
Here is a detailed explanation and interpretation of all three X-rays, now backed by textbook evidence.
Detailed Radiological Explanation and Interpretation
Patient Context
- 35-year-old (KASBE /35Y), right side (marked "R" in image 3)
- Date: July 22, 2026
- DICOM AP pelvis/proximal femur series
Images 1 & 2 - Pre-operative State
What you see:
These are AP views of the pelvis and right proximal femur before definitive fixation. The right side shows:
1. Comminuted Proximal Femoral Fracture
- A highly fragmented, displaced fracture involving the intertrochanteric and subtrochanteric regions - the zone between and below the greater and lesser trochanters
- The fracture is extracapsular (outside the hip joint capsule), so the blood supply to the femoral head is theoretically intact
- Significant shortening and varus collapse - the shaft has ridden up and the femoral neck is angulated inward
- The greater trochanter is fragmented and displaced - this is a major destabilizing feature
This diagram from Campbell's Operative Orthopaedics shows the exact zones:
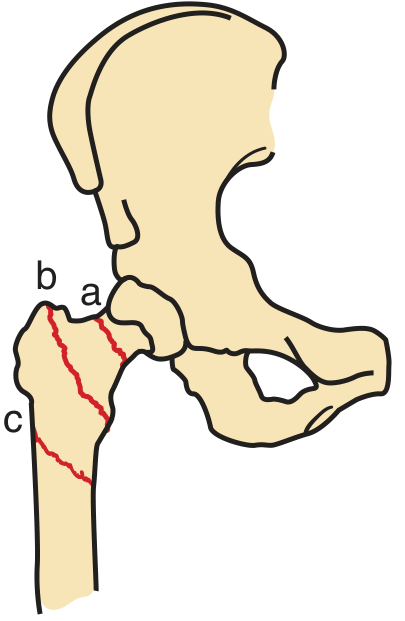
The fracture in this patient spans zones b + c (intertrochanteric + subtrochanteric) - this makes it an unstable, complex fracture pattern.
2. Background Bone Changes
- The proximal femur appears sclerotic and distorted with cortical thickening - signs of chronic bone remodeling, consistent with prior osteomyelitis or a previous implant removal (Girdlestone resection)
- There is no hardware inside the bone at this stage
3. External Devices (soft tissue overlays)
- Loop-shaped surgical drains (Jackson-Pratt or Hemovac type) - placed around the hip/thigh to evacuate fluid from a prior infection or debridement
- IV catheter over the medial thigh
- Foley catheter visible in the pelvis (standard for major pelvic/femoral surgery)
Why is this fracture so complex?
In a 35-year-old, this degree of comminution from an intertrochanteric/subtrochanteric fracture requires significant force (high-energy trauma). On top of this, the background sclerosis/bone changes mean the bone quality and anatomy are already compromised - making surgical fixation technically more challenging.
Image 3 - Post-operative Result
What you see:
A well-executed surgical reconstruction. The key implant is a Cephalomedullary Nail (Gamma Nail / Proximal Femoral Nail).
Implant anatomy explained:
| Component | What it does |
|---|---|
| Intramedullary nail (long rod in femoral shaft) | Acts as an internal splint - load-sharing device inside the medullary canal |
| Two parallel lag screws (into femoral head/neck) | Compress and hold the femoral head/neck fragment to the shaft; dual screw provides rotational control |
| Distal interlocking screw (bottom of nail) | Prevents rotation and telescoping of the nail; important for subtrochanteric extension |
Why a cephalomedullary nail (not a plate)?
As per Miller's Review of Orthopaedics: the cephalomedullary nail is indicated for all unstable intertrochanteric fractures - reverse oblique fractures, subtrochanteric fractures, fractures with comminution, and fractures without an intact lateral femoral cortex. It offers:
- Less collapse than sliding hip screw (SHS) devices due to the intramedullary buttress effect
- Mechanical advantage - the nail is load-sharing (not load-bearing), reducing implant stress
- Allows weight-bearing as tolerated post-operatively
A long nail (as seen here) is specifically indicated when there is subtrochanteric extension, as in this case.
Implant position assessment:
Center-center lag screw placement - The screws are positioned centrally in the femoral head on this AP view. This is the ideal position. The Tip-Apex Distance (TAD) - a measurement from screw tip to apex of femoral head - should be less than 25 mm to minimize risk of cut-out (screw migrating through the femoral head into the joint). The positioning here appears satisfactory.
No cut-out - The screws have not migrated through the femoral head - the most feared hardware complication.
Neck-shaft angle - Appears anatomically restored. No varus malreduction (drooping of the femoral head), which is a known predictor of nail cut-out per Campbell's Operative Orthopaedics.
Callus formation - Hazy new bone bridging the fracture site at the intertrochanteric region indicates active, progressing bone healing.
Clinical Interpretation - Full Story
| Stage | Finding | Significance |
|---|---|---|
| Background | Sclerotic, distorted proximal femur, no hardware | Prior infection/osteomyelitis or Girdlestone procedure (implant removed for infection) |
| Acute injury | High-energy comminuted intertrochanteric + subtrochanteric fracture | Unstable pattern, requires operative fixation |
| Pre-op | Surgical drains in situ | Active infection management / debridement prior to definitive fixation |
| Post-op | Cephalomedullary nail, good alignment, center-center screws, callus | Technically sound fixation, healing progressing well |
Key concerns going forward:
- Infection risk - Given the background of probable prior infection and intramedullary hardware now implanted, this patient needs close monitoring for periprosthetic joint infection
- Screw cut-out - The dual lag screws must remain well-positioned; serial X-rays are needed
- Fracture healing - Callus is present but healing in a 35-year-old with prior bone disease may be slower
- Rehabilitation - Weight-bearing as tolerated is standard after cephalomedullary nailing; early mobilization is critical to prevent complications of immobility
This is a technically challenging case managed with an appropriate implant choice, and the post-operative result appears satisfactory.
Sources: Campbell's Operative Orthopaedics 15th Ed 2026; Miller's Review of Orthopaedics 9th Ed; Textbook of Family Medicine.
This is a shared conversation. Sign in to Orris to start your own chat.