Give medeial about gerd
Reading File
Finding Sources
Searching PubMed
"gastroesophageal reflux disease"[MeSH Terms] AND management
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Here is a comprehensive medical overview of Gastroesophageal Reflux Disease (GERD):
Gastroesophageal Reflux Disease (GERD)
Definition
GERD develops when reflux of stomach contents into the esophagus causes troublesome symptoms or complications. — Goldman-Cecil Medicine
Epidemiology
- Prevalence of 10–20% in the Western world; <5% in Asia
- In the US, up to 44% of people have experienced GERD symptoms, and 30% had symptoms in the prior week
- Higher prevalence in North America vs. Europe, and in northern vs. southern Europe
- Risk factors: obesity (especially central), positive family history, monozygotic twins, increasing age
Pathophysiology
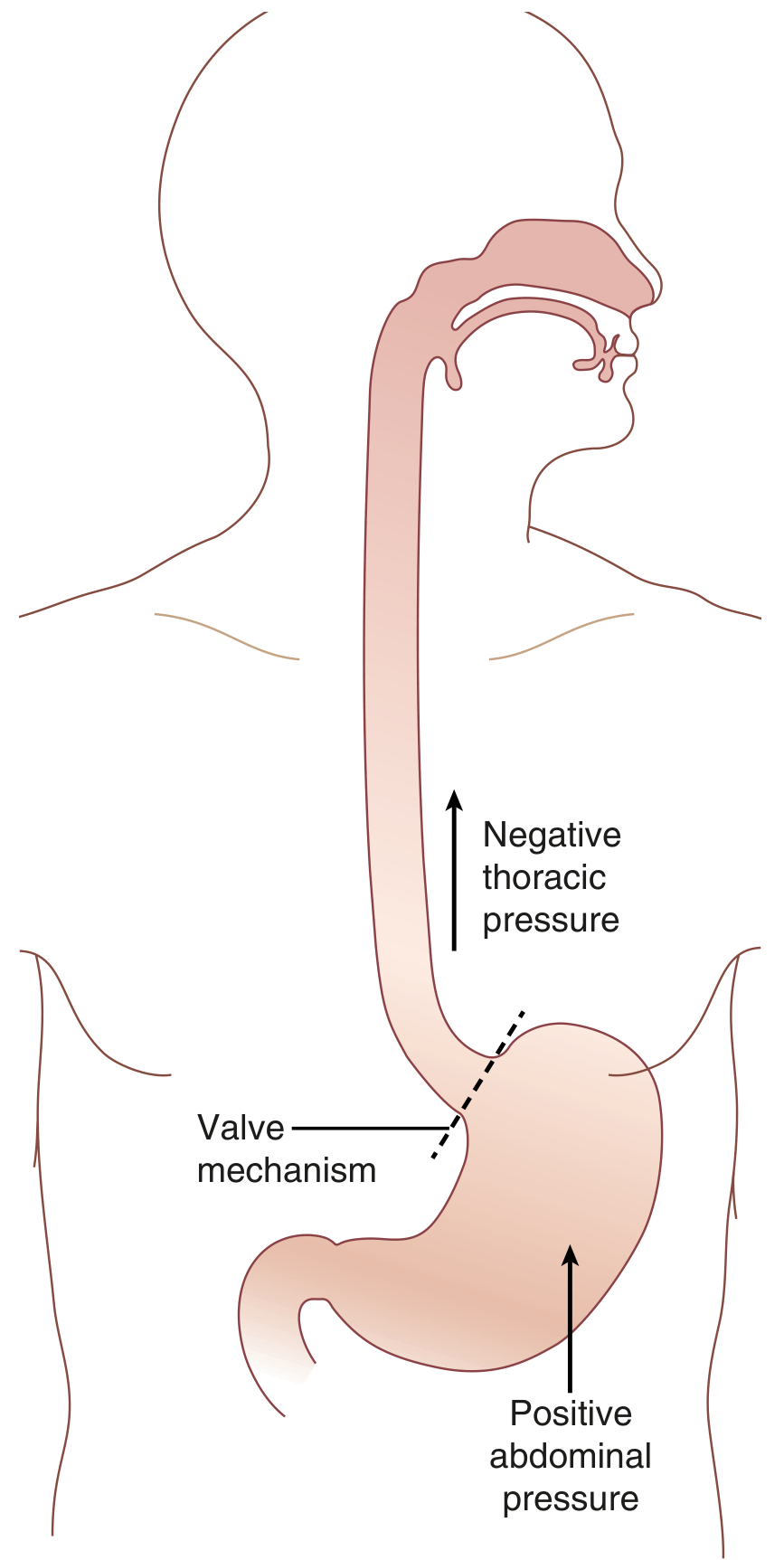
GERD occurs because of an imbalance between the transdiaphragmatic pressure gradient and the valve mechanism at the esophagogastric junction (EGJ). — Sabiston Textbook of Surgery
The antireflux barrier consists of five components:
- Lower esophageal sphincter (LES) — a 3–4 cm high-pressure zone; majority of GERD patients have a defective LES, though a large proportion have normal LES pressure
- Crural diaphragm — extrinsic pinching of the lower esophagus during increased abdominal pressure
- Angle of His — the acute angle between the esophagus and gastric fundus acts as a barrier to refluxate rise
- Gubaroff valve — mucosal thickening at the EGJ acting as a cushion
- Intra-abdominal portion of the esophagus — collapsed by abdominal pressure
GERD occurs in three main scenarios:
- Increased abdominal pressure — obesity (especially central fat distribution), pregnancy, athletes
- Decreased thoracic pressure — obstructive pulmonary diseases, professional singers/glass blowers
- Defective EGJ valve — hiatal hernia is the most common cause (disrupts intra-abdominal esophageal length, angle of His, LES position)
In physiologic reflux, the LES undergoes transient relaxations triggered by gastric distention via a vagal reflex. In GERD, these relaxations are more frequent and pronounced. An acid pocket in the gastric cardia (unaffected by meal buffering) is a key source of postprandial reflux.
Clinical Features
Typical symptoms (esophageal):
- Heartburn — retrosternal burning, worse postprandially, may mimic ischemic chest pain
- Acid regurgitation — effortless return of sour-tasting gastric contents into the pharynx or mouth
- Dysphagia (when complications like stricture develop)
The severity of symptoms does not correlate well with histologic damage. Some patients with severe esophagitis or Barrett metaplasia report no heartburn. — Yamada's Gastroenterology
Atypical/extraesophageal symptoms:
- Chronic cough, hoarseness, laryngitis, asthma exacerbations
- Dental enamel erosion (irreversible, on palatal surfaces of maxillary teeth)
- Noncardiac chest pain
- In the elderly, regurgitation, dysphagia, dyspepsia, and noncardiac chest pain often predominate over heartburn
Aggravating factors: alcohol, tobacco, obesity, CNS depressants, pregnancy, hiatal hernia, delayed gastric emptying
Complications
| Complication | Notes |
|---|---|
| Erosive esophagitis | Mucosal erosions/ulceration; eosinophil infiltration on histology |
| Peptic stricture | Narrowing causing progressive dysphagia |
| Barrett esophagus | Intestinal metaplasia replacing squamous epithelium; premalignant |
| Esophageal adenocarcinoma | Most feared long-term complication |
| Enamel erosion | Dissolution of palatal tooth surfaces |
Diagnosis
When typical symptoms respond to antisecretory therapy: no further workup is required.
Endoscopy is indicated when:
- Alarm features: dysphagia, weight loss, anemia, GI bleeding, persistent heartburn
- Failure to respond to 4–8 weeks of therapy
- Suspected Barrett esophagus, stricture, or eosinophilic esophagitis
Other investigations:
- Ambulatory 24–48h pH monitoring (or wireless Bravo capsule): gold standard to quantify acid exposure and correlate symptoms with reflux events; use off PPI to document GERD, on PPI to investigate refractory symptoms
- Combined impedance-pH monitoring: detects both acid and non-acid reflux
- Esophageal manometry: to exclude achalasia in suggestive cases; assesses LES pressure before antireflux surgery
- Barium swallow: no role in uncomplicated reflux; useful for hiatal hernia or suspected dysmotility
Treatment
1. Lifestyle Modifications
- Weight loss (in obese patients)
- Elevate head of the bed (for nocturnal symptoms)
- Avoid precipitants: alcohol, coffee, spicy foods, late meals
- Small, frequent meals
2. Pharmacological (Acid Suppression — Table of Agents)
| Drug Class | Example | Dose |
|---|---|---|
| Antacids | Mylanta, Maalox | 15 mL four times daily as needed |
| Alginate-antacid | Gaviscon | 2–4 tablets QID and at bedtime |
| H₂-receptor antagonists | Ranitidine 150 mg bid, Famotidine 20–40 mg bid | — |
| PPIs | Omeprazole 20–40 mg/day | — |
| Lansoprazole 15–30 mg/day | — | |
| Pantoprazole 40 mg/day | — | |
| Esomeprazole 20–40 mg/day | — | |
| Dexlansoprazole 30–60 mg/day | — |
PPIs are the cornerstone of treatment — superior to H₂ antagonists for healing esophagitis and controlling symptoms. PPIs provide symptomatic relief in up to 90% of patients. Twice-daily dosing heals esophagitis faster but does not resolve symptoms faster than once-daily. No major differences in efficacy among PPI agents. — Robbins & Cotran Pathology; Goldman-Cecil Medicine
Long-term maintenance PPI therapy is typically required, especially for erosive esophagitis. Dose should be titrated to the lowest effective dose.
Barrett esophagus: ACG recommends once-daily PPI for chemoprevention of progression to adenocarcinoma.
3. Surgical Treatment
Fundoplication (Nissen — 360° wrap, or partial Toupet/Thal) wraps the gastric fundus around the distal esophagus, restoring the EGJ valve. Currently performed laparoscopically in most patients.
- Indications: failed medical therapy, patient preference, complications
- Complications: dysphagia (wrap too tight), gas-bloat syndrome, wrap breakdown with recurrent reflux
- Does not clearly offer cancer prevention over PPI therapy in Barrett esophagus
Key Clinical Pearls
- Up to 29% of patients eventually diagnosed with achalasia were initially treated for "refractory GERD" — pH monitoring helps differentiate
- Hiatal hernia disrupts all five antireflux mechanisms simultaneously
- Obesity worsens GERD by increasing intra-abdominal pressure AND promoting hiatal hernia formation
- PPI resistance in Barrett esophagus may reflect profound reflux diathesis rather than true pharmacologic resistance
Sources: Goldman-Cecil Medicine International Edition; Sabiston Textbook of Surgery; Robbins, Cotran & Kumar Pathologic Basis of Disease; Schwartz's Principles of Surgery; Yamada's Textbook of Gastroenterology; Sleisenger and Fordtran's Gastrointestinal and Liver Disease
This is a shared conversation. Sign in to Orris to start your own chat.