I 25 old male presents with bloody diarrhea with mucus, abdomen pain and fever. Stool examination showed trophozoites with pseudopodia and ingested RBC. [ 2+5+4+4=15 marks ] A] What is the provisional diagnosis. What is the likely pathogen. B] What is the pathogenesis. C] Describe the laboratory diagnosis. D] What is the treatment and prevention.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have all the information needed for a comprehensive, well-structured answer. Let me compile it.
Case Analysis: Bloody Diarrhea with Mucus, Trophozoites with Ingested RBCs
A] Provisional Diagnosis and Likely Pathogen [2 marks]
Provisional Diagnosis: Amoebic Dysentery (Intestinal Amoebiasis)
Likely Pathogen: Entamoeba histolytica
The clinical triad of:
- Bloody diarrhea with mucus (dysentery)
- Abdominal pain and fever
- Trophozoites with pseudopodia and ingested RBCs on stool microscopy
...is pathognomonic for E. histolytica infection. The finding of trophozoites containing ingested erythrocytes in their cytoplasm is the single most definitive diagnostic feature distinguishing E. histolytica from all other commensal intestinal amoebae (e.g., E. coli, E. dispar).
- Medical Microbiology 9e, p. 801
B] Pathogenesis [5 marks]
Life Cycle Overview
The infective form is the quadrinucleated cyst, transmitted via the fecal-oral route through contaminated water, food, or direct contact. Cysts resist gastric acid and pass to the duodenum, where excystation releases the pathogenic trophozoite.
Mechanism of Intestinal Invasion
-
Attachment: Trophozoites attach to colonic epithelial cells via a galactose-inhibitable adherence lectin (Gal/GalNAc lectin). This attachment is a prerequisite for cytolysis and tissue necrosis.
-
Cytolysis: Attachment is followed by a lethal alteration of host cell membrane permeability, causing an irreversible rise in intracellular calcium, leading to cell death. Colonic epithelial cells, neutrophils, lymphocytes, and monocytes are all lysed. Released toxic neutrophil constituents amplify tissue destruction.
-
Ulcer Formation: Trophozoites invade the intestinal mucosa, producing discrete ulcers with a pinhead-sized center and raised edges, from which mucus, necrotic cells, and amoebae are shed. Amebae multiply above the muscularis mucosae and spread laterally, undermining the mucosa and producing the characteristic "flask-shaped" ulcer - a narrow neck through the mucosa opening into an expanded necrotic area in the submucosa.
-
Spread: Coalescence of colonies can undermine large areas. Trophozoites may penetrate through the muscle layers and occasionally the serosa, causing perforation.
-
Extraintestinal spread: Trophozoites entering portal blood are carried to the liver (most common extraintestinal site), producing amoebic liver abscess containing characteristic "anchovy paste" (necrotic, bacteriologically sterile material). Less commonly, lungs, brain, and spleen may be involved.
-
Favored sites: Cecum, appendix, ascending colon (primary); sigmoid colon and rectum (later lesions). Occasionally a chronic granulomatous mass called an ameboma forms on the intestinal wall.
The basis for tissue destruction includes: (i) cytotoxin production, (ii) lectin-mediated adherence, and (iii) trophozoite-mediated lysis with secondary neutrophil-mediated injury.
- Medical Microbiology 9e, pp. 800-801; Jawetz Melnick & Adelberg's Medical Microbiology 28e, pp. 733-734
C] Laboratory Diagnosis [4 marks]
1. Microscopic Examination of Stool (Definitive)
The cornerstone of diagnosis. Three stool samples should be collected on alternate days to improve sensitivity (parasites are not homogeneously distributed).
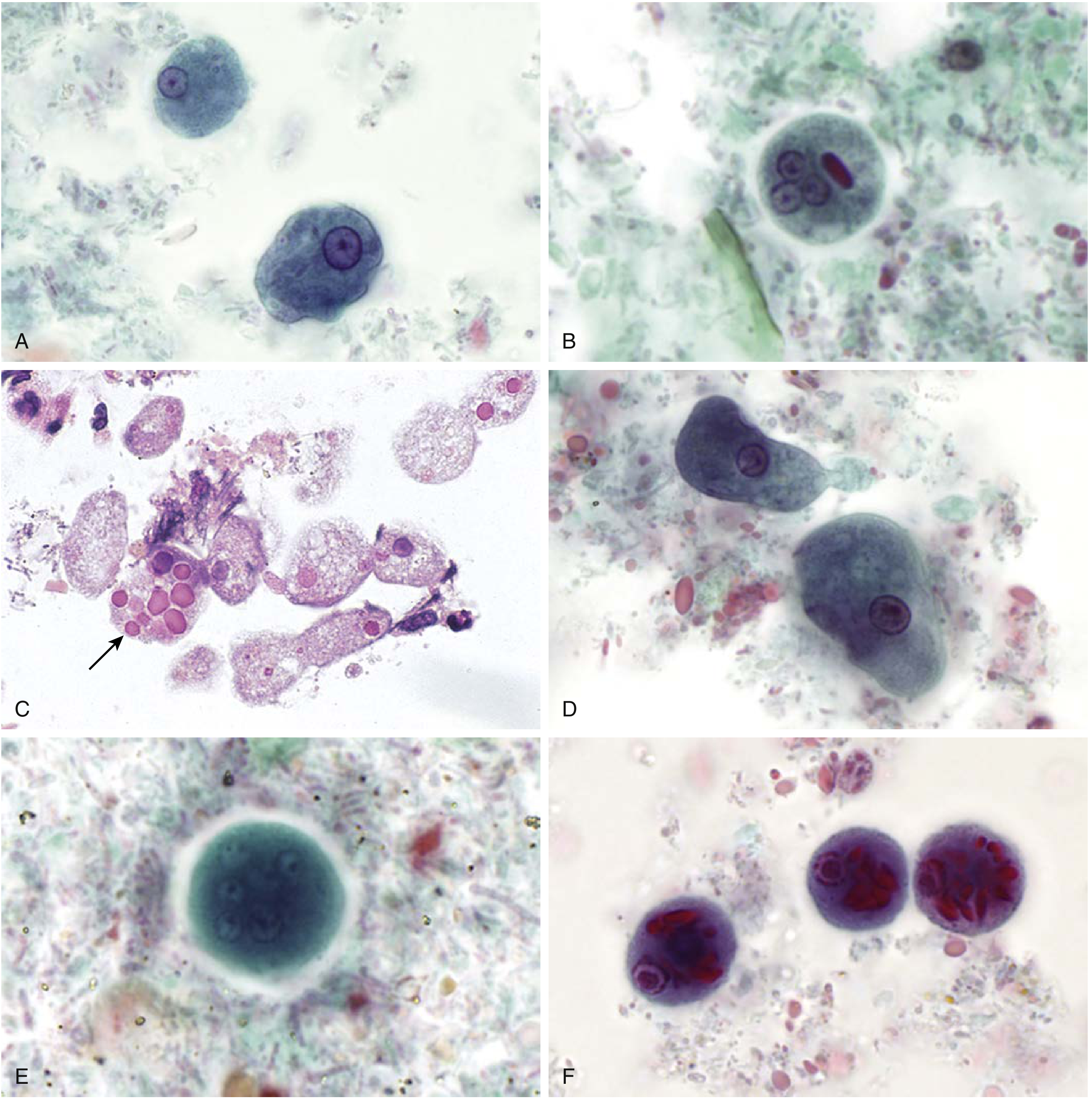
Figure: Trichrome-stained intestinal protozoa at 1000x. Panel C (arrow) shows E. histolytica trophozoites with ingested red blood cells from a colonic lesion - the pathognomonic finding in this case. - Henry's Clinical Diagnosis and Management by Laboratory Methods
Trophozoite features (found in liquid/diarrhoeic stools):
- Size: 12-50 μm
- Motile with unidirectional pseudopodia (directional movement distinguishes from non-pathogenic amoebae)
- Cytoplasm: hyaline outer ectoplasm, granular endoplasm
- Single nucleus with fine, evenly-distributed peripheral chromatin and a small, central karyosome
- Ingested RBCs in cytoplasm - pathognomonic
Cyst features (found in formed stools):
- Size: 10-20 μm
- 1-4 nuclei (mature cyst: 4 nuclei)
- Chromatoidal bars with bluntly rounded ends (vs. splintered ends in E. coli)
- May contain glycogen vacuole
Differentiation from E. coli:
| Feature | E. histolytica | E. coli |
|---|---|---|
| Peripheral chromatin | Fine, uniform, dispersed | Coarse, clumped |
| Karyosome | Central, sharp | Eccentric, coarse |
| Ingested RBCs | Present | Absent |
| Cyst nuclei | Up to 4 | Up to 8 |
| Chromatoidal bars | Rounded ends | Splintered/frayed ends |
2. Staining Methods
- Trichrome stain or iron-haematoxylin stain: for permanent smears, better nuclear detail
- Iodine wet mount: stains cysts (glycogen appears brown), nuclei visible
- Saline wet mount: shows motile trophozoites in fresh specimens
3. Concentration Techniques
- Formol-ether (formalin-ethyl acetate) sedimentation: concentrates cysts and eggs from formed stool
- Zinc sulphate flotation: for cyst recovery
4. Proctoscopy/Colonoscopy with Biopsy
- Reveals characteristic flask-shaped ulcers
- Biopsy of ulcer edges shows trophozoites on histopathology (H&E stain)
5. Antigen Detection (ELISA/EIA)
- Stool antigen tests detect E. histolytica-specific antigens
- Distinguishes E. histolytica from E. dispar (which is morphologically identical but non-pathogenic) - important since standard microscopy cannot differentiate these species
6. Serology (Indirect Haemagglutination, ELISA)
- Useful for extraintestinal amoebiasis (liver abscess), where stool microscopy is frequently negative
-
80% of intestinal disease cases are seropositive at clinical presentation
- Less useful in endemic areas (high background seropositivity)
7. PCR / DNA-Based Assays
- Most sensitive and specific; can differentiate E. histolytica from E. dispar, E. moshkovskii, and E. bangladeshi
- Used when morphological distinction is insufficient
8. Imaging (for Extraintestinal Disease)
-
Ultrasound, CT scan, MRI, or radionuclide scan for amoebic liver abscess
-
Aspirated "anchovy paste" (sterile, chocolate-brown pus) is characteristic; trophozoites are at the margins of the abscess wall, not in the necrotic center
-
Medical Microbiology 9e, pp. 801-802; Henry's Clinical Diagnosis and Management by Laboratory Methods, pp. 1518-1519
D] Treatment and Prevention [4 marks]
Treatment
Treatment depends on the clinical form:
| Clinical Form | Drug of Choice | Rationale |
|---|---|---|
| Acute/fulminating amoebic dysentery | Metronidazole 400-800 mg TDS x 5-10 days | Tissue amebicide - kills invasive trophozoites |
| Followed by (luminal amebicide) | Iodoquinol, diloxanide furoate, or paromomycin | Eradicates luminal cysts to prevent relapse |
| Asymptomatic cyst carrier | Iodoquinol, diloxanide furoate, or paromomycin alone | Luminal agent only needed |
| Amoebic liver abscess | Metronidazole + luminal agent | Percutaneous drainage if needed |
- Metronidazole is the drug of choice for invasive and extraintestinal disease; it is a tissue amebicide that is inadequate alone because it does not reliably eliminate luminal cysts.
- The subsequent luminal agent (diloxanide furoate / iodoquinol / paromomycin) is mandatory to prevent relapse and break the transmission cycle.
- Tinidazole or secnidazole are alternatives to metronidazole with similar efficacy.
Prevention
Individual level:
- Boil or treat drinking water (chlorination alone does not reliably kill cysts - filtration is also needed)
- Thoroughly wash and peel fruits and vegetables before consumption
- Avoid raw vegetables and salads in endemic areas
- Practice careful hand hygiene, especially after defecation and before food handling
- Travelers to endemic regions should be advised to avoid ice cubes, unpeeled fruits, and tap water
Community/Public Health level:
-
Introduce adequate sanitation infrastructure (sewage disposal, latrines)
-
Prevent use of human feces (night soil) as agricultural fertilizer
-
Safe water supply: chlorination + filtration of municipal water
-
Control of mechanical vectors (flies, cockroaches) that transport cysts
-
Identify and treat asymptomatic cyst carriers, especially in healthcare, food service, and institutional settings
-
Health education regarding fecal-oral transmission routes
-
Medical Microbiology 9e, p. 802; Jawetz Melnick & Adelberg's Medical Microbiology 28e, p. 834
Summary:
This 25-year-old male has amoebic dysentery caused by Entamoeba histolytica, confirmed by the pathognomonic finding of trophozoites with ingested RBCs. The pathogenesis involves lectin-mediated attachment, cytolysis, and flask-shaped mucosal ulceration. Diagnosis rests primarily on stool microscopy, supplemented by antigen detection or PCR to distinguish E. histolytica from E. dispar. Treatment requires metronidazole (tissue amebicide) followed by a luminal amebicide (diloxanide furoate/iodoquinol/paromomycin). Prevention centres on safe water, sanitation, and hygienic food practices.
This is a shared conversation. Sign in to Orris to start your own chat.