Meckel diverticulum full
Reading File
Finding Sources
Searching PubMed
"Meckel diverticulum"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a complete, authoritative answer. Here is the full review:
Meckel Diverticulum - Complete Review
Definition and Classification
Meckel diverticulum (MD) is the most common congenital anomaly of the gastrointestinal tract and the most common true diverticulum in the body. A true diverticulum contains all three layers of the bowel wall - mucosa, muscularis, and serosa - distinguishing it from acquired pseudodiverticula (e.g., colonic diverticula) which lack or have attenuated muscularis.
It accounts for approximately 67% of all omphalomesenteric duct remnants.
Embryology and Pathogenesis
During early gestation (weeks 5-7), the omphalomesenteric (vitelline) duct connects the fetal yolk sac to the primitive gut. By weeks 7-8, this duct is normally completely obliterated. Failure of involution produces a spectrum of anomalies:
| Remnant Type | Description |
|---|---|
| Meckel diverticulum (most common, ~67%) | Diverticular sac from ileum |
| Patent omphalomesenteric duct | Persistent ileum-to-umbilicus fistula (~6-15%) |
| Omphalomesenteric (vitelline) cyst | Mucosa-lined cystic mass within a fibrous cord |
| Omphalomesenteric band | Solid fibrous cord connecting ileum to umbilicus |
| Vitelline vessel remnant | Fibrous band derived from vitelline vessels |
Molecularly, aberrant expression of SOX2 (normally expressed in proximal primitive gut/gastric epithelium) and CDX2 (normally in posterior gut) may drive ectopic gastric tissue formation in the diverticulum. SOX2 is found expressed in the ectopic gastric tissue, while CDX2 is expressed in patches - suggesting aberrant SOX2 expression, not absence of CDX2, is the key driver.
Gross Pathology

Meckel diverticulum gross specimen: the blind pouch arises from the antimesenteric border of the ileum (Robbins Pathologic Basis of Disease, Fig. 17.2)
- Arises from the antimesenteric border of the ileum (vs. enteric duplication cysts, which form on the mesenteric border)
- Length: typically 1-10 cm; "giant" diverticula are those >5 cm
- Type I giant: long but same caliber as ileum
- Type II giant (ovoid): larger diameter
- May be connected to the umbilicus or mesentery by a fibrous band
The "Rule of 2s"
A classic mnemonic:
| Feature | Value |
|---|---|
| Prevalence | ~2% of population |
| Location | Within 2 feet (60 cm) of the ileocecal valve |
| Length | ~2 inches (5 cm) |
| Male:Female ratio | 2:1 (some sources cite 3:1) |
| Age of symptoms | Most symptomatic by age 2 |
| Symptomatic rate | Only ~2-4% are ever symptomatic |
| 50% of symptomatic patients present before age 2 |
Histology / Ectopic Tissue
- Normal mucosa resembles small intestine
- Heterotopic (ectopic) tissue present in ~50% of all diverticula (some series report 27-50%)
- Gastric mucosa = most common ectopic tissue (80-85% of all ectopic tissue in MD); found in 24-70% of symptomatic MD in one meta-analysis
- Pancreatic tissue = second most common; colonic, Brunner glands, biliary, hepatic, jejunal tissue also rarely described
- Presence of ectopic tissue correlates with increased risk of symptomatic/complicated disease
- The ectopic gastric mucosa secretes acid → peptic ulceration of adjacent ileal mucosa ("marginal ulcer" at the gastric-ileal mucosal junction) → bleeding
Epidemiology
- Prevalence: 1.2-4% of the general population (large autopsy series: 2-3%)
- Males are 2-3x more commonly symptomatic than females
- Lifetime risk of complications: ~4-6%
- Risk of complications decreases dramatically with age
- Most adults with MD remain asymptomatic; incidental diagnosis is common
Clinical Presentations and Complications
1. Painless Rectal Bleeding (most common in children)
- Most common complication in pediatric patients, especially infancy to age 5
- Blood is typically maroon/brick-red (even with massive bleeding)
- Rarely BRBPR (like left colon); may present as melena with slower bleeding
- Mechanism: acid from ectopic gastric mucosa → marginal ulcer at gastric-ileal interface
- Despite massive bleeding, death is uncommon in children - hypovolemia causes splanchnic vasoconstriction, reducing blood flow
- H. pylori has been observed in diverticular gastric mucosa but its role in bleeding is considered unlikely
2. Intestinal Obstruction (most common in adults)
- Mechanisms:
- Intussusception with MD as the lead point (in children >4 years, intussusception is almost always secondary to MD)
- Volvulus around a persistent fibrous vitelline cord remnant
- Herniation through a fibrous band
- Entrapment in an inguinal, femoral, or umbilical hernia = Littre hernia
- Diverticular lithiasis - an enterolith from the diverticulum migrates into the distal ileum, causing obstruction or provoking inflammation
- Presents with bilious vomiting and abdominal distension
- Volvulus around a vitelline cord can occur in neonates
3. Meckel Diverticulitis
- Acute inflammation of the diverticulum
- Mimics acute appendicitis clinically - diagnosis often made at exploratory laparotomy
- Perforation in ~1/3 of cases (may result from peptic ulceration)
- Chronic form = Meckel ileitis, can mimic Crohn disease of the ileum
- More common in older adults; accounts for up to 20% of complications
4. Neoplasms (rare, mainly adults)
- Carcinoid tumors - most common neoplasm; typically small, resembling jejunoileal carcinoids (not appendiceal) in immunohistochemical characteristics and metastatic potential; patients usually in their 6th decade, often asymptomatic
- Adenocarcinoma - very rare
- Sarcoma - very rare
- Neoplasms do not occur in childhood
Summary by Age Group
| Age Group | Most Common Complication |
|---|---|
| Children (<5 years) | Painless GI bleeding |
| Children (>4 years) | Intussusception |
| Adults | Intestinal obstruction |
| Older adults | Meckel diverticulitis (~20% of complications) |
Diagnosis
1. Meckel (Technetium-99m Pertechnetate) Scan - Meckel Scan
- Investigation of choice for suspected bleeding MD
- Sensitivity: 80-90%, Specificity: ~95% in children
- 99mTc-pertechnetate is taken up and secreted by gastric mucosa (normal and ectopic); surface mucus cells of stomach and heterotopic gastric tissue in MD concentrate this anion
- Enhancement techniques to improve sensitivity:
- Cimetidine (H2 blocker): reduces anion secretion from gastric mucosa, increasing intracellular retention and improving visualization
- Pentagastrin: increases anion uptake (mechanism unclear)
- Glucagon: reduces peristalsis, decreasing washout artifact
- Limitation: requires ectopic gastric mucosa for a true positive; false-positive and false-negative rates are high in adults
- False positives: Crohn's disease, other inflammatory bowel disorders, intussusception, bowel duplication, urinary tract pathology
2. CT Scan / CT Enterography
- MD appears as a tubular blind-ending structure arising from the antimesenteric border of the terminal ileum
- May be mistaken for a normal bowel loop
- CT enterography improves detection sensitivity significantly
- Useful for diagnosing obstruction or peritonitis, though the diverticulum itself is often difficult to identify
3. Plain Abdominal Radiograph
- Rarely diagnostic
- May show: dilated bowel loops with gas-fluid levels (in obstruction), a saccular soft-tissue shadow in the mid-abdomen (see image below), enterolith (may be indistinguishable from appendicolith)
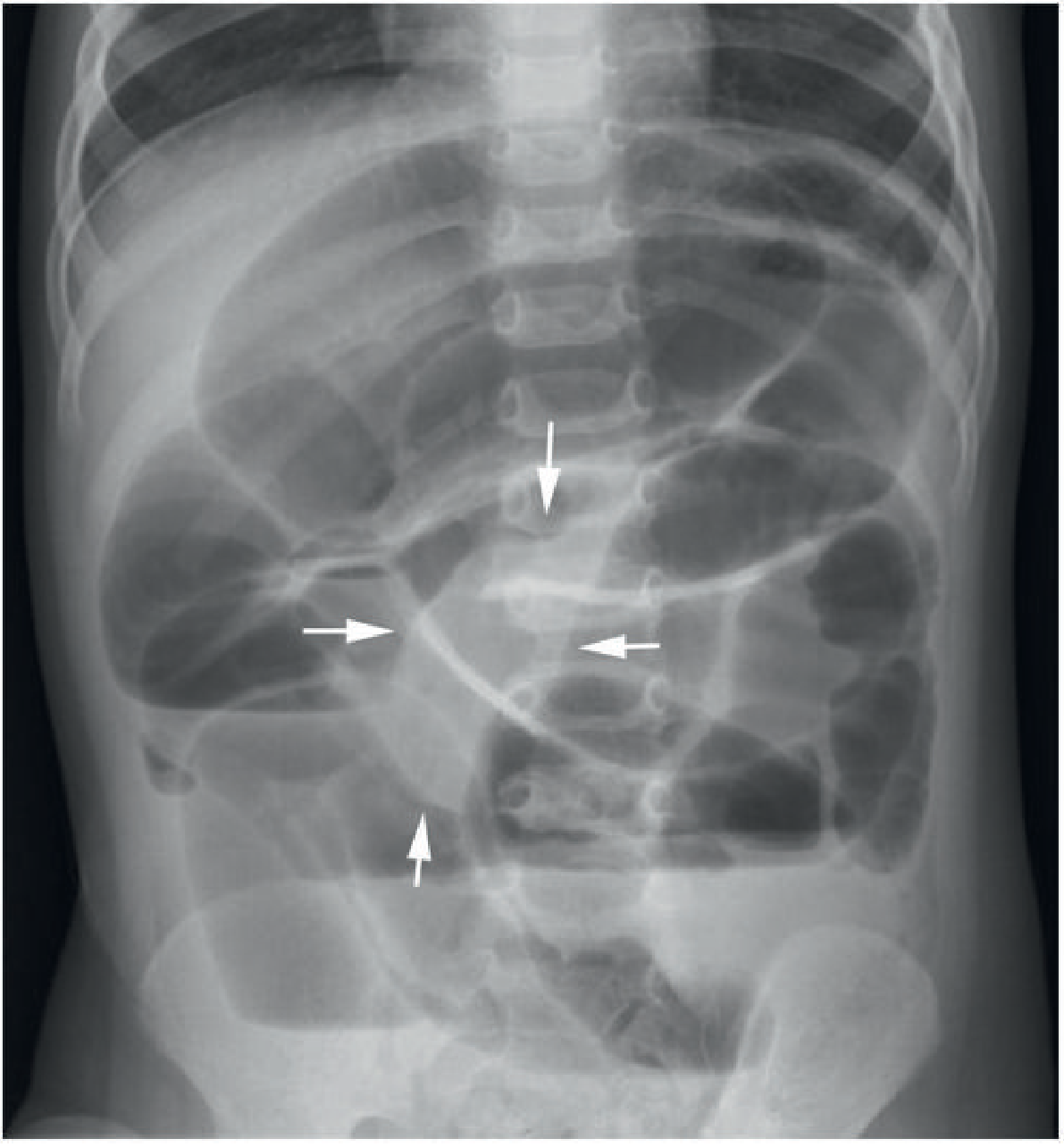
Fig: Plain abdominal radiograph in a 2-year-old with Meckel diverticulitis and peritonitis, showing dilated bowel loops, gas-fluid levels, and saccular soft-tissue shadow (arrows) - Grainger & Allison's Diagnostic Radiology
4. Barium Studies
- Small bowel follow-through: usually not useful - MD may not fill with barium and empties rapidly
- Enteroclysis: better than follow-through; contrast under pressure fills the diverticulum
- Characteristic barium appearance: saccular blind-ending pouch on antimesenteric border with a triradiate fold pattern converging with the ileum
- Useful for chronic persistent symptoms when cross-sectional and nuclear medicine imaging are negative
5. Angiography
- Useful when bleeding is present and Meckel scan is negative
- Localizes source of hemorrhage
- Can demonstrate the vitelline artery (arising from a distal branch of the SMA) and its characteristic blush of tortuous small vessels
- Note: the vitelline artery frequently involutes; the diverticulum is then supplied by branches directly from the SMA
6. Radiolabeled RBC Scan (99mTc-labeled red blood cells)
- Used when Meckel scan is negative and diagnosis is still suspected
- Localizes active bleeding site
7. Capsule Endoscopy
- Small bowel video capsule endoscopy can successfully detect MD
- A 2025 systematic review (PMID: 40202427) catalogued cases discovered by capsule endoscopy
8. Double Balloon Enteroscopy
- Retrograde approach useful for obscure GI bleeding due to MD, particularly when the lesion is close to the ileocecal valve
- Challenging when the lesion is far from the ileocecal valve
9. MR Enterography
- Can be considered to localize the lesion when other modalities are inconclusive, especially for lesions far from the ileocecal valve
10. Ultrasound
- Rarely diagnostic; intussusception caused by MD may be identified on US
- Not a first-line test
Management
Symptomatic / Complicated MD
- Surgical treatment is mandatory for bleeding, obstruction, or perforation
- Diverticulectomy is the standard operation
- Concurrent ileal resection is added if adjacent small bowel is ulcerated, inflamed, obstructed, or if the diverticulum base is wide or involved
- Laparoscopic removal is a well-reported and accepted approach
- Postoperative morbidity occurs in up to 6% of cases
Incidentally Discovered / Asymptomatic MD
- Management is controversial
- Many experts do not recommend prophylactic removal in adults given the low lifetime complication risk (~4-6%)
- Factors favoring resection of asymptomatic MD:
- Diverticulum >2 cm in length
- Associated omphalomesenteric band (risk of volvulus/obstruction)
- Palpable mass within the diverticulum (suggests tumor or ectopic mucosa)
- Younger male patients
- Some surgeons routinely search for and resect MD during appendectomy or laparotomy for acute abdomen
Littre Hernia
A special complication: MD is entrapped in an inguinal, femoral, or umbilical hernia sac = Littre hernia. The patient presents with typical hernia symptoms. Management is surgical reduction and diverticulectomy.
Differential Diagnosis (Pediatric GI Bleeding)
- Red dyes in food/drinks (false hematochezia)
- Bismuth subsalicylate, iron, spinach (false melena)
- Upper GI source with rapid transit (in young children can cause hematochezia)
- Intussusception (other causes)
- Intestinal polyps
- Inflammatory bowel disease (especially if chronic)
- Appendicitis (for pain presentations)
Key Summary Table
| Feature | Details |
|---|---|
| Type | True diverticulum (all 3 wall layers) |
| Location | Antimesenteric border of ileum, within 60 cm of IC valve |
| Origin | Failed involution of vitelline/omphalomesenteric duct |
| Prevalence | 2% of population |
| Male predominance | 2-3:1 |
| Ectopic tissue | ~50%; gastric mucosa 80-85% |
| Most common complication (children) | Painless rectal bleeding |
| Most common complication (adults) | Intestinal obstruction |
| Best diagnostic test (bleeding) | Meckel scan (99mTc pertechnetate) |
| Treatment | Diverticulectomy ± ileal resection |
| Special hernia | Littre hernia (MD in hernia sac) |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Yamada's Textbook of Gastroenterology, 7th ed.
- Grainger & Allison's Diagnostic Radiology
- Rosen's Emergency Medicine
Recent literature: Two 2025 systematic reviews are available - PMID 40202427 on capsule endoscopy detection of MD, and PMID 40696289 on sonographic features of axial torsion of MD in pediatric patients - these do not contradict the above standard guidelines.
Write it for 10 marks ans
Meckel Diverticulum — 10 Marks Answer
Definition
Meckel diverticulum is the most common congenital anomaly of the gastrointestinal tract and the most common true diverticulum (containing all three layers of the bowel wall - mucosa, muscularis propria, and serosa). It results from failed involution of the omphalomesenteric (vitelline) duct, which normally connects the yolk sac to the primitive gut and obliterates by 7-8 weeks of gestation.
Rule of 2s
| Feature | Value |
|---|---|
| Prevalence | 2% of population |
| Distance from ileocecal valve | Within 2 feet (60 cm) |
| Length | ~2 inches (5 cm) |
| Male : Female ratio | 2:1 |
| Age of symptomatic presentation | Most by age 2 |
| Symptomatic rate | Only ~2% ever symptomatic |
Anatomy
- Arises from the antimesenteric border of the ileum
- Contains ectopic tissue in ~50% of cases
- Ectopic gastric mucosa = 80-85% of all ectopic tissue
- Pancreatic tissue = second most common
- Ectopic gastric mucosa secretes acid → peptic ulceration of adjacent ileal mucosa ("marginal ulcer") → bleeding
Complications (Clinical Features)
1. Painless Rectal Bleeding
- Most common complication in children (especially <5 years)
- Blood is typically maroon/brick-red; melena may occur with slower bleeding
- Due to acid secretion by ectopic gastric mucosa → marginal ulceration
- Despite massive bleeding, death is uncommon in children (splanchnic vasoconstriction limits blood loss)
2. Intestinal Obstruction
- Most common complication in adults
- Mechanisms:
- Intussusception (MD acts as lead point - in children >4 years, nearly all intussusceptions are secondary to MD)
- Volvulus around a persistent fibrous vitelline cord
- Littre hernia - MD trapped in an inguinal/femoral/umbilical hernia sac
- Diverticular lithiasis (enterolith causing obstruction)
- Presents with bilious vomiting and abdominal distension
3. Meckel Diverticulitis
- Acute inflammation mimicking acute appendicitis - diagnosis usually made at laparotomy
- Perforation occurs in ~1/3 of cases
- Chronic form (Meckel ileitis) can mimic Crohn disease
- More common in older adults (~20% of complications)
4. Neoplasms (rare)
- Carcinoid tumor (most common), adenocarcinoma, sarcoma
- Mainly in adults; do not occur in childhood
Investigations
Meckel (Technetium-99m Pertechnetate) Scan — Investigation of Choice
- 99mTc pertechnetate is taken up by ectopic gastric mucosa
- Sensitivity 80-90%, Specificity ~95% in children
- Sensitivity enhanced by:
- Cimetidine (H2 blocker) - reduces anion secretion, improves retention
- Pentagastrin - enhances uptake
- Limitation: requires ectopic gastric mucosa; less reliable in adults
Other Investigations
| Investigation | Role |
|---|---|
| CT/CT enterography | Tubular blind-ending structure on antimesenteric border; useful for obstruction/peritonitis |
| Angiography | Active bleeding; demonstrates vitelline artery (branch of SMA) |
| 99mTc-labeled RBC scan | Localizes active bleeding when Meckel scan negative |
| Capsule endoscopy | Useful for obscure GI bleeding |
| Double-balloon enteroscopy | Retrograde approach for lesions near ileocecal valve |
| Barium studies (enteroclysis) | Blind-ending saccular pouch with triradiate folds; used when above negative |
Management
Symptomatic / Complicated MD
- Surgical treatment is the only definitive therapy
- Diverticulectomy - standard operation
- Diverticulectomy + ileal resection - if adjacent bowel is ulcerated, inflamed, or the base is wide
- Laparoscopic approach is well established
Asymptomatic / Incidentally Found MD
- Management is controversial; prophylactic resection is generally not recommended in adults
- Resection favored if:
- Length >2 cm
- Associated fibrous omphalomesenteric band (volvulus risk)
- Palpable mass within the diverticulum
- Young male patient
Summary
Meckel diverticulum is a true ileal diverticulum arising from incomplete regression of the vitelline duct. Summarized by the Rule of 2s, it is most often asymptomatic but can present with painless rectal bleeding in children and intestinal obstruction in adults. Ectopic gastric mucosa is central to the pathogenesis of bleeding. The Meckel scan is the investigation of choice. Treatment is surgical diverticulectomy.
This is a shared conversation. Sign in to Orris to start your own chat.