What is multi myeloma,,
Reading File
Finding Sources
Searching PubMed
"multiple myeloma"[MeSH Terms] AND diagnosis
Reading File
Reading File
Reading File
Finding Sources
Searching Images
multiple myeloma bone marrow plasma cells histology
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer.
Multiple Myeloma
Definition
Multiple myeloma (MM) is a malignancy of plasma cells characterized by infiltration of the bone marrow with clonal plasma cells, resulting in widespread skeletal destruction, anemia, renal dysfunction, and immunodeficiency. It is defined by the presence of ≥10% clonal plasma cells on bone marrow examination, an M protein in serum or urine, and evidence of one or more myeloma-defining events (see Diagnosis below).
— Goldman-Cecil Medicine, p. 1977
Epidemiology
- Accounts for ~1% of all malignancies and >10% of hematologic malignancies
- ~30,000 new cases/year in the United States
- Median age at diagnosis: 65–70 years; only 2% of patients are <40
- More common in males and in people of African descent (Black Americans have nearly twice the incidence of White Americans)
- Almost all cases evolve from a premalignant MGUS (monoclonal gammopathy of undetermined significance) phase
— Goldman-Cecil Medicine, p. 1977–1978 | Robbins & Kumar Basic Pathology, p. 421
Pathogenesis
Genetic Events
- Primary IgH translocations (chromosome 14q32) occur in ~40% of cases, fusing the IgH locus to oncogenes such as cyclin D1 and cyclin D3 — dysregulation of D-cyclins drives cell proliferation
- Hyperdiploid myeloma (trisomies) accounts for another ~40%
- Progression from MGUS → myeloma is driven by RAS mutations and MYC abnormalities; secondary events include deletion 17p, deletion 1p, and amplification 1q (all adverse prognostic markers)
Bone Marrow Microenvironment
- The cytokine IL-6 (produced by bone marrow fibroblasts and macrophages) is a major growth factor for myeloma plasma cells
- NF-κB signaling and other paracrine loops (SDF-α, MIP-1-α) sustain tumor growth
Bone Destruction Mechanism
Myeloma plasma cells cause pure osteolytic disease via two complementary mechanisms:
- Osteoclast activation: Myeloma cells upregulate RANKL and decrease OPG (osteoprotegerin) → increased RANKL/OPG ratio → osteoclast activation → bone resorption
- Osteoblast suppression: Elevated IL-3, IL-7, and DKK1 simultaneously suppress bone formation
The net result is hypercalcemia, pathologic fractures, and bone pain.
— Goldman-Cecil Medicine, p. 1978 | Robbins & Kumar, p. 421
Clinical Manifestations ("CRAB" Criteria)
| Feature | Details |
|---|---|
| C – Hypercalcemia | From osteoclast-driven bone resorption; causes confusion, polyuria, constipation, weakness |
| R – Renal insufficiency | Cast nephropathy (Bence Jones proteins), light chain deposition, amyloid, hypercalcemia-induced dehydration |
| A – Anemia | Marrow infiltration + suppression of normal hematopoiesis |
| B – Bone disease | Lytic "punched-out" lesions, vertebral fractures, bone pain (the most common presenting symptom) |
Additional features:
- Recurrent bacterial infections — myeloma suppresses normal B-cell function; despite elevated total immunoglobulin (from M protein), functional antibody production is severely depressed
- Hyperviscosity (less common) — from high levels of circulating M protein
- Peripheral neuropathy — especially with AL amyloid
- Many patients are initially asymptomatic, detected incidentally on blood tests
Bone Marrow Histology
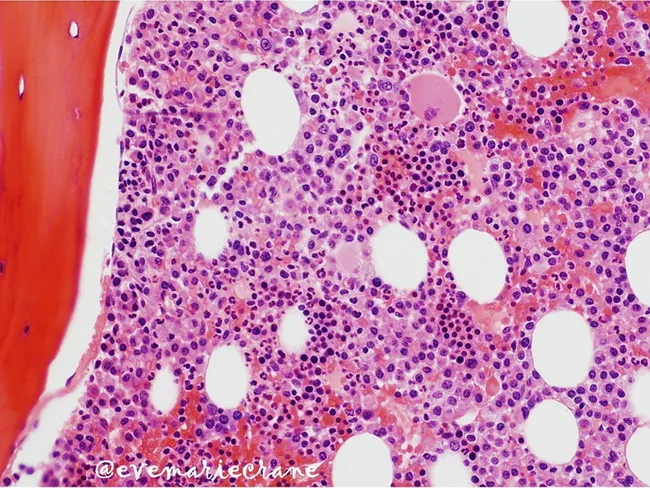
Bone marrow biopsy (H&E): Clonal plasma cells (~50% of nucleated cells) with hyperchromatic eccentric nuclei, clumped chromatin, and moderate cytoplasm, replacing normal hematopoietic elements
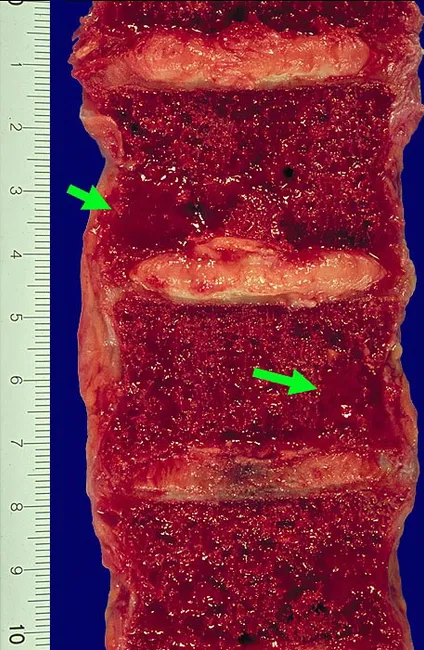
Gross specimen: Vertebral bodies with lytic myeloma lesions (green arrows) — gelatinous red-brown tumor replacing marrow and thinning cortical bone
Microscopic features:
- Marrow plasma cells usually >30% of cellularity at diagnosis
- Cells may resemble normal plasma cells or show abnormal features: prominent nucleoli, Russell bodies (cytoplasmic inclusions of condensed immunoglobulin)
- Skeletal lesions: "punched-out" lytic defects 1–4 cm, most common in vertebral column, ribs, skull, pelvis, femur
— Robbins & Kumar, p. 422
M Protein (Paraprotein) Types
| Ig Type | Frequency |
|---|---|
| IgG | ~60% |
| IgA | 20–25% |
| Light chain only (κ or λ) | ~15% |
| IgM, IgD, IgE | Rare |
| Non-secretory | <5% |
Diagnosis
International Myeloma Working Group Criteria — requires all three:
- ≥10% clonal plasma cells on bone marrow biopsy OR biopsy-proven plasmacytoma
- M protein in serum or urine (absent in non-secretory myeloma)
- One or more myeloma-defining events:
- Hypercalcemia (>11 mg/dL)
- Renal insufficiency (creatinine >2 mg/dL or CrCl <40 mL/min)
- Anemia (Hb <10 g/dL or >2 g/dL below normal)
- Bone lesions (≥1 lytic lesion on skeletal survey, CT, or PET-CT)
- Clonal BM plasma cells ≥60%
- Serum free light chain ratio ≥100
-
1 focal lesion on MRI
Key workup: Serum and urine protein electrophoresis (SPEP/UPEP), serum free light chains, bone marrow biopsy, skeletal survey or whole-body low-dose CT/PET-CT, CBC, CMP (creatinine, calcium), β2-microglobulin, LDH, cytogenetics/FISH.
Staging (Revised ISS)
| Stage | Criteria | Median Survival |
|---|---|---|
| I | β2-microglobulin <3.5 mg/L + albumin ≥3.5 g/dL; standard-risk cytogenetics; normal LDH | ~62 months |
| II | Neither Stage I nor III | ~44 months |
| III | β2-microglobulin ≥5.5 mg/L + high-risk cytogenetics (del17p, t(4;14), t(14;16)) or high LDH | ~29 months |
Treatment
Transplant-Eligible Patients (~50% of newly diagnosed)
- Induction (~3–4 months): VRd (bortezomib + lenalidomide + dexamethasone) is the standard; daratumumab can be added (DaraVRd) for high-risk disease
- Autologous stem cell transplantation (ASCT) with high-dose melphalan — prolongs event-free and overall survival (not curative)
- Maintenance therapy with lenalidomide post-transplant
Transplant-Ineligible Patients
- DRd (daratumumab + lenalidomide + dexamethasone) or VRd at attenuated doses
- Bortezomib + melphalan + prednisone (VMP) is an alternative
Relapsed/Refractory Myeloma
- Multiple salvage regimens combining proteasome inhibitors (bortezomib, carfilzomib, ixazomib), immunomodulatory agents (lenalidomide, pomalidomide), anti-CD38 monoclonals (daratumumab, isatuximab), anti-BCMA agents (belantamab, teclistamab, idecabtagene vicleucel CAR-T)
- Second ASCT may be considered if first remission lasted >1 year
Supportive Care
- Bisphosphonates (zoledronic acid, pamidronate) for bone disease
- G-CSF and antimicrobial prophylaxis for infections
- Radiation for painful or impending fracture lesions
- Treat hypercalcemia with hydration, bisphosphonates
— Goldman-Cecil Medicine, pp. 1979–1981
Prognosis
Median overall survival has improved dramatically with modern therapy — from ~3 years in the 1990s to >7–10 years for many patients with standard-risk disease. High-risk cytogenetics (del17p, t(4;14), t(14;16)) remain associated with shorter survival (~29 months median). Achieving minimal residual disease (MRD) negativity is strongly associated with superior outcomes (PMID 38768337).
Differentiation from Related Disorders
| Entity | Plasma Cells | M Protein | End-organ damage |
|---|---|---|---|
| MGUS | <10% | <3 g/dL | None |
| Smoldering MM | 10–60% | ≥3 g/dL (serum) or ≥500 mg/24h (urine) | None |
| Multiple Myeloma | ≥10% | Any level | Present (CRAB or myeloma-defining event) |
| Solitary plasmacytoma | Single lesion, no systemic involvement | Usually absent | Local only |
Sources: Robbins & Kumar Basic Pathology, p. 421–422 | Goldman-Cecil Medicine, pp. 1977–1981 | Washington Manual of Medical Therapeutics, p. 821
Symptoms , treatment , what to food to take to reduce , is it dangerous
Checking Date & Time
Finding Sources
Finding Sources
Searching PubMed
"multiple myeloma" AND diet AND nutrition
Reading File
Reading File
Reading Article
PMID: 41342739
I have all the information needed. Here is a comprehensive answer:
Multiple Myeloma: Symptoms, Treatment, Diet & Danger
1. Symptoms
Multiple myeloma is often called "CRAB" — a simple way to remember its main symptoms:
🦀 C — Calcium (High blood calcium / Hypercalcemia)
- Confusion, memory problems
- Excessive thirst and urination
- Constipation
- Nausea and loss of appetite
- Extreme fatigue and weakness
🦀 R — Renal (Kidney problems)
- Swelling in the legs
- Reduced urine output
- Fatigue from waste build-up in the blood
🦀 A — Anemia (Low red blood cells)
- Fatigue and weakness
- Shortness of breath
- Dizziness
- Pale skin
🦀 B — Bone problems
- Bone pain — most common first symptom (back, ribs, sternum/breastbone, skull, hips)
- Pathologic fractures (broken bones from minor injury)
- Vertebral collapse → back pain or height loss
Other important symptoms
| Symptom | Cause |
|---|---|
| Recurrent infections (pneumonia, etc.) | Weakened immune system |
| Weakness, fatigue, depression | Anemia + systemic illness |
| Numbness/tingling in hands/feet | Nerve compression or amyloid deposits |
| Hearing loss, vertigo (rare) | Myeloma deposits in skull/temporal bone |
Important: Many people have no symptoms at all early on — the disease is discovered incidentally on routine blood tests.
— Swanson's Family Medicine Review | Cummings Otolaryngology, p. 2912
2. Treatment
Treatment has improved dramatically and is chosen based on age, fitness, and disease features.
Step 1 — Induction Chemotherapy (All patients)
The standard first-line regimen is VRd:
- V — Bortezomib (Velcade) — a proteasome inhibitor
- R — Lenalidomide (Revlimid) — an immunomodulatory drug
- d — Dexamethasone — a steroid
Daratumumab (an antibody targeting CD38 on myeloma cells) is increasingly added to this for high-risk disease.
Step 2 — Stem Cell Transplant (Eligible patients ~50%)
- Autologous stem cell transplantation (ASCT): Patient's own stem cells are collected, then high-dose chemotherapy (melphalan) destroys the myeloma, and the stem cells are returned to rebuild the bone marrow
- Not a cure, but significantly extends survival
- Suitable for patients under ~65–70 with good overall health
Step 3 — Maintenance Therapy
- Lenalidomide taken long-term after transplant to keep myeloma in remission
For patients NOT eligible for transplant
- Daratumumab + Lenalidomide + Dexamethasone (DRd)
- Bortezomib + Melphalan + Prednisone (VMP)
Supportive treatments (equally important)
| Problem | Treatment |
|---|---|
| Bone disease | Zoledronic acid (bisphosphonate) — protects bones |
| Pain / fractures | Radiation therapy to specific lesions |
| Anemia | Erythropoietin injections, blood transfusions |
| Infections | Antibiotics, antiviral prophylaxis, vaccines |
| Kidney disease | Hydration, avoid NSAIDs and contrast dye |
| Hypercalcemia | IV fluids + bisphosphonates |
Newer/Advanced treatments (relapsed disease)
- CAR-T cell therapy (e.g., idecabtagene vicleucel) — reprograms immune cells to kill myeloma
- Bispecific antibodies (teclistamab, elranatamab) — newer immunotherapy
- Carfilzomib, pomalidomide, isatuximab — for resistant disease
— Goldman-Cecil Medicine, pp. 1979–1981
3. Foods to Help (Dietary Guidance)
Important caveat: There is no food that cures or directly "treats" multiple myeloma. However, diet plays a meaningful supporting role in:
- Reducing inflammation (which drives myeloma progression)
- Supporting the immune system
- Maintaining weight and strength during treatment
- Potentially slowing progression in early/precursor stages
Foods to INCLUDE ✅
| Food Group | Examples | Why |
|---|---|---|
| High-fiber vegetables | Broccoli, spinach, kale, cabbage, Brussels sprouts | Reduce inflammation, support gut microbiome |
| Fruits | Berries (blueberries, strawberries), pomegranate, citrus | Rich in antioxidants, anti-inflammatory |
| Legumes & beans | Lentils, chickpeas, kidney beans | High fiber — feeds gut bacteria that suppress tumor growth |
| Whole grains | Oats, brown rice, barley, quinoa | Reduce insulin resistance (a myeloma risk factor) |
| Fatty fish | Salmon, sardines, mackerel | Omega-3s reduce inflammation |
| Turmeric | Curcumin (active ingredient) | Anti-inflammatory; studied in myeloma precursor states |
| Green tea | EGCG compounds | Antioxidant, some anti-myeloma cell activity in lab studies |
| Nuts & seeds | Walnuts, flaxseed, almonds | Healthy fats, anti-inflammatory |
A 2026 clinical trial (NUTRIVENTION) found that a high-fiber, plant-based diet in patients with myeloma precursor states (MGUS/smoldering myeloma) improved gut microbiome diversity, reduced inflammation, reduced insulin resistance, and may delay progression to full myeloma — independent of weight loss. [PMID: 41342739]
Foods to LIMIT or AVOID ❌
| Food | Reason |
|---|---|
| Red and processed meat | Pro-inflammatory, high purine content |
| Sugary drinks and processed sugar | Increases insulin resistance, promotes inflammation |
| Alcohol | Toxic to kidneys (already at risk in myeloma) |
| High-purine foods (organ meats, anchovies) | Can worsen kidney problems and gout |
| High-sodium/salty foods | Worsens fluid retention and kidney strain |
| High-calcium supplements (in excess) | Can worsen already elevated calcium levels |
Special dietary concerns during treatment
- During chemotherapy: Eat small, frequent meals; prioritize protein (eggs, fish, poultry, legumes) to maintain muscle mass
- Kidney disease: Limit potassium and phosphorus if told by your doctor (bananas, dairy, nuts may need restriction)
- Hydration: Drink plenty of water (2–3 liters/day unless restricted) — critical for kidney protection
Always consult a registered dietitian who specializes in oncology, as dietary needs vary by individual and treatment phase.
4. Is It Dangerous?
Yes — multiple myeloma is a serious, life-threatening cancer, but it is also manageable and treatable, with many patients living much longer than in previous decades.
Why it is dangerous
- It is not curable with current standard therapy (except in rare cases with allogeneic transplant)
- It progressively destroys bones, kidneys, and the immune system
- Renal failure, severe infections, and pathologic fractures are common causes of death
- It tends to relapse — even after treatment, the disease comes back
Survival has improved dramatically
| Era | Median Survival |
|---|---|
| 1990s (melphalan + steroids only) | ~3 years |
| 2000s (thalidomide, bortezomib era) | 4–5 years |
| Today (modern triplet/quadruplet therapy) | 7–10+ years for standard-risk patients |
Factors that affect outcome
| Better prognosis | Worse prognosis |
|---|---|
| Standard-risk cytogenetics | Deletion 17p, t(4;14), t(14;16) |
| Age <65, fit for transplant | Older age, multiple comorbidities |
| MRD (minimal residual disease) negativity | High β2-microglobulin, low albumin |
| Good kidney function at diagnosis | Renal failure at presentation |
Key message
Multiple myeloma is serious, but it is not an immediate death sentence. With modern treatment, many patients:
- Achieve complete remission
- Live 10+ years with good quality of life
- Some younger patients with early detection may live 15–20 years
The key is early diagnosis, prompt treatment, and regular monitoring.
Sources: Goldman-Cecil Medicine, pp. 1977–1981 | Swanson's Family Medicine Review, p. 347 | Cummings Otolaryngology, p. 2912 | Robbins & Kumar Basic Pathology, p. 421 | NUTRIVENTION Trial, Cancer Discovery 2026 [PMID: 41342739]
Can a 20 year old boy reduce the risk of it with proper protocols
Checking Date & Time
Finding Sources
Searching PubMed
"multiple myeloma" AND "risk factors" AND prevention
Reading File
Finding Sources
Great — I have everything needed for a thorough, honest answer.
Can a 20-Year-Old Reduce the Risk of Multiple Myeloma?
First — the honest picture
At 20, your baseline risk of multiple myeloma is extremely low. Only 2% of all myeloma patients are under 40, and the disease is primarily one of people aged 65+. You are not in a high-risk age group.
That said, the habits you build in your 20s directly shape your health decades later. Myeloma almost always develops from a precursor state called MGUS (monoclonal gammopathy of undetermined significance), and several lifestyle factors influence whether MGUS develops and whether it progresses. So yes — smart protocols today can meaningfully reduce long-term risk.
What Actually Causes Myeloma (Risk Factors)
Understanding the risks helps you know what to address:
| Risk Factor | Modifiable? |
|---|---|
| Older age (median 65–70 years) | ❌ No |
| Black/African descent | ❌ No |
| Male sex | ❌ No |
| Family history (first-degree relatives) | ❌ No — screen only |
| Obesity / high BMI | ✅ Yes |
| Insulin resistance | ✅ Yes |
| Chronic inflammation | ✅ Yes |
| Exposure to benzene, organic solvents, herbicides, insecticides, radiation | ✅ Yes — avoidable |
| Sedentary lifestyle | ✅ Yes |
| Western diet (high sugar, processed food) | ✅ Yes |
| Smoking | ✅ Yes (associated with blood cancers generally) |
— Goldman-Cecil Medicine, p. 1978 | Tintinalli's Emergency Medicine
Protocols a 20-Year-Old Can Follow
🏋️ 1. Maintain a Healthy Body Weight
This is the single most impactful modifiable risk factor.
- Obesity increases myeloma risk by 1.5–3× relative risk through:
- Hyperinsulinemia / insulin resistance — stimulates plasma cell growth factors including IGF-1
- Chronic low-grade inflammation — promotes the MGUS → myeloma progression
- Disrupted sex hormone levels
- Maintaining a BMI of 18.5–24.9 and avoiding abdominal fat accumulation is protective
A 2026 clinical trial (NUTRIVENTION) showed that reducing BMI and insulin resistance in people with myeloma precursor states slowed disease progression — these same mechanisms apply preventively in healthy young people. [PMID: 41342739]
🥗 2. Eat a High-Fiber, Anti-Inflammatory Diet
| Eat More | Eat Less |
|---|---|
| Vegetables (broccoli, spinach, kale, cabbage) | Red and processed meats |
| Fruits (berries, citrus, pomegranate) | Ultra-processed foods, fast food |
| Legumes (lentils, beans, chickpeas) | Sugary drinks, refined carbs |
| Whole grains (oats, brown rice, quinoa) | Excess alcohol |
| Fatty fish (salmon, sardines) | Fried foods |
| Nuts and seeds | Excess calories |
| Turmeric, green tea |
The NUTRIVENTION trial specifically showed that a high-fiber, plant-based diet improves gut microbiome diversity, reduces inflammation markers, and boosts anti-tumor immunity — independent of weight loss. Fiber produces short-chain fatty acids (SCFAs) in the gut that actively suppress tumor cell growth.
Goldman-Cecil recommends: "Eat a diet rich in whole grains, vegetables, fruits, and beans; limit fast foods, processed meats, and sugar-sweetened beverages" for general cancer prevention. — Goldman-Cecil Medicine, p. 1896
🏃 3. Exercise Regularly
- Physical activity reduces chronic inflammation, improves insulin sensitivity, and helps maintain healthy body weight — all directly relevant to myeloma risk
- Aim for: 150 minutes moderate aerobic activity/week + 2× strength training
- Resistance training specifically helps maintain muscle mass and metabolic health
🚭 4. Avoid Chemical Exposures
These are directly linked to myeloma risk and are avoidable:
- Benzene — found in gasoline, cigarette smoke, certain industrial solvents; avoid prolonged exposure
- Organic solvents — in paint thinners, dry cleaning chemicals, degreasers
- Herbicides and pesticides — use protective equipment if working with these; wash produce thoroughly
- Ionizing radiation — avoid unnecessary X-rays; follow "as low as reasonably achievable" (ALARA) principles
- Smoking — cigarette smoke is a benzene delivery system; do not smoke
— Goldman-Cecil Medicine, p. 1978
🍺 5. Limit or Avoid Alcohol
- Alcohol is associated with ~4% of cancers worldwide
- It promotes insulin resistance, increases inflammation, and disrupts immune surveillance
- If you do drink, keep it minimal
💤 6. Prioritize Sleep and Stress Management
- Chronic sleep deprivation and high cortisol (stress hormone) impair immune surveillance — the first line of defense against abnormal cell proliferation
- Aim for 7–9 hours of quality sleep per night
- Manage stress through exercise, mindfulness, social connection
🩺 7. Know Your Family History
- If you have first-degree relatives (parent, sibling) with myeloma or MGUS, your risk is modestly elevated
- In that case, ask your doctor about periodic blood tests (serum protein electrophoresis) starting in your 40s to catch MGUS early
Summary Table — Your 20s Prevention Protocol
| Protocol | Benefit | Effort |
|---|---|---|
| Maintain healthy BMI | Reduces insulin resistance & inflammation | Medium |
| High-fiber, plant-based diet | Gut microbiome, immune health, anti-tumor | Medium |
| Exercise 5× per week | Reduces inflammation, insulin resistance | Medium |
| Avoid benzene/solvents/pesticides | Removes a direct causative risk factor | Low |
| Don't smoke | Removes benzene + immune suppression | Low |
| Limit alcohol | Reduces inflammation, cancer risk | Low |
| Sleep 7–9 hrs, manage stress | Supports immune surveillance | Low–Medium |
| Know family history | Enables early screening if needed | Low |
Bottom Line
At 20, you are in an excellent position. You almost certainly won't develop myeloma for decades, if ever. But the habits you build now — staying lean, eating anti-inflammatory foods, exercising, avoiding chemical toxins, not smoking — reduce chronic inflammation and insulin resistance, which are the two main biological pathways through which lifestyle contributes to myeloma risk later in life.
No supplement, protocol or "hack" eliminates genetic risk — but a disciplined healthy lifestyle is genuinely protective and also dramatically lowers your risk of dozens of other cancers, heart disease, and diabetes simultaneously.
If a close family member has had myeloma, mention it to your doctor. Otherwise, no special screening is needed at your age — just live well.
— Goldman-Cecil Medicine, pp. 1895–1896, 1978 | NUTRIVENTION Trial, Cancer Discovery 2026 [PMID: 41342739]
This is a shared conversation. Sign in to Orris to start your own chat.