Glomerulonephritis definition,pathophysiology,causes treatment and management
Reading File
Finding Sources
Searching PubMed
"glomerulonephritis"[MeSH Terms] AND treatment
Searching the Web
glomerulonephritis pathophysiology causes treatment management 2025
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent - I now have comprehensive content. Let me compile a thorough, well-structured answer using all the information gathered from Harrison's Principles of Internal Medicine 22E and Comprehensive Clinical Nephrology.
Glomerulonephritis (GN): Complete Clinical Overview
1. Definition
Glomerulonephritis (GN) refers to a group of immune-mediated inflammatory disorders affecting the glomeruli - the kidney's filtration units. The glomeruli become inflamed, impairing their ability to filter waste, excess fluids, and electrolytes from the blood.
GN is associated with hypertension, volume expansion, and an abnormal urinalysis. It may present acutely (over days to weeks), subacutely, or as a chronic, smoldering process with inexorable progression to chronic kidney failure over months to years. - Harrison's Principles of Internal Medicine 22E
2. Pathophysiology
The central mechanism in most forms of GN is immune injury to the glomerulus, which proceeds through three major immunological pathways:
A. Immune Complex Deposition (most common)
Antibody-antigen complexes form in the circulation or in situ at the glomerulus. These complexes:
- Deposit in the glomerular capillary walls (subendothelial, mesangial, or subepithelial locations)
- Activate the complement cascade (particularly C3)
- Trigger an intense inflammatory response with cellular proliferation
- Reduce filtering surface area, causing oliguria and salt/water retention
- Cause "bloodless capillaries" - disruption of capillary blood flow by proliferating cells
Classic example: Post-infectious GN (PIGN) - antibody-bacterial antigen complexes deposit after streptococcal pharyngitis or impetigo 10 days to 3 weeks after infection, consuming C3 (causing hypocomplementemia). - Harrison's 22E
B. Anti-GBM Antibody Disease
Circulating IgG autoantibodies are directed at an epitope in the α3 chain of the non-collagenous domain of Type IV collagen in the glomerular basement membrane (GBM). This is the mechanism in Goodpasture disease. Plasmapheresis is required to remove all GBM autoantibody, which may take weeks to months.
C. ANCA-Associated Vasculitis (Pauci-Immune)
Antineutrophilic cytoplasmic antibodies (ANCA) - either anti-proteinase 3 (PR3, causing granulomatous disease) or anti-myeloperoxidase (MPO, causing microscopic polyangiitis) - activate neutrophils, causing necrotizing glomerular inflammation with minimal immune deposits.
The RPGN Classification
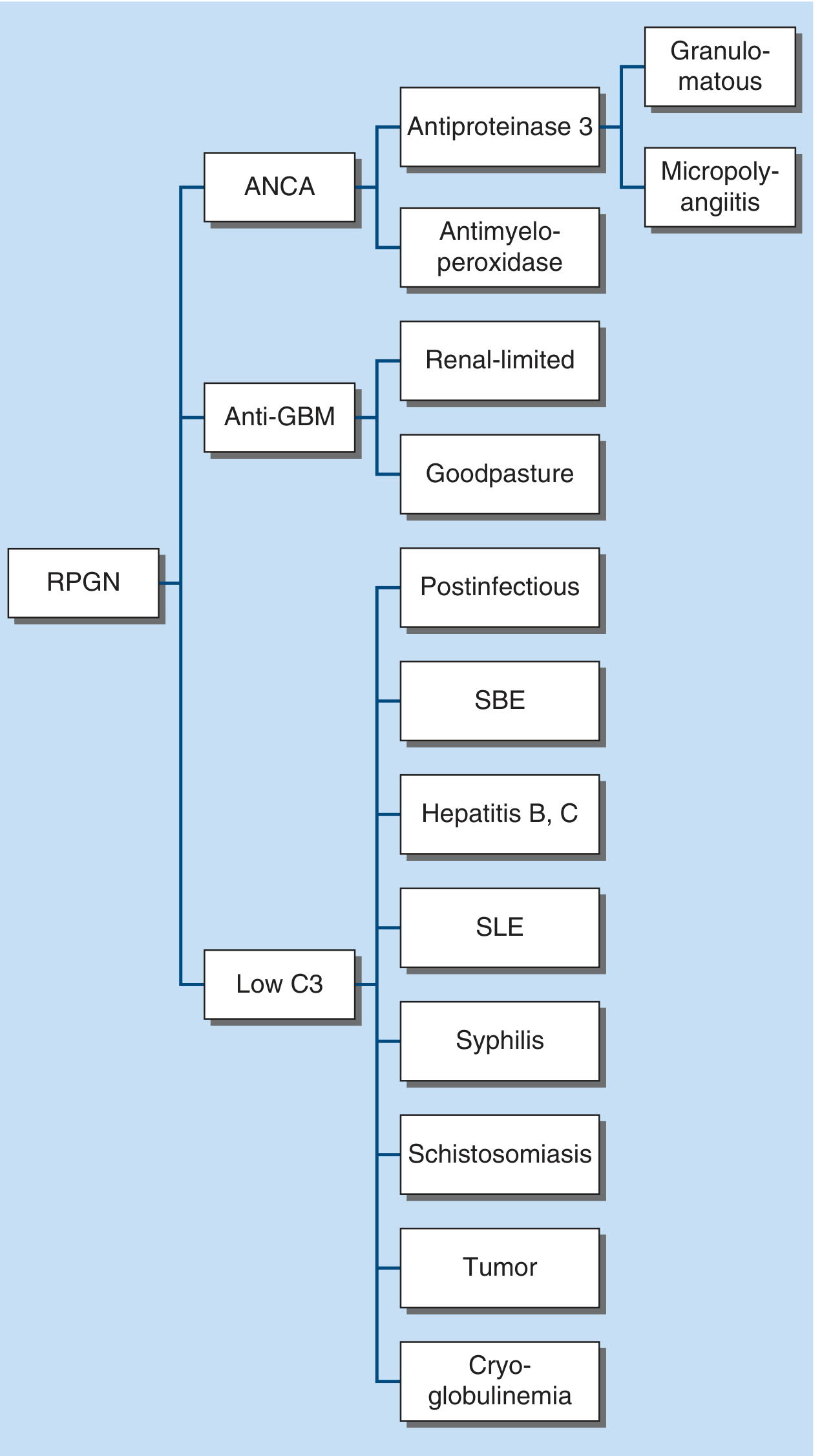
Rapidly Progressive Glomerulonephritis (RPGN) is classified by immunofluorescence into three main categories:
- Type I - Anti-GBM antibody (Goodpasture syndrome, renal-limited)
- Type II - Immune complex (Low C3: postinfectious, SBE, hepatitis B/C, SLE, cryoglobulinemia, syphilis, schistosomiasis, tumors)
- Type III - ANCA-positive pauci-immune vasculitis (granulomatosis with polyangiitis, microscopic polyangiitis)
3. Causes / Etiology
Primary (Idiopathic / Renal-Limited)
| Type | Key Features |
|---|---|
| IgA Nephropathy | Most common GN worldwide; mesangial deposition of galactose-deficient IgA-1; gross hematuria within 1-3 days of viral pharyngitis |
| Membranoproliferative GN (MPGN) | "Tram-track" GBM splitting; can be immune complex or C3 glomerulopathy |
| Focal Segmental Glomerulosclerosis | Podocyte injury; nephrotic syndrome + hematuria |
| Minimal Change Disease | Pure nephrotic syndrome; mainly in children |
Secondary (Systemic Disease)
| Category | Examples |
|---|---|
| Infections | Group A streptococci (PSGN), staphylococci (MRSA), subacute bacterial endocarditis, hepatitis B/C, HIV, syphilis, schistosomiasis, malaria |
| Autoimmune | Lupus nephritis (SLE) - >50% of SLE patients develop kidney disease; ANCA vasculitis (GPA, MPA, EGPA) |
| Anti-GBM | Goodpasture disease |
| Cryoglobulinemia | Hepatitis C; low C3 and C4; high rheumatoid factor |
| IgA Vasculitis | Henoch-Schönlein purpura; palpable purpura, arthralgia, GI bleeding |
| Malignancy | Lymphoma, myeloma, lung/renal cell carcinoma |
| Drugs | NSAIDs, gold, penicillamine, lithium, captopril |
4. Clinical Presentation
Nephritic Syndrome (typical GN presentation)
- Hematuria - microscopic (dysmorphic RBCs) or macroscopic ("cola-colored" / "tea-colored" urine due to hematin formation in acid urine)
- Proteinuria (usually sub-nephrotic, <3.5 g/day)
- Oliguria / anuria - from reduced filtering surface area and prerenal Na+/water retention
- Hypertension - from volume expansion
- Edema - from salt and water retention; ascites in children; pulmonary edema in elderly
- Urinary sediment - RBC casts, dysmorphic RBCs, WBC casts (pathognomonic of GN)
Rapidly Progressive GN (RPGN) - Medical Emergency
- Days to weeks of declining renal function
- Crescents on biopsy (proliferating parietal epithelial cells + monocytes filling Bowman's space)
- Can lead to dialysis-dependent renal failure within weeks if untreated
Chronic GN
- Slow, irreversible progression to CKD and ESRD over years
- Third leading cause of CKD; accounts for ~10% of dialysis patients
5. Investigations
| Test | Purpose |
|---|---|
| Urinalysis + microscopy | Hematuria, proteinuria, RBC casts, dysmorphic RBCs |
| Serum creatinine / eGFR | Assess renal function |
| C3, C4 complement | Low in immune complex GN (PSGN, SLE, SBE, cryoglobulinemia) |
| ANCA (PR3, MPO) | ANCA vasculitis |
| Anti-GBM antibody | Goodpasture disease |
| ANA, anti-dsDNA | Lupus nephritis |
| ASOT, anti-DNase B, streptozyme | Post-streptococcal GN |
| Hepatitis B/C serology | Secondary causes |
| Cryoglobulins, rheumatoid factor | Cryoglobulinemia |
| Kidney biopsy | Gold standard for diagnosis, classification, and guiding treatment |
6. Treatment and Management
Treatment is directed at the underlying cause and severity of disease. Early diagnosis and prompt treatment are critical before chronic sclerotic changes develop.
A. General / Supportive Management (all forms)
- Blood pressure control: ACE inhibitors (ACEi) or ARBs are first-line; they reduce intraglomerular pressure and proteinuria via anti-angiotensin II inhibition
- Dietary sodium restriction and diuretics for edema and hypertension
- Fluid management: Monitor fluid balance carefully given oliguria
- Treatment of underlying infection: Antibiotics for PSGN (if infection still present); drainage for abscesses
- Lipid management and cardioprotection in nephrotic-range proteinuria
B. Post-Infectious GN (PSGN)
- Mostly self-limiting - supportive care is the mainstay
- Penicillin/amoxicillin if active streptococcal infection persists
- Antihypertensives, diuretics for volume overload
- Full complement recovery expected within 6-8 weeks; prognosis is generally excellent in children
C. IgA Nephropathy
- ACEi/ARBs for proteinuria and hypertension
- Corticosteroids if proteinuria >1 g/day despite RAAS blockade
- Fish oil (omega-3): modest benefit in some patients
- Tonsillectomy historically used (limited evidence)
- Novel targeted therapies: complement pathway inhibitors (sparsentan, iptacopan) based on recent trials
D. ANCA-Associated Vasculitis (GPA, MPA)
Induction therapy:
- Rituximab (anti-CD20) + high-dose glucocorticoids (preferred, especially for severe/relapsing disease)
- OR Cyclophosphamide (IV pulse preferred over oral) + glucocorticoids
Maintenance therapy:
- Rituximab every 6 months for 18-24 months, OR
- Azathioprine or mycophenolate mofetil
- Gradual glucocorticoid taper
For RPGN/dialysis-dependent: Plasma exchange (PLEX) may be considered (benefit debated by recent PEXIVAS trial)
E. Anti-GBM Disease (Goodpasture)
- Plasmapheresis (daily for 14 days or until anti-GBM undetectable) - removes circulating antibody
- High-dose IV methylprednisolone → oral prednisone taper
- Cyclophosphamide (oral or IV) to suppress antibody production
- Dialysis if severe renal failure; kidney recovery unlikely if oligoanuric at presentation
F. Lupus Nephritis (Class III/IV)
Induction:
- Mycophenolate mofetil (MMF) 2-3 g/day + glucocorticoids (preferred in most patients)
- OR IV cyclophosphamide + glucocorticoids
- Belimumab (add-on to MMF) has shown improved renal outcomes in recent trials
- Voclosporin (calcineurin inhibitor) + MMF is another approved induction regimen
Maintenance:
- MMF 1-2 g/day + low-dose glucocorticoids (preferred over azathioprine in high-risk groups)
- Hydroxychloroquine in all SLE patients
G. Crescentic / RPGN (any etiology)
- IV methylprednisolone pulse (500-1000 mg/day x 3 days) → oral prednisone
- Immunosuppression (cyclophosphamide or rituximab depending on etiology)
- Plasma exchange for anti-GBM disease and severe ANCA vasculitis
- Dialysis support as needed
H. End-Stage Management
- If progression to ESRD despite treatment:
- Hemodialysis or peritoneal dialysis
- Kidney transplantation (wait for anti-GBM levels to normalize before transplant in Goodpasture; >12 months of seronegativity recommended)
7. Summary Table
| GN Type | Key Immunology | C3 | Treatment |
|---|---|---|---|
| Post-infectious | Immune complexes (subendothelial) | Low | Supportive + antibiotics |
| IgA nephropathy | Mesangial IgA-1, C3 | Normal | ACEi/ARB, steroids, novel complement inhibitors |
| Lupus nephritis | Immune complexes (multi-location) | Low | MMF/cyclophosphamide + steroids |
| ANCA vasculitis | Pauci-immune | Normal | Rituximab or cyclophosphamide + steroids |
| Anti-GBM | Linear IgG on GBM | Normal | Plasmapheresis + cyclophosphamide + steroids |
| Cryoglobulinemia | Immune complexes (HCV-related) | Low C3 and C4 | Treat HCV, rituximab, steroids |
| IgA vasculitis (HSP) | Mesangial IgA, C3 | Normal | Supportive; steroids for severe renal disease |
Recent evidence note: A 2026 systematic review (PMID: 40971335) on C3 glomerulopathy and primary immune complex MPGN highlights that proteinuria correlates with poor clinical outcomes, reinforcing aggressive proteinuria management. A 2024 network meta-analysis (PMID: 39212247) found that multitarget therapy (MMF + tacrolimus) and biologics (belimumab, voclosporin) outperform standard therapy for lupus nephritis induction.
Sources: Harrison's Principles of Internal Medicine 22E, Comprehensive Clinical Nephrology 7th Edition, Brenner and Rector's The Kidney, Frameworks for Internal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.