Pt difficulty in speaking of 66male pt
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent content retrieved. Now I have comprehensive information to provide a detailed clinical answer.
Difficulty Speaking in a 66-Year-Old Male — Clinical Approach
Key Distinction: Dysarthria vs. Aphasia
These are the two main categories of "difficulty speaking" and must be differentiated first.
| Feature | Aphasia | Dysarthria |
|---|---|---|
| Definition | Language disorder (comprehension/expression of words) | Motor speech disorder (articulation, phonation, prosody) |
| Mechanism | Cortical/language center damage | Neuromuscular control dysfunction |
| Speech quality | Wrong words, paraphasias, comprehension deficits | Slurred/slow/nasal speech, but correct words |
| Writing | Also affected | Usually preserved |
Aphasia
Most common cause in a 66-year-old male: Stroke
- In a UK community study, new stroke-induced aphasia cases numbered ~202/year per 250,000 population
- 38% of acute stroke patients are aphasic on admission
- Nearly half of severe aphasia cases die soon after stroke onset
- Best predictor of recovery: less severe aphasia close to stroke onset
- ~95% with mild aphasia reach best recovery at 2 weeks; severe aphasia peaks at 10 weeks
Types of Aphasia (by location):
| Type | Fluency | Comprehension | Repetition | Location |
|---|---|---|---|---|
| Broca's | Non-fluent | Intact | Impaired | Left inferior frontal |
| Wernicke's | Fluent | Impaired | Impaired | Left superior temporal |
| Global | Non-fluent | Impaired | Impaired | Large left MCA territory |
| Conduction | Fluent | Intact | Impaired | Arcuate fasciculus |
| Anomic | Fluent | Intact | Intact | Variable |
Dysarthria
Dysarthria = impaired speech from abnormal neuromuscular control, affecting articulation, respiration, prosody, resonance, and phonation.
Assessment includes 3 activities (Localization in Clinical Neurology):
- Contextual speech (reading a standard paragraph + spontaneous speech)
- Vowel prolongation ("ahhh...") — reveals laryngeal tremor, spasticity
- Diadochokinesis — rapid "puh-tuh-kuh" repetitions (tests lips, tongue, posterior tongue)
Types of Dysarthria and Localization:
| Type | Quality | Lesion Level |
|---|---|---|
| Flaccid | Breathy, hypernasal, short phrases | Lower motor neuron / multiple cranial nerve palsies |
| Spastic | Harsh, strained, strangled; slow rate; hypernasality | Bilateral upper motor neuron |
| Ataxic | Irregular breakdowns, vowel distortions, excess/equal stress | Cerebellum |
| Hypokinetic | Soft, monotone, rapid bursts (festinating speech) | Parkinsonism (basal ganglia) |
| Mixed | Combined features | ALS (flaccid+spastic), MS (spastic+ataxic), Wilson disease |
Differential Diagnosis in a 66-Year-Old Male
Neurological (Most common):
- Ischemic stroke (MCA territory) — most urgent; sudden onset
- TIA — transient episode, resolves < 24h
- Hemorrhagic stroke
- Brain tumor — progressive, may have headache, seizures
- Parkinson's disease — hypokinetic dysarthria + other features
- ALS — mixed flaccid-spastic dysarthria, progressive
Other causes to consider:
- Myasthenia gravis — fluctuating, worsens with fatigue
- Hypothyroidism — slow, hoarse speech
- Drug toxicity (e.g., phenytoin → ataxic dysarthria; sedatives)
- Hypoglycemia — reversible with glucose
- Oral/laryngeal pathology — consider if no neurological signs
Urgent Red Flags — STROKE Protocol
In a 66-year-old male, sudden-onset difficulty speaking = stroke until proven otherwise.
FAST criteria: Face drooping | Arm weakness | Speech difficulty | Time to call emergency
Immediate workup:
- Non-contrast CT head (rule out hemorrhage)
- Blood glucose (rule out hypoglycemia)
- ECG (AF → cardioembolic stroke)
- CBC, coagulation, metabolic panel
- MRI + DWI if CT negative but high suspicion
Time-sensitive intervention:
- IV tPA within 4.5 hours of onset (if ischemic, no contraindications)
- Mechanical thrombectomy within 24 hours (large vessel occlusion)
Management
Aphasia/Dysarthric rehabilitation:
- Speech therapy is the cornerstone — retrains contralateral areas to compensate
- Dysarthric patients learn to slow delivery and emphasize words to improve clarity
- For aphasia: stimulation-facilitation techniques (picture matching, sentence completion, phoneme-based training)
- Melodic intonation therapy (MIT) — particularly effective in non-fluent (Broca's) aphasia
- Constraint-induced language therapy with intensive phonemic cues
Sources: Bradley and Daroff's Neurology in Clinical Practice | Localization in Clinical Neurology, 8e
Face tilted o. One side
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Excellent. Here is a comprehensive clinical answer integrating the new symptom:
Updated Clinical Picture: 66M — Difficulty Speaking + Face Tilted/Drooping to One Side
This combination strongly points to unilateral facial palsy (CN VII), which in this context must be urgently classified as central (UMN) vs. peripheral (LMN) — the most critical clinical distinction.
The Critical Distinction: UMN vs. LMN Facial Palsy
| Feature | Central (UMN) — STROKE | Peripheral (LMN) — Bell's Palsy |
|---|---|---|
| Forehead sparing? | Yes — forehead spared (bilateral cortical input) | No — entire face including forehead affected |
| Eye closure | Preserved | Lost — eye won't close (Bell's phenomenon) |
| Which face affected? | Contralateral lower face | Ipsilateral whole face |
| Cause in 66M | Stroke (MCA territory), tumor | Bell's palsy (HSV-1), Ramsay Hunt, parotid tumor |
| Urgency | EMERGENCY | Urgent but less acute |
Key rule: If the upper face (forehead wrinkling, eye closure) is spared → stroke until proven otherwise. If the upper face is involved → likely Bell's palsy or peripheral CN VII lesion.
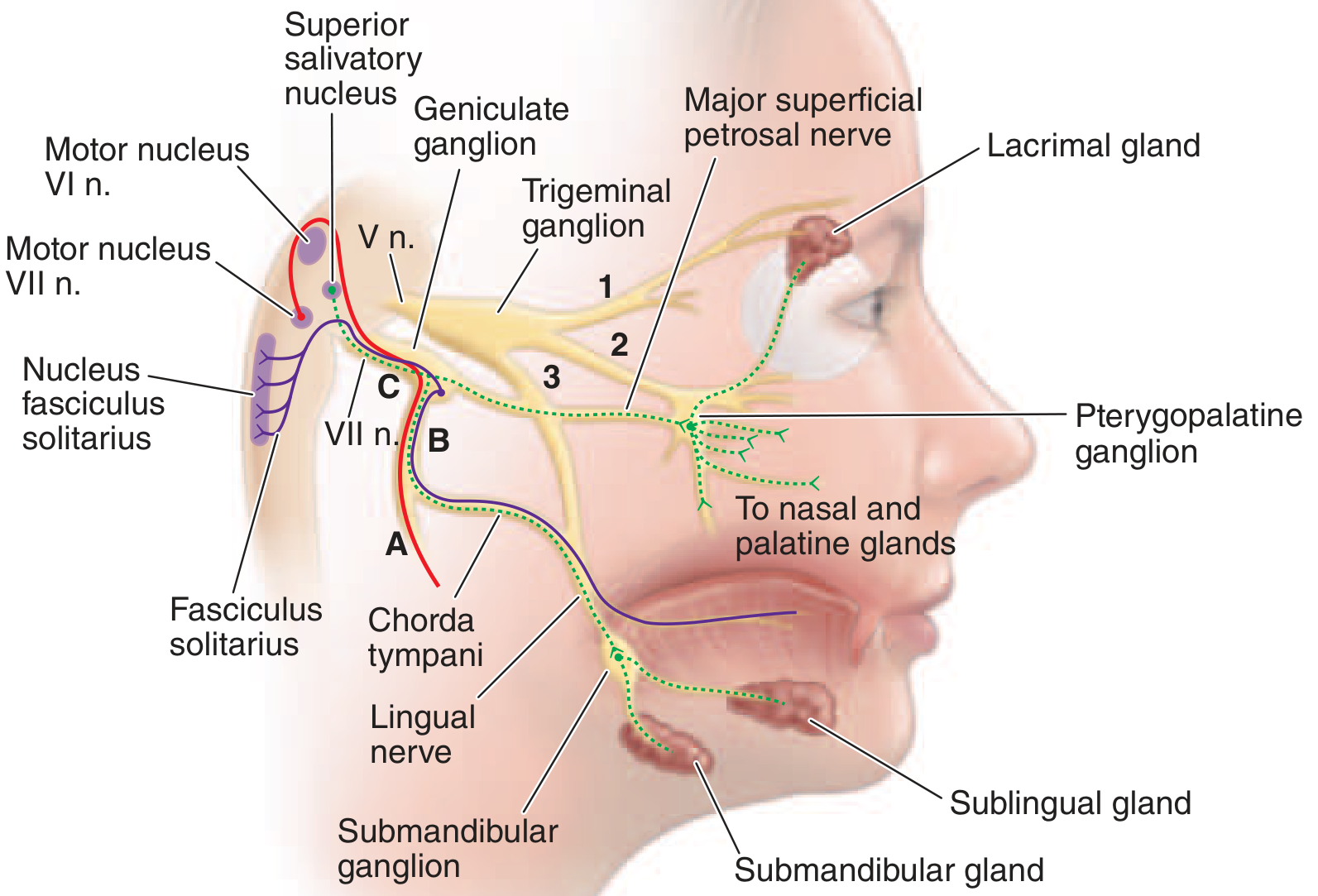
Anatomy of CN VII — Lesion Localization
The facial nerve (CN VII) supplies all muscles of facial expression, stapedius, stylohyoid, and posterior digastric. Its parasympathetic fibers control lacrimation and salivation; sensory fibers carry taste from anterior 2/3 of the tongue.
Lesion site determines what additional features are present:
| Site | Motor Loss | Additional Features |
|---|---|---|
| Above nucleus (cortex/subcortex) | Contralateral lower face only | + Arm/leg weakness (stroke) |
| Pons (nucleus) | Ipsilateral whole face | + Ipsilateral CN VI palsy (abducens) + contralateral limb weakness |
| Geniculate ganglion | Ipsilateral whole face | + Loss of taste (ant. 2/3 tongue) + reduced lacrimation + hyperacusis |
| Stylomastoid foramen | Ipsilateral whole face | Motor only; taste and lacrimation intact |
| Parotid | Partial (individual branches) | Parotid mass/swelling |
Clinical Features of Complete Peripheral Facial Palsy
(Harrison's, 22nd Ed.)
- Corner of the mouth droops
- Creases and skin folds effaced
- Forehead unfurrowed
- Eyelids will not close → eye rolls upward on attempted closure (Bell's phenomenon)
- Lower lid sags → tears spill over cheek
- Food collects between teeth and lips
- Saliva dribbles from corner of mouth
- Patient feels heaviness/numbness in face
Bell's Palsy (Most Common Peripheral Cause)
- Incidence: ~25/100,000/year (~1 in 60 over a lifetime)
- Onset: abrupt — maximal weakness within 48 hours
- May be preceded by pain behind the ear for 1–2 days
- Cause: HSV-1 reactivation in geniculate ganglion (most common); VZV in up to 1/3
- 80% recover within weeks to months
- Incomplete paralysis in first week = most favorable prognostic sign
- MRI: swelling and enhancement of geniculate ganglion and facial nerve in temporal bone
Ramsay Hunt syndrome (VZV): Severe facial palsy + vesicles in external auditory canal ± CN VIII involvement (deafness, tinnitus, vertigo)
In This 66-Year-Old Male — Priority Assessment
Given difficulty speaking + unilateral facial drooping together:
Step 1: Is this a STROKE?
- Sudden onset + facial droop + dysarthria/aphasia = activate stroke protocol immediately
- Check FAST: Face drooping ✓ | Speech difficulty ✓
- Also assess: arm/leg weakness, gait, vision
Step 2: Emergency workup
| Test | Purpose |
|---|---|
| Non-contrast CT head | Rule out hemorrhagic stroke |
| Blood glucose | Rule out hypoglycemia |
| ECG | Detect atrial fibrillation |
| CBC, metabolic panel, coagulation | Baseline + tPA eligibility |
| MRI + DWI | Gold standard for ischemic stroke (if CT negative) |
Step 3: Examine forehead
- Forehead spared → Likely stroke → IV tPA within 4.5 hours if eligible
- Forehead involved (whole face) → Likely Bell's palsy or peripheral lesion → steroids ± antivirals
Treatment of Bell's Palsy (if confirmed)
- Prednisolone 25 mg twice daily × 10 days (started within 72 hours of onset)
- Acyclovir/Valacyclovir if Ramsay Hunt suspected (vesicles present)
- Eye protection: lubricating drops, eye patch at night (prevent corneal exposure)
Bottom line: In a 66-year-old male, facial drooping + speech difficulty = stroke must be ruled out first. The presence or absence of forehead involvement is the fastest bedside clue to localize the lesion.
Sources: Harrison's Principles of Internal Medicine 22E | Gray's Anatomy for Students | Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.