Topographic anatomy of respiratory system- thoracic cavity , lungs , pleura and bronchi
Reading File
Finding Sources
Finding Sources
Searching Images
topographic anatomy thoracic cavity lungs pleura bronchi
Finding Sources
Finding Sources
Finding Sources
Searching Images
lung lobes fissures surface anatomy diagram
Loading Image
Loading Image
Searching Images
pleural cavity parietal visceral pleura costodiaphragmatic recess diagram
Loading Image
Searching Images
bronchial tree trachea main bronchi lobar segmental anatomy diagram
Loading Image
Searching Images
mediastinum trachea carina hilum lung root anatomy
Now I have comprehensive material to compose a detailed answer. Let me synthesize everything.
Topographic Anatomy of the Respiratory System: Thoracic Cavity, Lungs, Pleura, and Bronchi
1. THE THORACIC CAVITY
Boundaries
- Superior aperture (thoracic inlet): Bounded by the manubrium sterni anteriorly, the 1st rib laterally, and T1 vertebra posteriorly. Transmits the trachea, oesophagus, great vessels, and apex of the lung (the pleural dome projects 2–3 cm above the medial third of the clavicle into the neck).
- Inferior aperture (thoracic outlet): Closed by the diaphragm; bounded by the xiphisternum, costal cartilages (7–10), ribs 11–12, and T12 vertebra.
- Walls: Sternum + costal cartilages (anterior), ribs + intercostal muscles (lateral), thoracic vertebral column (posterior).
Compartments
| Compartment | Contents |
|---|---|
| Right pleural cavity | Right lung + pleura |
| Left pleural cavity | Left lung + pleura |
| Mediastinum | Heart, great vessels, trachea, oesophagus, thoracic duct, phrenic & vagus nerves |
The mediastinum is further divided into superior (above the sternal angle / T4–T5 disc) and inferior (anterior, middle, posterior).
Key Topographic Landmarks
- Sternal angle (angle of Louis): At the level of T4/T5, marks the junction of the manubrium and body of sternum. Corresponds to the bifurcation of the trachea (carina), the level of the aortic arch, and the upper border of the pericardium.
- Xiphosternal junction: Corresponds to T9 and the level of the central tendon of the diaphragm.
2. THE LUNGS
General Features
The lungs occupy the pleural cavities on either side of the mediastinum. They are conical in shape with:
- Apex — projects 2–3 cm above the clavicle into the root of the neck, covered by the cervical pleura (pleural dome) and the suprapleural membrane (Sibson's fascia)
- Base (diaphragmatic surface) — concave, rests on the diaphragm; right side higher than left (due to liver)
- Costal surface — convex, related to the ribs
- Medial (mediastinal) surface — contains the hilum
Surfaces and Relations
| Surface | Relations |
|---|---|
| Apex | Subclavian artery grooves the right, brachiocephalic (left) the left; cervical sympathetic chain, brachial plexus |
| Costal | Ribs, intercostal spaces |
| Base | Right = liver; Left = stomach, spleen |
| Mediastinal | Heart/pericardium (cardiac impression), great vessels, oesophagus |
Hilum
The root of the lung lies at T5–T7 and contains:
- Main bronchus
- Pulmonary artery
- Two pulmonary veins (superior and inferior)
- Bronchial arteries and veins
- Lymphatics and autonomic nerves
On the right, the arrangement from anterior to posterior is: vein, artery, bronchus. Superior to inferior: upper lobe bronchus (eparterial) → pulmonary artery → lower lobe bronchi.
On the left, the pulmonary artery arches over the main bronchus (hyparterial arrangement).
Lobes and Fissures
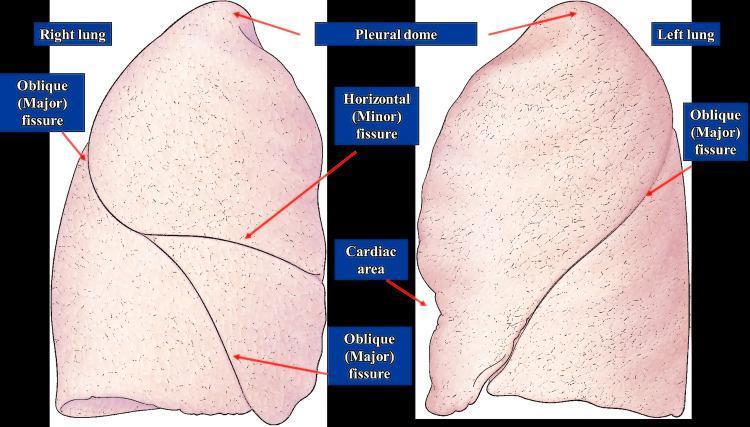
| Lung | Fissures | Lobes |
|---|---|---|
| Right | Oblique (major) + Horizontal (minor/transverse) | Upper, Middle, Lower (3 lobes) |
| Left | Oblique (major) only | Upper (+ Lingula), Lower (2 lobes) |
Oblique fissure (both sides): runs from T3/T4 spinous process posteriorly, around the chest to the 6th rib/costal cartilage anteriorly — approximated by the medial border of the scapula when the arm is fully abducted.
Horizontal fissure (right only): runs from the oblique fissure at the midaxillary line to the sternum at the level of the 4th costal cartilage.
Surface Projections of Lung Borders
| Border | Projection |
|---|---|
| Anterior | Both lungs meet behind manubrium at 2nd costal cartilage; right descends to 6th costal cartilage; left diverges at 4th CC, leaving the cardiac notch |
| Inferior | Crosses rib 6 at midclavicular line, rib 8 at midaxillary line, rib 10 at scapular line, T10/T11 posteriorly |
| Apex | 2–3 cm above clavicle medially |
Bronchopulmonary Segments
Each lobe is subdivided into bronchopulmonary segments — 10 on the right, 8–10 on the left. Each segment is:
- A functionally independent unit
- Supplied by a segmental (tertiary) bronchus and a segmental pulmonary artery
- Drained by intersegmental pulmonary veins
- Surgically resectable individually
Right lung segments (10):
- Upper lobe: apical, posterior, anterior
- Middle lobe: lateral, medial
- Lower lobe: superior (apical), medial basal, anterior basal, lateral basal, posterior basal
Left lung segments (8–10):
- Upper lobe: apical-posterior, anterior, superior lingular, inferior lingular
- Lower lobe: superior (apical), anteromedial basal, lateral basal, posterior basal
3. THE PLEURA
Layers
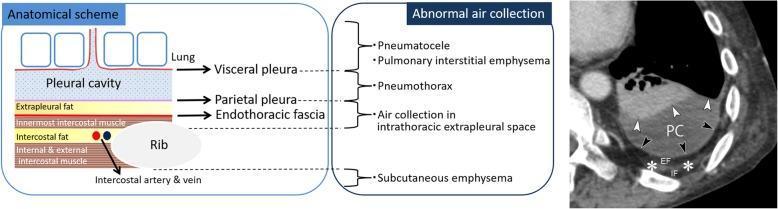
The pleura is a serous membrane with two continuous layers:
| Layer | Description |
|---|---|
| Visceral pleura | Closely adherent to lung surface; extends into fissures; innervated by visceral autonomic fibres (insensitive to pain) |
| Parietal pleura | Lines thoracic wall, diaphragm, mediastinum; innervated by somatic nerves (phrenic + intercostal — pain sensitive) |
Between the layers is the pleural cavity — a potential space containing a thin film (5–10 mL) of serous fluid for lubrication. Negative intrapleural pressure (−5 cmH₂O at rest) keeps the lung expanded.
Parts of Parietal Pleura
- Costal pleura — lines inner surface of ribs and intercostal spaces (supplied by intercostal nerves)
- Diaphragmatic pleura — covers the upper diaphragm (central part: phrenic nerve; peripheral: lower intercostal nerves)
- Mediastinal pleura — forms the lateral boundary of the mediastinum
- Cervical pleura (dome/cupula) — projects above the 1st rib into the neck; reinforced by Sibson's (suprapleural) fascia
Pleural Recesses
Sites where two layers of parietal pleura are in contact (lungs do not fill these spaces even at full inspiration):
| Recess | Location | Clinical Significance |
|---|---|---|
| Costodiaphragmatic recess | Between costal and diaphragmatic pleura; deepest at midaxillary line (2 rib spaces) | Largest recess; site of pleural effusion collection; needle aspiration via 9th intercostal space, midaxillary line |
| Costomediastinal recess | Between costal and mediastinal pleura anteriorly; most prominent on left (cardiac notch) | Smaller; relevant in cardiac surgery and thoracic approaches |
Surface Projection of Pleura vs. Lung
The pleura extends ~2 rib spaces beyond the inferior lung border:
| Level | Lung | Pleura |
|---|---|---|
| Midclavicular line | Rib 6 | Rib 8 |
| Midaxillary line | Rib 8 | Rib 10 |
| Posterior (scapular line) | Rib 10 | Rib 12 |
This gap = the costodiaphragmatic recess (pleural but not pulmonary).
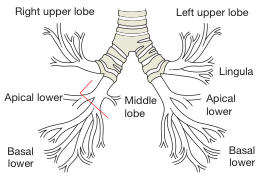
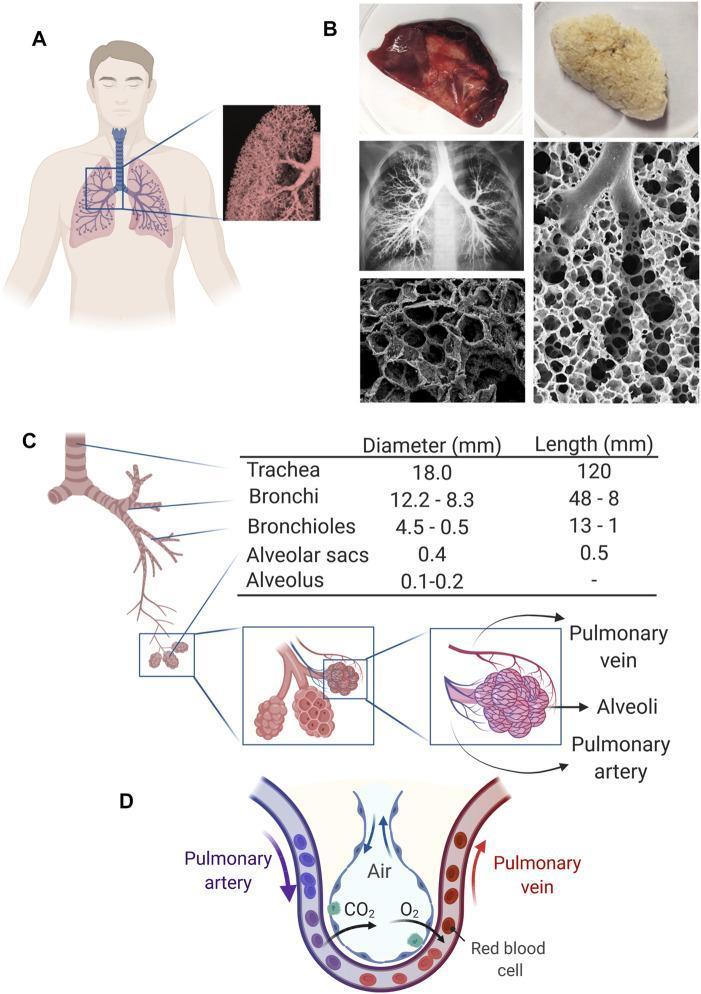
4. THE BRONCHI
Trachea
- Begins at C6 (lower border of cricoid cartilage)
- Bifurcates at the carina, T4/T5 (sternal angle level)
- Length: ~10–12 cm; diameter ~2 cm
- Composed of 16–20 C-shaped hyaline cartilage rings (posterior wall = trachealis muscle)
- Relations: anteriorly the thyroid gland; posteriorly the oesophagus; laterally the common carotid arteries
Main Bronchi
| Feature | Right Main Bronchus | Left Main Bronchus |
|---|---|---|
| Length | ~2.5 cm | ~5 cm |
| Direction | More vertical (25° from vertical) | More horizontal (45° from vertical) |
| Width | Wider | Narrower |
| Clinical significance | Foreign bodies more likely to lodge here | Less so |
The right main bronchus divides into:
- Right upper lobe bronchus (eparterial — arises above the pulmonary artery)
- Right intermediate bronchus → right middle lobe bronchus + right lower lobe bronchus
The left main bronchus is hyparterial (runs below the left pulmonary artery) and divides into:
- Left upper lobe bronchus
- Left lower lobe bronchus
Lobar → Segmental → Subsegmental Bronchi
- Lobar (secondary) bronchi: 3 on the right, 2 on the left
- Segmental (tertiary) bronchi: correspond to the bronchopulmonary segments
- Further subdivision: subsegmental → terminal bronchioles → respiratory bronchioles → alveolar ducts → alveolar sacs
Histological Layers of Bronchial Wall
From lumen outwards:
- Mucosa: pseudostratified columnar ciliated epithelium with goblet cells
- Lamina propria: loose CT with mast cells
- Smooth muscle (increasingly prominent toward bronchioles)
- Submucosal glands (seromucous — present in bronchi, absent in bronchioles)
- Cartilage plates (irregular in bronchi; absent in bronchioles <1 mm)
- Adventitia
Clinical Notes on Bronchial Anatomy
- Right middle lobe syndrome: The right middle lobe bronchus is long, narrow, and surrounded by lymph nodes — vulnerable to extrinsic compression causing recurrent collapse.
- Aspiration: With patient supine, aspirated material tends to go to the posterior segment of the right upper lobe or the superior segment of the right lower lobe. With patient erect, into the lower lobes (more so the right, due to the more vertical right main bronchus).
- Bronchoscopy landmarks: The carina is the key landmark; widening or splaying of the carina (>70°) suggests subcarinal lymphadenopathy or a left atrial mass.
Summary Table: Key Topographic Levels
| Structure | Vertebral Level | Surface Landmark |
|---|---|---|
| Apex of lung | C7/T1 | 2–3 cm above medial clavicle |
| Tracheal bifurcation (carina) | T4/T5 | Sternal angle |
| Hilum of lung | T5–T7 | 2nd–4th intercostal space |
| Inferior lung border (MCL) | — | Rib 6 |
| Inferior pleural reflection (MCL) | — | Rib 8 |
| Inferior pleural reflection (MAL) | — | Rib 10 |
| Inferior pleural reflection (posterior) | T12 | Rib 12 |
| Costodiaphragmatic recess | — | 9th–10th ICS, midaxillary |
Functions and arteries nerves veins for above parts
Searching Images
pulmonary artery vein bronchial artery lung blood supply diagram
Searching Images
intercostal nerve innervation pleura phrenic nerve diaphragm
Searching Images
pulmonary circulation gas exchange alveolar capillary oxygen carbon dioxide diagram
Searching Images
vagus nerve pulmonary plexus sympathetic bronchial innervation
Loading Image
Loading Image
Now I have all the material needed. Here is the comprehensive answer:
Functions, Arteries, Veins, and Nerves of the Respiratory System
1. THORACIC CAVITY
Functions
- Protective container for the heart, great vessels, lungs, oesophagus, and thoracic duct
- Mechanical bellows — volume changes during inspiration/expiration drive ventilation
- Pressure regulation — negative intrapleural pressure (~−5 cmH₂O at rest, −8 to −9 cmH₂O during inspiration) maintains lung expansion and facilitates venous return to the heart
- Thermal and humidification corridor for inspired air via the upper airways
Arteries of the Thoracic Wall
| Artery | Origin | Distribution |
|---|---|---|
| Posterior intercostal arteries (3–11) | Descending thoracic aorta | Intercostal spaces (run in the costal groove: nerve above, vein above, artery in middle — "VAN" from above) |
| 1st & 2nd posterior intercostal | Superior intercostal a. (from costocervical trunk of subclavian) | Upper two intercostal spaces |
| Anterior intercostal arteries | Internal thoracic artery (upper 6 spaces) + musculophrenic artery (lower 3) | Anterior intercostal spaces |
| Internal thoracic (mammary) artery | Subclavian artery | Descends 1 cm lateral to sternum; divides at 6th CC into superior epigastric + musculophrenic |
| Pericardiophrenic artery | Internal thoracic artery | Accompanies phrenic nerve to diaphragm |
Veins
- Posterior intercostal veins drain into the azygos system (right) and hemiazygos/accessory hemiazygos (left), then into the superior vena cava
- Anterior intercostal veins drain into the internal thoracic veins → brachiocephalic vein
- Azygos vein: right side; arches over root of right lung at T4, drains into SVC
- Hemiazygos and accessory hemiazygos: left side; cross midline to join azygos at T8 and T6 respectively
Nerves
- Intercostal nerves (T1–T11) — ventral rami of thoracic spinal nerves; supply intercostal muscles, parietal pleura, skin
- Subcostal nerve (T12) — below the 12th rib
- Phrenic nerve (C3, C4, C5) — motor to diaphragm + sensory to central diaphragmatic and mediastinal pleura; "C3, 4, 5 keeps the diaphragm alive"
- Sympathetic chain — paravertebral ganglia T1–T12; splanchnic nerves arise from T5–T12
2. THE LUNGS
Functions
The lung has two blood supplies serving distinct functions:
| System | Function |
|---|---|
| Pulmonary circulation | Gas exchange (functional circulation) |
| Bronchial circulation | Nutritive supply to bronchial walls, pleura, and lung parenchyma (systemic) |
Primary Functions:
- Gas exchange — O₂ diffuses from alveoli into pulmonary capillary blood; CO₂ diffuses in reverse across the ultra-thin air-blood barrier (~0.5 µm)
- Acid-base regulation — CO₂ elimination controls plasma pH
- Metabolic functions — angiotensin I → angiotensin II (ACE in pulmonary endothelium); inactivation of bradykinin, serotonin, prostaglandins
- Filtration — removes small emboli and microaggregates from venous blood
- Phonation — expired air drives vocal cord vibration
Arteries of the Lung
A. Pulmonary Arteries (Functional — deoxygenated blood)
| Vessel | Origin/Course | Note |
|---|---|---|
| Pulmonary trunk | Right ventricle → bifurcates at T4/T5 (under aortic arch) | Carries deoxygenated blood |
| Right pulmonary artery | Longer; passes behind ascending aorta and SVC → enters right hilum | Anterior to right main bronchus at hilum |
| Left pulmonary artery | Shorter; arches over left main bronchus → left hilum | Connected to aortic arch by ligamentum arteriosum (remnant of ductus arteriosus) |
| Lobar → segmental arteries | Accompany bronchi within lung parenchyma | One artery per bronchopulmonary segment |
B. Bronchial Arteries (Nutritive — oxygenated blood)
| Side | Origin | Number |
|---|---|---|
| Right | 1st right posterior intercostal artery (or from right side of aorta) | Usually 1 |
| Left | Directly from descending thoracic aorta (T5–T6 level) | Usually 2 |
Bronchial arteries supply: bronchial walls down to terminal bronchioles, pulmonary connective tissue, visceral pleura, hilar lymph nodes, and vasa vasorum of pulmonary vessels.
Clinical note: In chronic lung disease (bronchiectasis, cystic fibrosis), bronchial arteries hypertrophy massively and are the source of life-threatening haemoptysis — treated by bronchial artery embolization.
Veins of the Lung
A. Pulmonary Veins (return oxygenated blood to left atrium)
- Four pulmonary veins (2 superior, 2 inferior) emerge from the hilum
- Enter the left atrium at the four corners of its posterior wall
- The superior pulmonary veins drain the upper and middle lobes; inferior veins drain the lower lobes
- Run anteroinferior to the bronchi and pulmonary arteries — important surgical anatomy
- Pulmonary veins carry the only oxygenated blood in veins in the body
B. Bronchial Veins
- Drain the larger bronchi and hilar structures only
- Right bronchial vein → azygos vein
- Left bronchial vein → accessory hemiazygos or left superior intercostal vein
- (Most bronchial capillary blood drains into pulmonary veins — a small component of normal right-to-left physiological shunt)
Nerves of the Lung
A. Pulmonary Plexus
Formed anterior and posterior to the lung root by:
- Vagus nerve (CN X) — parasympathetic fibres
- Sympathetic fibres — from T2–T5 thoracic ganglia via the cardiac/pulmonary branches
| Division | Effect on Bronchi | Effect on Vessels | Effect on Glands |
|---|---|---|---|
| Parasympathetic (vagus) | Bronchoconstriction | Vasodilation | Increased secretion |
| Sympathetic (T2–T5) | Bronchodilation | Vasoconstriction | Decreased secretion |
B. Afferent (Sensory) Fibres
| Receptor | Stimulus | Pathway | Reflex |
|---|---|---|---|
| Stretch receptors (SAR) | Lung inflation | Vagus | Hering-Breuer reflex (terminates inspiration) |
| Irritant receptors (RAR) | Irritants, cold air | Vagus | Cough, bronchoconstriction |
| J receptors (juxtacapillary) | Pulmonary congestion, emboli | Vagus | Dyspnoea, rapid shallow breathing |
| Free nerve endings | Pain (visceral pleura insensitive) | Vagus | — |
Note: The lung parenchyma and visceral pleura are insensitive to pain (no somatic innervation). Pain from the lung is only generated when the parietal pleura, diaphragm, or chest wall is involved.
Lymphatics of the Lung
- Superficial (subpleural) plexus — drains the peripheral lung
- Deep (peribronchial) plexus — drains lung parenchyma alongside bronchi and vessels
- Both drain to hilar lymph nodes → tracheobronchial nodes → paratracheal nodes → thoracic duct (left) or right lymphatic duct
- Subcarinal nodes (between main bronchi) are a key station in lung cancer staging
3. THE PLEURA
Functions
- Lubrication — thin film of pleural fluid (5–10 mL) reduces friction during breathing
- Force transmission — negative intrapleural pressure couples chest wall movement to lung expansion
- Surface tension seal — keeps the visceral and parietal layers apposed, preventing lung collapse
- Compartmentalization — contains infections, haemorrhage, or air to one pleural space
Arteries of the Pleura
| Pleura | Arterial Supply |
|---|---|
| Parietal (costal) | Posterior intercostal arteries + anterior intercostal branches of internal thoracic |
| Parietal (diaphragmatic) | Musculophrenic artery + inferior phrenic artery |
| Parietal (mediastinal) | Pericardiophrenic artery + bronchial arteries |
| Visceral pleura | Bronchial arteries (drains partly into pulmonary veins) |
Veins of the Pleura
- Parietal pleura veins → intercostal veins → azygos/hemiazygos system
- Visceral pleura veins → pulmonary veins (most) + bronchial veins (smaller contribution)
Nerves of the Pleura
| Region | Nerve Supply | Sensation |
|---|---|---|
| Visceral pleura | Autonomic (visceral afferents via vagus + sympathetic) | Insensitive to pain; sensitive to stretch |
| Costal parietal pleura | Intercostal nerves (T1–T11) | Pain localised to chest wall |
| Central diaphragmatic pleura | Phrenic nerve (C3, C4, C5) | Pain referred to tip of shoulder (C4 dermatome) |
| Peripheral diaphragmatic pleura | Lower intercostal nerves (T6–T11) | Pain referred to anterior abdominal wall |
| Mediastinal pleura | Phrenic nerve | Referred to neck/shoulder |
| Cervical pleura (dome) | Cervical plexus branches | Neck pain |
Key clinical point: Pleuritic pain from the costal parietal pleura is sharp, localised, and worsened by breathing. Central diaphragmatic pleuritis (e.g., sub-phrenic abscess) causes shoulder-tip pain via the phrenic nerve (C4).
4. THE BRONCHI AND TRACHEA
Functions
| Level | Function |
|---|---|
| Trachea & main bronchi | Air conduction; warming, humidifying, and filtering inspired air; mucociliary clearance (ciliated epithelium + mucus) |
| Lobar & segmental bronchi | Continued conduction + distribution of air to specific segments |
| Terminal bronchioles | Last purely conducting airway (no gas exchange) |
| Respiratory bronchioles | Transitional zone — partial gas exchange begins |
| Alveolar ducts & sacs | Primary site of gas exchange |
Mucociliary escalator: Cilia beat ~12–15 Hz; mucus-trapped particles are propelled upward at ~1 cm/min toward the larynx for expectoration or swallowing.
Arteries of the Trachea and Bronchi
| Segment | Arterial Supply |
|---|---|
| Trachea (cervical) | Inferior thyroid artery (from thyrocervical trunk) |
| Trachea (thoracic) | Bronchial arteries + branches of subclavian |
| Main bronchi | Bronchial arteries from descending thoracic aorta |
| Intrapulmonary bronchi | Bronchial arteries (follow bronchi) + small branches from pulmonary arteries |
Bronchial arteries (summary):
- 2–3 total (1 right + 2 left typically)
- Right originates from 1st right posterior intercostal artery or directly from aorta
- Left × 2 originate directly from aorta at T5–T6
- Anastomose with pulmonary capillaries at the bronchiolar level
Veins of the Trachea and Bronchi
| Segment | Venous Drainage |
|---|---|
| Trachea (cervical) | Inferior thyroid veins → brachiocephalic veins |
| Main & lobar bronchi | Bronchial veins → azygos (right) / hemiazygos (left) |
| Intrapulmonary bronchi | Bronchial venules drain into pulmonary veins (contributes to physiological shunt) |
Nerves of the Trachea and Bronchi
| Nerve | Type | Effect |
|---|---|---|
| Recurrent laryngeal nerve (CN X branch) | Mixed | Supplies trachea; left RLN loops under aortic arch — vulnerable in aortic aneurysm, lung cancer, mediastinal mass |
| Vagus nerve (CN X) | Parasympathetic efferent | Bronchoconstriction, increased mucus secretion |
| Sympathetic T2–T5 | Sympathetic efferent | Bronchodilation, decreased secretion |
| Vagal afferents | Sensory | Cough reflex from tracheal and carinal mucosa (carina most sensitive) — touching the carina triggers violent coughing |
| Pulmonary plexus branches | Mixed autonomic | Follow bronchi into lung parenchyma |
The pulmonary plexus lies anterior (anterior pulmonary plexus) and posterior (posterior pulmonary plexus — larger) to the lung root. It receives:
- Parasympathetic: pre-ganglionic fibres from vagus → synapse in ganglia in bronchial walls
- Sympathetic: post-ganglionic fibres from T2–T5 sympathetic ganglia
Summary Reference Table
| Structure | Artery | Vein | Nerve |
|---|---|---|---|
| Thoracic wall | Posterior intercostal (aorta) + anterior intercostal (internal thoracic) | Azygos/hemiazygos system | Intercostal nerves T1–T11 |
| Diaphragm | Pericardiophrenic + musculophrenic + inferior phrenic | Inferior phrenic veins | Phrenic (C3,4,5) motor; T6–T12 peripheral sensory |
| Lungs (functional) | Pulmonary arteries (right ventricle) | Pulmonary veins (left atrium) | Pulmonary plexus (vagus + sympathetic T2–T5) |
| Lungs (nutritive) | Bronchial arteries (aorta) | Bronchial veins → azygos; partly → pulmonary veins | Same |
| Parietal pleura (costal) | Posterior intercostal arteries | Intercostal veins | Intercostal nerves (pain sensitive) |
| Parietal pleura (diaphragmatic, central) | Pericardiophrenic / inferior phrenic | Phrenic veins | Phrenic nerve → shoulder-tip referral |
| Visceral pleura | Bronchial arteries | Pulmonary veins | Autonomic only — pain insensitive |
| Trachea (thoracic) | Bronchial arteries | Azygos veins | Recurrent laryngeal + vagus |
| Bronchi | Bronchial arteries (aorta) | Bronchial veins → azygos; intrapulmonary → pulmonary veins | Pulmonary plexus (vagus + sympathetic) |
Functions and arteries nerves veins for above parts
The previous response already covered Functions, Arteries, Veins, and Nerves for all four parts — Thoracic Cavity, Lungs, Pleura, and Bronchi — in full detail.
Here's a quick recap of what was covered:
What was already answered:
| Part | Functions | Arteries | Veins | Nerves |
|---|---|---|---|---|
| Thoracic Cavity | Protective container, bellows mechanism, pressure regulation | Posterior/anterior intercostal, internal thoracic | Azygos, hemiazygos, intercostal veins | Intercostal T1–T11, phrenic C3,4,5, sympathetic chain |
| Lungs | Gas exchange, acid-base, metabolic (ACE), filtration | Pulmonary arteries (functional) + Bronchial arteries (nutritive, from aorta) | Pulmonary veins (to left atrium) + Bronchial veins (to azygos) | Pulmonary plexus — vagus (parasympathetic) + sympathetic T2–T5 |
| Pleura | Lubrication, force coupling, seal | Intercostal + pericardiophrenic + bronchial (visceral) | Intercostal veins + pulmonary veins (visceral) | Intercostal nerves (costal); Phrenic nerve (central diaphragmatic — shoulder-tip referral); Autonomic only (visceral — pain insensitive) |
| Bronchi/Trachea | Air conduction, warming, humidification, mucociliary clearance | Bronchial arteries from aorta + inferior thyroid (cervical trachea) | Bronchial veins → azygos/hemiazygos | Recurrent laryngeal, vagus, sympathetic T2–T5; carina = most sensitive cough trigger |
If you meant a different anatomical region (e.g., mediastinum, diaphragm, chest wall muscles, or a specific organ), please clarify and I'll cover it in detail.
This is a shared conversation. Sign in to Orris to start your own chat.