Pt with pulmonary embolism
Reading File
Asking for Preferences
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have comprehensive information across all domains. Let me compile the full overview.
Pulmonary Embolism (PE) - Full Clinical Overview
Pathophysiology
PE is a life-threatening manifestation of venous thromboembolism (VTE). In most cases, a thrombus originating from deep veins of the lower extremities detaches, travels through the right heart, and lodges in the pulmonary vasculature.
Virchow's Triad - the three predisposing factors:
- Hypercoagulability (thrombophilia, cancer, oral contraceptives, immobility)
- Venous stasis (prolonged immobilization, heart failure, post-surgical)
- Venous injury/inflammation (trauma, surgery, IV catheters)
Hemodynamic consequences:
- Obstruction of the pulmonary vascular bed raises pulmonary vascular resistance (PVR)
- Acute pulmonary hypertension causes right ventricular (RV) pressure overload and dilation
- The dilated RV compresses the interventricular septum, reducing LV filling ("D-sign")
- Decreased LV cardiac output leads to systemic hypotension and ischemia
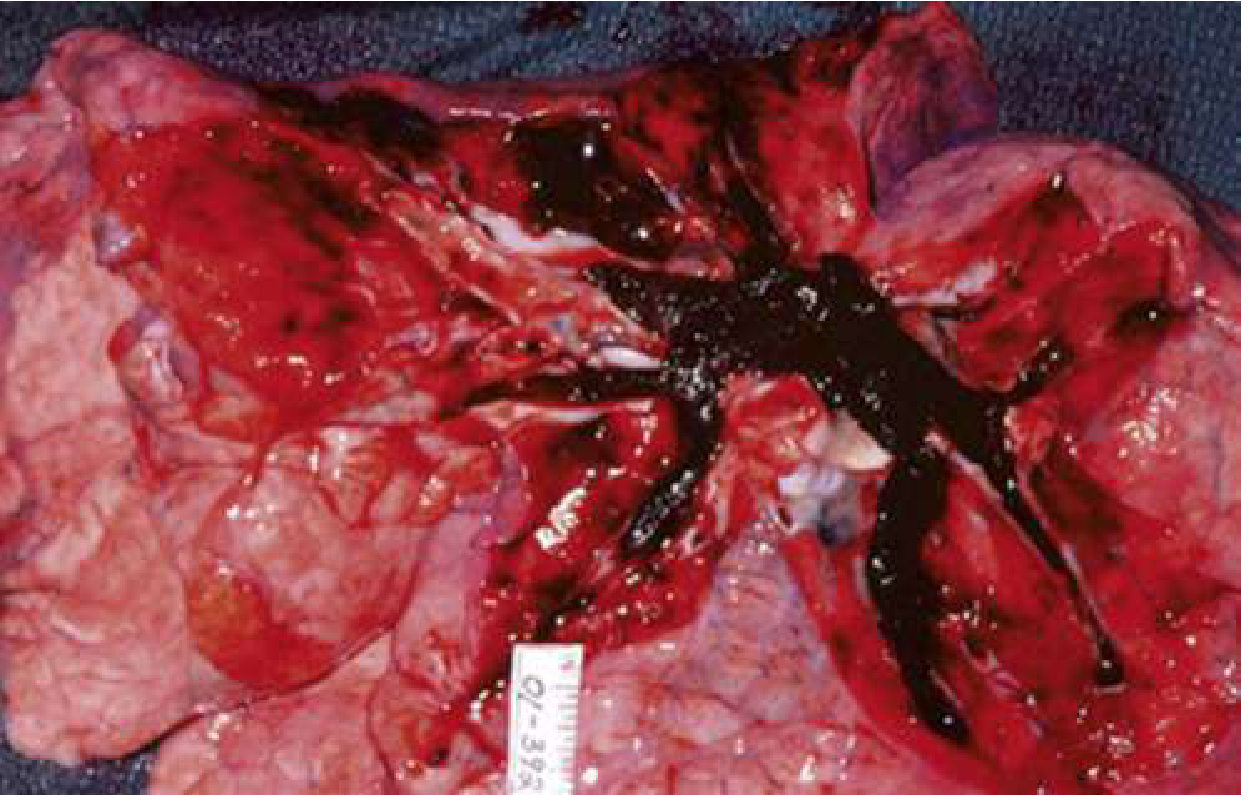
- In extreme cases, the thrombus can occlude the entire RV outflow system (as seen in the autopsy photo below), causing sudden cardiovascular collapse
Gas exchange effects:
- V/Q mismatch is the primary cause of hypoxemia
- Dead space ventilation increases (perfused segments lost)
- Reflex bronchoconstriction and atelectasis contribute
- Pulmonary infarction can occur in peripheral PE, producing pleuritic pain, hemoptysis, and fever
Risk Factors
| Category | Examples |
|---|---|
| Surgical/Trauma | Lower extremity surgery, prolonged procedures, pelvic trauma |
| Immobility | Prolonged bed rest, long-haul flights ("economy class syndrome") |
| Malignancy | Lung, brain, pancreas, leukemia - especially active/treated cancers |
| Thrombophilia (inherited) | Factor V Leiden, prothrombin G20210A mutation, antithrombin III deficiency, protein C/S deficiency |
| Thrombophilia (acquired) | Antiphospholipid syndrome |
| Hormonal | OCP, HRT, fertility drugs, anti-androgen prostate cancer therapy |
| Prior VTE | Strongest single predictor of recurrence |
| Pregnancy/Postpartum | 5x risk vs. age-matched controls; peaks postpartum especially after C-section |
| Obesity, smoking, age >35 | Modifiable/additive factors |
Clinical Presentation
PE is called the "great masquerader" because it can present across a wide spectrum:
Symptoms (most to least common):
- Dyspnea - 75-80% of patients; can be constant, exertional, or vague ("can't take a full breath")
- Chest pain - second most common; can be pleuritic (sharp, worse with inspiration - seen in ~20%) or non-pleuritic (dull, aching)
- Cough, hemoptysis - with pulmonary infarction (peripheral PE)
- Unilateral leg swelling/pain - present in <30%, but relatively specific when combined with dyspnea
- Syncope - <5% of syncope patients have PE, but unexplained syncope with risk factors should prompt evaluation
- Low-grade fever - if high fever (>38.6°C/101.5°F), consider pneumonia instead
Signs:
- Tachycardia (most common sign)
- Tachypnea, hypoxemia
- Hypotension/shock (massive PE)
- Loud P2, right-sided S3/S4, signs of RV failure (raised JVP, peripheral edema)
- PEA arrest is the most common ECG finding in PE-related cardiac arrest
Pearl: Approximately 25% of sudden cardiac deaths are attributed to PE.
Diagnosis & Workup
Step 1 - Estimate Pre-Test Probability (PTP)
Wells Score for PE:
| Criterion | Points |
|---|---|
| Clinical signs/symptoms of DVT | 3 |
| PE is #1 diagnosis OR equally likely | 3 |
| Heart rate >100 bpm | 1.5 |
| Immobilization ≥3 days or surgery in prior 4 weeks | 1.5 |
| Prior DVT or PE | 1.5 |
| Hemoptysis | 1 |
| Malignancy (treated within 6 months or palliative) | 1 |
- Low: <2 points | Moderate: 2-6 | High: >6
Revised Geneva Score (fully objective):
- Low: 0-3 | Intermediate: 4-10 | High: >10
Step 2 - Apply PERC Rule (if low gestalt PTP)
If all 8 criteria are met AND gestalt PTP is low, PE can be ruled out without further testing:
Age <50 | Pulse <100 | SaO2 >94% | No unilateral leg swelling | No hemoptysis | No recent trauma/surgery | No prior PE/DVT | No hormone use
Step 3 - D-Dimer
- Sensitivity 95-98%, specificity 40-55%
- Use in non-high PTP patients (Wells <6 or Geneva <5)
- Negative D-dimer effectively excludes PE (NPV 99-100%)
- Age-adjusted D-dimer threshold = age × 10 mcg/L (for patients >50 years) - increases specificity without sacrificing sensitivity
Step 4 - Imaging
CT Pulmonary Angiography (CTPA) - first-line imaging modality
- Visualizes emboli directly in pulmonary arteries
- Also shows RV dilation (ratio >0.9 signals intermediate/high risk)
- Preferred over V/Q in most patients
V/Q Scan - preferred when:
- Contrast allergy or renal impairment
- Pregnancy (lower fetal radiation vs. CTPA)
- Young women (lower breast radiation)
Compression Ultrasonography (CUS) - for DVT; if positive in a patient with high PE suspicion, may be sufficient to start treatment without CTPA
Echocardiography - NOT recommended for initial PE diagnosis; valuable for risk stratification once PE is confirmed (RV strain, septal shift, McConnell's sign)
Ancillary Tests
| Test | Utility |
|---|---|
| ECG | Sinus tachycardia most common; S1Q3T3, new RBBB, T-wave inversions V1-V4 suggest RV strain |
| Troponin (I or T) | Elevated = myocardial injury from RV ischemia; predicts worse prognosis |
| BNP/NT-proBNP | Elevated = RV strain; guides risk stratification |
| ABG | Hypoxemia, hypocapnia, respiratory alkalosis; elevated A-a gradient |
| CXR | Usually non-specific; Hampton's hump (wedge-shaped opacity), Westermark's sign (oligemia), atelectasis |
Risk Stratification
| Category | Criteria | Mortality |
|---|---|---|
| Low-risk (submassive) | Hemodynamically stable, no RV dysfunction, normal troponin/BNP | <1% |
| Intermediate-low | Stable, but elevated troponin OR BNP OR RV dysfunction on imaging | ~3-5% |
| Intermediate-high (submassive) | Stable, but BOTH troponin elevated AND RV dysfunction | ~10-15% |
| High-risk (massive) | Hemodynamic instability (SBP <90 or drop >40 mmHg for >15 min), or cardiac arrest | >30% |
Shock index >1 (HR > SBP) indicates hemodynamic compromise.
Management
Anticoagulation (cornerstone of treatment)
DOACs (Direct Oral Anticoagulants) - preferred for most patients:
- Rivaroxaban: 15 mg BID x 21 days, then 20 mg daily
- Apixaban: 10 mg BID x 7 days, then 5 mg BID
- Dabigatran or Edoxaban: require 5-10 days of parenteral heparin first
Heparin (IV UFH or LMWH):
- Use if thrombolysis or surgical intervention is planned
- UFH is preferred pre-thrombolysis (short half-life, reversible)
- LMWH (enoxaparin) preferred for cancer-associated PE
Duration of anticoagulation:
- Provoked PE (reversible risk factor): 3 months
- Unprovoked PE: minimum 3 months; consider extended if low bleeding risk
- Cancer-associated PE: long-term (DOAC or LMWH preferred)
Treatment by Risk Category
Low-Risk PE:
- DOAC anticoagulation
- Outpatient management appropriate if Hestia criteria negative or PESI class I-II
- Follow-up at 1-2 weeks
Intermediate-Risk PE:
- Hospital admission (monitored bed); anticoagulation (DOAC or heparin)
- Thrombolysis reserved for clinical deterioration
- Activate PERT (PE Response Team) if available
High-Risk (Massive) PE:
- IV UFH immediately
- Systemic thrombolysis (alteplase 100 mg IV over 2 hours) - if no contraindications
- Surgical embolectomy - if thrombolysis contraindicated or failed
- Catheter-directed therapy (CDT) - alternative in intermediate-high risk or thrombolysis contraindications
- ECMO - as bridge to definitive therapy in refractory shock
Hemodynamic & Supportive Care
- Supplemental O2: target SpO2 >90%; avoid hypoxic pulmonary vasoconstriction
- Avoid aggressive fluid resuscitation - small boluses (250-500 mL) only; excessive fluids worsen RV dilation and LV compression
- Vasopressors: norepinephrine first-line for hypotension; dobutamine as adjunct (may worsen hypotension if used alone)
- Avoid intubation if possible - positive pressure ventilation increases intrathoracic pressure, reduces preload, and can precipitate hemodynamic collapse in severe PE. If intubation is unavoidable, optimize hemodynamics before induction.
IVC Filter
- Indicated when anticoagulation is absolutely contraindicated AND PE risk is high
- Retrievable filters preferred
- Does NOT replace anticoagulation - resume as soon as safe
Special Populations
Pregnancy
- Risk is ~5x that of non-pregnant women; peaks postpartum (especially post-C-section)
- Increased coagulation factors (V, VIII, X, vWF) and decreased protein S
- D-dimer is unreliable (normally elevated in pregnancy)
- Pregnancy-adapted YEARS algorithm may help guide testing
- Imaging: V/Q (lower breast radiation) vs. CTPA - both acceptable; halve the perfusion dose for V/Q
- Treatment: LMWH throughout pregnancy and postpartum (warfarin teratogenic; DOACs not approved)
Cancer
- LMWH (e.g., dalteparin) or DOACs (rivaroxaban, apixaban) preferred over warfarin
- Duration: indefinite while cancer is active
- Outpatient management increasingly supported - see recent meta-analysis (PMID 39603673)
Prognosis & Long-Term Complications
- 30-day mortality: <2% low-risk, up to 30-65% in massive PE with cardiac arrest
- Post-PE syndrome: dyspnea, exercise intolerance, decreased quality of life in ~50% at 1 year
- Chronic thromboembolic pulmonary hypertension (CTEPH): occurs in 0.5-5% of survivors; workup with V/Q scan at 3-6 months if persistent symptoms; definitive treatment is pulmonary endarterectomy
- Recurrence: ~10% at 1 year, ~30% at 10 years for unprovoked PE
PE Response Teams (PERT)
Multidisciplinary teams (emergency medicine, pulmonology, cardiology, cardiac surgery, hematology, interventional radiology) that streamline decision-making for intermediate and high-risk PE. A 2025 meta-analysis (PMID 40258457) assessed outcomes associated with PERT activation in acute PE.
Sources: Rosen's Emergency Medicine (10e), Murray & Nadel's Textbook of Respiratory Medicine, Miller's Anesthesia (10e), PubMed 2024-2026 literature.
This is a shared conversation. Sign in to Orris to start your own chat.