Here is a thorough comparison of Nephrotic vs Nephritic Syndrome as presented in Robbins, Cotran & Kumar Pathologic Basis of Disease and Robbins & Kumar Basic Pathology.
Nephrotic vs Nephritic Syndrome
Definition and Core Concept
| Feature | Nephrotic Syndrome | Nephritic Syndrome |
|---|
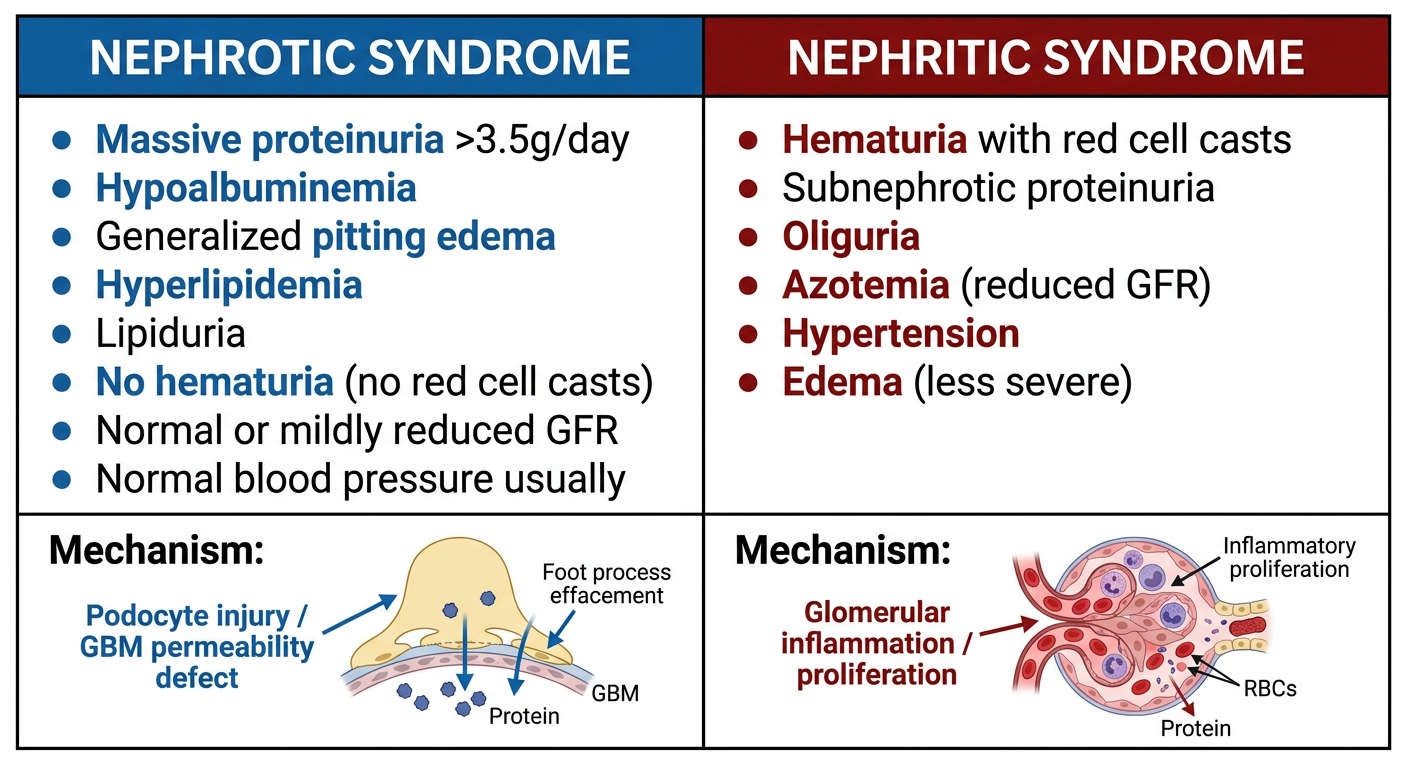
| Core defect | Increased GBM permeability to plasma proteins (podocyte/barrier injury) | Glomerular inflammation with capillary wall disruption |
| Key mechanism | Non-inflammatory - podocyte injury → protein leakage | Inflammatory - leukocyte infiltration + cell proliferation → GFR fall and bleeding |
Clinical Features (Robbins Table 20.3)
| Feature | Nephrotic Syndrome | Nephritic Syndrome |
|---|
| Proteinuria | Massive: >3.5 g/day (may be selective for low-MW proteins like albumin) | Subnephrotic (usually <3.5 g/day) |
| Hematuria | Absent or microscopic | Present - RBCs and RBC casts in urine (hallmark) |
| Edema | Generalized, soft, pitting - periorbital, dependent areas, may have ascites/pleural effusions | Present but less severe |
| Hypertension | Usually absent or mild | Present - due to fluid retention + renin release from ischemic kidneys |
| Azotemia | Absent or mild | Present - reduced GFR |
| Oliguria | Not a feature | Present |
| Hypoalbuminemia | Yes (<3 g/dL) - from urinary losses exceeding hepatic synthesis | Not prominent |
| Hyperlipidemia | Yes - increased cholesterol, TG, VLDL, LDL | Not a feature |
| Lipiduria | Yes (oval fat bodies, fatty casts) | Not a feature |
Table 20.3, Robbins Cotran & Kumar Pathologic Basis of Disease
Pathophysiology
Nephrotic Syndrome - Robbins explains:
The glomerular capillary wall (endothelium + GBM + podocytes) acts as a size and charge barrier. Structural or physicochemical alterations increase permeability, allowing proteins to escape:
- Massive proteinuria → heavy loss of albumin (and sometimes globulins)
- Hypoalbuminemia → hepatic compensatory synthesis cannot keep up; renal catabolism of filtered albumin also contributes
- Generalized edema → decreased intravascular colloid osmotic pressure + compensatory aldosterone secretion + sympathetic activation + reduced natriuretic factors → sodium and water retention
- Hyperlipidemia → compensatory increased hepatic lipoprotein synthesis (stimulated by hypoalbuminemia); decreased catabolism of lipoproteins (loss of lipoprotein lipase in urine)
- Lipiduria → lipoproteins pass through the damaged GBM
Selectivity of proteinuria: Highly selective = mostly albumin/transferrin (low MW); poorly selective = higher MW globulins also lost.
(Robbins, Cotran & Kumar, p. 844)
Nephritic Syndrome - Robbins explains:
The lesions share proliferation of glomerular cells + infiltration of inflammatory leukocytes. This inflammatory reaction:
- Severely injures capillary walls → blood passes into urine (hematuria)
- Induces hemodynamic changes → reduced GFR
- Reduced GFR → oliguria, fluid retention, azotemia
- Hypertension from fluid retention + renin release from ischemic kidneys
(Robbins, Cotran & Kumar, p. 840)
Morphology (Light/EM/IF)
| Feature | Nephrotic | Nephritic |
|---|
| Light microscopy | Variable - may appear normal (MCD), sclerosis (FSGS), GBM thickening (membranous) | Proliferative GN with leukocyte infiltration, sometimes crescents |
| Electron microscopy | Effacement (fusion) of podocyte foot processes - universal finding | Inflammatory deposits (subepithelial humps in poststreptococcal GN), GBM disruptions |
| Immunofluorescence | Granular (membranous) or negative (MCD) | Granular IgG/C3 (immune complex GN) or linear IgG (anti-GBM disease) |
Causes (Robbins)
Nephrotic Syndrome
| Cause | Notes |
|---|
| Minimal Change Disease | Most common in children; selective proteinuria; foot process effacement only on EM; responds well to steroids |
| Focal Segmental Glomerulosclerosis (FSGS) | Primary or secondary; focal/segmental scarring; often steroid-resistant; may progress to ESKD |
| Membranous Nephropathy | Most common cause of nephrotic syndrome in adults; autoimmune against PLA2R on podocytes; subepithelial deposits; "spike and dome" on EM |
| MPGN / C3 Glomerulopathy | Mixed nephrotic-nephritic picture; complement dysregulation |
| Diabetic nephropathy, Amyloidosis | Secondary causes |
Nephritic Syndrome
| Cause | Notes |
|---|
| Acute Poststreptococcal GN | Most common in children 6-10 yrs; Group A β-hemolytic streptococci (types 1, 4, 12); immune complex deposition in subepithelial spaces; "humps" on EM |
| Rapidly Progressive (Crescentic) GN | Severe nephritic syndrome + rapid renal failure; fibrinoid necrosis, GBM breaks, crescent formation |
| IgA Nephropathy | Most common GN worldwide; recurrent hematuria; IgA deposits in mesangium |
| Lupus nephritis (proliferative) | Can also have nephrotic features |
Summary Table (Robbins Basic Pathology - Table 12.2)
The Robbins Basic Pathology table specifically contrasts these presentations by disease:
- Nephrotic presentations: Minimal change disease, FSGS, Membranous nephropathy
- Mixed nephrotic/nephritic: MPGN, C3 glomerulopathy
- Nephritic presentation: Acute postinfectious GN, RPGN
- Hematuria without full syndrome: IgA nephropathy
Key Robbins Mnemonics to Remember
Nephrotic = "PAHHL" - Proteinuria (massive), Albumin low, Hyperlipidemia, Hypoalbuminemia, Lipiduria + Edema
Nephritic = "HAHOP" - Hematuria (RBC casts), Azotemia, Hypertension, Oliguria, Proteinuria (sub-nephrotic)
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease (10th ed.), pp. 832-845; Robbins & Kumar Basic Pathology, Table 12.2