Surgical appoches of ic fracture
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have excellent images and comprehensive text content. Now I can compose a detailed, well-structured answer on the surgical approaches for intertrochanteric (IT) fractures.
Surgical Approaches for Intertrochanteric (IT) Fractures
Intertrochanteric fractures (AO/OTA type 31-A) lie extracapsular between the greater and lesser trochanters. Because the blood supply to the femoral head is not at risk, these fractures are almost universally managed with internal fixation rather than arthroplasty (unlike displaced femoral neck fractures). The surgical approach is dictated by the chosen implant.
1. Patient Positioning (Common to All Approaches)
The patient is placed supine on a traction/fracture table (e.g., OSI, Stryker). The injured leg is secured in a traction boot; the contralateral limb is either:
- Lithotomy position - flexed, abducted, and held in a stirrup (image intensifier passes between the legs)
- Scissor position - contralateral leg extended to the side (image intensifier approaches from the opposite side)
The scissor position is preferred when contralateral hip motion is limited.

Fracture table is essential - fixation without it is not recommended as fracture reduction is difficult to maintain (Rockwood & Green's 10th Ed, p. 2714).
Reduction is achieved with longitudinal traction + slight internal rotation to reach an anatomical or slight valgus position (valgus reduces cut-out risk).
2. Approach A: Lateral Approach for Sliding Hip Screw (SHS/DHS) - Extramedullary Fixation
This is the standard approach for stable A1 fractures (and some A2).
Incision
- A 5-7 cm lateral longitudinal skin incision is made just distal to the greater trochanter, centered over the lateral femoral cortex
- The fascia lata (iliotibial band) is divided in line with the skin incision
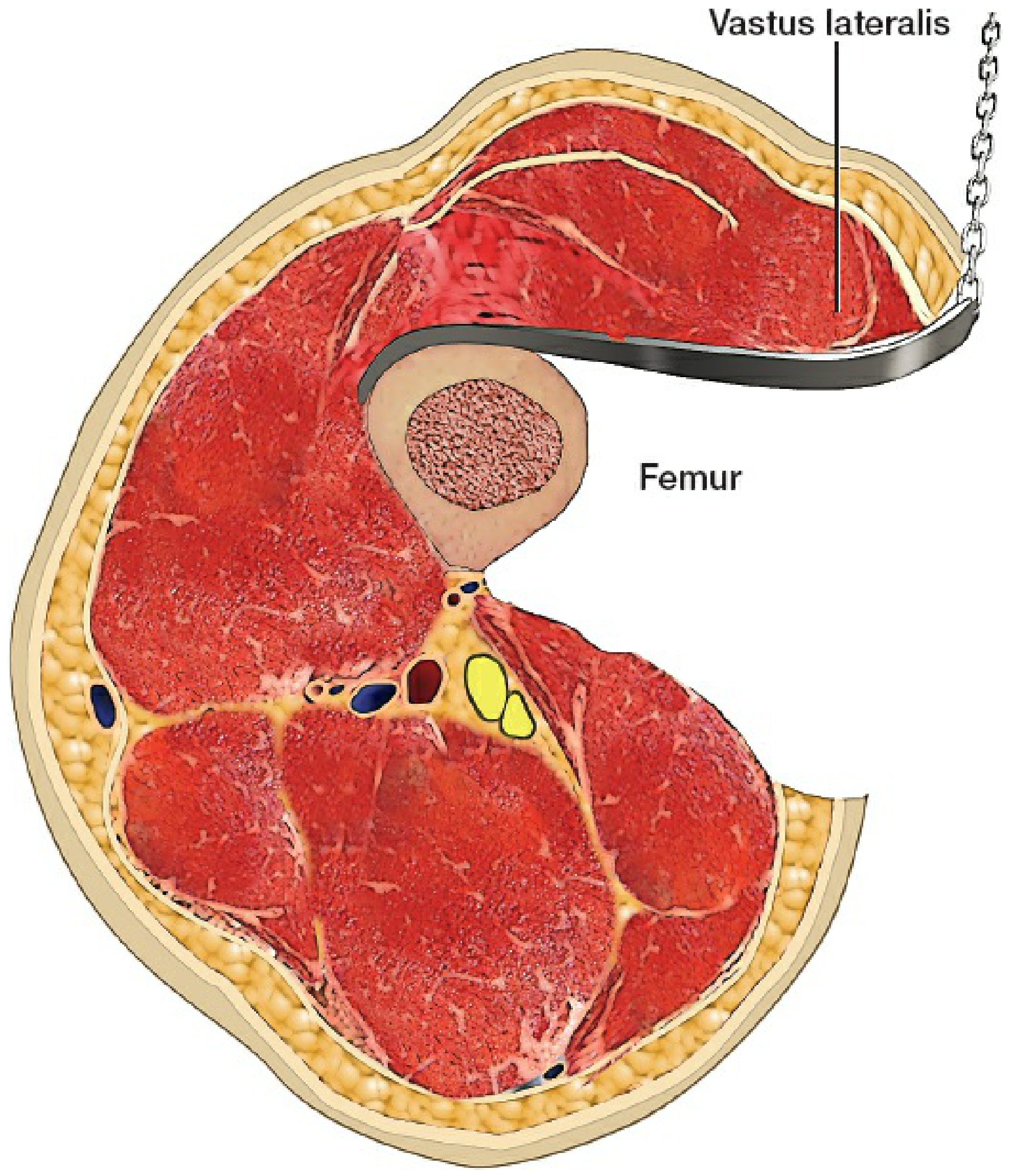
Muscle Handling - Vastus Lateralis
Two options:
- Retraction (preferred): Vastus lateralis is reflected anteriorly and held out of the way with a retractor attached to the support rail. This avoids splitting the muscle and reduces blood loss.
- Splitting: A direct split through the muscle belly is made if needed for access.
Key Surgical Steps (SHS)
- Supine on fracture table, fracture reduced under fluoroscopy (AP + lateral)
- 5-7 cm lateral incision just distal to greater trochanter
- Divide fascia lata; reflect vastus lateralis anteriorly
- Insert guidewire using an angle guide at 135° - aimed at central/low position on AP, central on lateral view
- Measure guidewire to determine lag screw length
- Ream over guidewire, insert lag screw - tip should be 5-7 mm from subchondral bone (tip-to-apex distance <25 mm)
- Ensure rotational alignment by palpating the anterior fracture line
- Apply barrel plate (usually 4-hole) to the lateral femur; fix with cortical screws
- Close vastus lateralis split (if split), close fascia lata, subcuticular skin closure
3. Approach B: Lateral/Proximal Lateral Approach for Cephalomedullary Nail (Intramedullary) - IMN
Used for unstable A2 and A3 fractures, reverse oblique fractures, and subtrochanteric extension. Implants include the PFNA, Gamma nail, TFN, and IMHS.
Incision
- A short 3-5 cm proximal lateral incision starting at the tip of the greater trochanter and extending proximally
- Fascia lata is divided
- Gluteus medius is split in line with its fibers (or retracted) to access the tip or piriform fossa of the greater trochanter (entry point depends on nail design)
Entry Point
- Greater trochanter entry nails (e.g., PFNA): entry at the tip of the greater trochanter, slightly medial
- Piriformis fossa entry nails (less common for IT fractures, more for subtrochanteric)
Key Surgical Steps (IMN)
- Supine on fracture table; closed reduction achieved under fluoroscopy
- Short proximal lateral incision at tip of greater trochanter
- Divide fascia lata; split or retract gluteus medius
- Open entry point with awl at tip of greater trochanter
- Pass guide rod down medullary canal; ream as required
- Insert nail to correct depth
- Insert cephalic lag screw or helical blade into femoral head via the nail's targeting arm - central/low on AP, central on lateral
- Insert distal locking screw(s) with freehand or targeting arm technique
- Close proximally in layers
Advantages Over SHS for Unstable Fractures
- Shorter lever arm - less bending moment
- Allows controlled collapse in anatomical position
- Less femoral medialization
- Norwegian Hip Fracture Registry (17,341 patients): lower reoperation rate and better 1-year mortality for unstable A2/A3 fractures with cephalomedullary nail vs SHS
4. Implant Selection by Fracture Type (AO/OTA Classification)
| Fracture Type | Stability | Recommended Implant |
|---|---|---|
| A1 (simple 2-part, intact medial wall) | Stable | SHS or cephalomedullary nail |
| A2 (comminuted, medial wall loss) | Unstable | Cephalomedullary nail (AAOS strong recommendation) |
| A3 (reverse oblique, lateral wall fracture) | Very unstable | Cephalomedullary nail |
| Subtrochanteric extension | Unstable | Long cephalomedullary nail |
AAOS guidelines: Either SHS or cephalomedullary device for stable A1; cephalomedullary nail strongly recommended for A2 and A3 (Rockwood & Green's 10th Ed, p. 2713).
UK NICE guidance: SHS acceptable for A1 and A2; no recommendation against cephalomedullary nail for A3.
5. Arthroplasty (Hemiarthroplasty/THA)
Although not a primary approach for IT fractures, hemiarthroplasty or THA may be considered in:
- Severely comminuted fractures in elderly patients with pre-existing arthritis
- Failed internal fixation (non-union, hardware failure)
- Pathological fractures
The approach in such cases is the posterior (Moore/Southern) approach or anterolateral (Watson-Jones) approach, similar to hip arthroplasty for femoral neck fractures.
6. Critical Technical Points
- Tip-to-apex distance (TAD): Should be <25 mm to minimize lag screw cut-out risk. Measured as the sum of distances from lag screw tip to femoral head apex on AP and lateral X-rays (corrected for magnification)
- Lag screw position: Central-inferior on AP, central on lateral (9-segment method) - inferior position reduces cut-out
- Anti-rotation: Prevent femoral head rotation during lag screw insertion by placing a finger on the anterior neck or using an anti-rotation pin
- Lateral wall integrity: If the lateral wall is deficient, a SHS risks failure - convert to cephalomedullary nail or add a trochanteric side plate
Source: Rockwood and Green's Fractures in Adults, 10th Ed. 2025, Chapter 54 (pp. 2713-2725)
This is a shared conversation. Sign in to Orris to start your own chat.