Management of hypotension
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypotension" AND "management"
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have comprehensive material from multiple authoritative sources. Let me compile the full response.
Management of Hypotension
Hypotension is defined as a systolic BP <90 mmHg, or a mean arterial pressure (MAP) <65 mmHg, or a drop in systolic BP >40 mmHg from baseline. Management depends critically on the underlying cause - classified into four shock types: hypovolemic, distributive, cardiogenic, and obstructive.
Step 1: Initial Assessment and General Principles
Regardless of cause, the immediate priorities are:
- Establish IV access; begin cardiac monitoring and pulse oximetry
- Assess blood glucose; provide oxygen supplementation
- Identify and treat the underlying cause simultaneously with resuscitation
- Target MAP ≥65 mmHg (in most contexts)
Step 2: Classify the Shock Type
| Type | Mechanism | Examples |
|---|---|---|
| Hypovolemic | Reduced preload / volume loss | Hemorrhage, dehydration, burns |
| Distributive | Vasodilation / maldistribution | Sepsis, anaphylaxis, neurogenic, drug-induced |
| Cardiogenic | Pump failure | MI, arrhythmia, myocarditis, valvular disease |
| Obstructive | Outflow obstruction | PE, tension pneumothorax, cardiac tamponade |
Step 3: Fluid Resuscitation
The first-line intervention in most types of hypotension (except cardiogenic) is IV fluids.
- Crystalloids (balanced saline, e.g. lactated Ringer's or normal saline) are the standard first choice
- In septic shock: 30 mL/kg IV crystalloid is recommended in the first 3 hours for patients with hypotension or lactate >2 mmol/L, though modern practice is shifting toward dynamic, individualized fluid assessment guided by fluid responsiveness rather than fixed-volume protocols
- Excessive fluid is harmful: positive fluid balance is associated with increased mortality and renal failure in septic shock
- Fluid responsiveness should be assessed using dynamic markers (pulse pressure variation, passive leg raise) before additional boluses
- Colloids have not been shown to be superior to crystalloids for most patients
"Vasopressors are typically initiated when hemodynamic stability cannot be restored with fluid administration alone." - Miller's Anesthesia, 10e
Step 4: Vasopressor Therapy
First-Line: Norepinephrine
- Mechanism: Stimulates α-adrenergic receptors (peripheral vasoconstriction) + β1 (inotropic stimulation), raising MAP
- Indication: First-line vasopressor for septic shock and acute hypotension refractory to fluids
- Dose: Titrated IV infusion (typically 0.01-3 mcg/kg/min)
- Adverse effects: Bradycardia, arrhythmias, peripheral ischemia
- Tintinalli's Emergency Medicine: "Norepinephrine is recommended as the initial vasopressor of choice for treatment of severe sepsis and septic shock refractory to adequate fluid resuscitation"
Second-Line / Add-on Agents
| Drug | Mechanism | Use | Notes |
|---|---|---|---|
| Vasopressin | V1 receptor - direct vasoconstriction; no inotropic/chronotropic effect | Add-on to norepinephrine in septic shock (up to 0.03 units/min) | Raises MAP or allows norepinephrine dose reduction; not recommended as sole initial vasopressor |
| Epinephrine | α + β1 + β2 stimulation | Second agent in septic shock when norepinephrine insufficient; first-line for anaphylaxis | Risk of arrhythmias and lactic acidosis |
| Phenylephrine | Selective α1 agonist | Hypotension in non-septic contexts; spinal anesthesia-related hypotension | Reflex bradycardia and reduced CO; not recommended in septic shock |
| Dopamine | Dose-dependent DA, β1, α receptor activation | No longer recommended as first-line for septic shock; associated with more arrhythmias | Indirect-acting; inferior to norepinephrine in most trials |
| Dobutamine | β1 > β2 agonist (inotrope) | Cardiogenic shock - augments contractility | Not a vasopressor; may worsen hypotension via vasodilation if used alone |
Step 5: Cause-Specific Management
Septic Shock (Distributive)
- 1-hour bundle: blood cultures, broad-spectrum antibiotics, 30 mL/kg crystalloid IV, vasopressors if MAP <65, lactate measurement
- Norepinephrine = first-line vasopressor
- Add vasopressin if norepinephrine dose escalating
- Corticosteroids (hydrocortisone 200 mg/day) reduce vasopressor requirements and aid shock reversal; mortality benefit less clear
- Source control where applicable (drain abscess, debride infected tissue)
Cardiogenic Shock
- Norepinephrine is the first-line vasoactive agent per current guidelines
- Add dobutamine or milrinone for inotropic support (improves cardiac output)
- Epinephrine, levosimendan, and milrinone are alternatives
- Intra-aortic balloon pump (IABP) or other mechanical circulatory support if refractory
- Treat underlying cause (urgent PCI for STEMI-related shock, cardioversion for arrhythmias)
Obstructive Shock
- Pulmonary embolism with hemodynamic instability: IV saline with caution (excessive fluids worsen RV failure), systemic thrombolysis or catheter-directed therapy; norepinephrine as vasopressor
- Tension pneumothorax: Immediate needle decompression followed by chest drain
- Cardiac tamponade: Emergency pericardiocentesis
Hypovolemic / Hemorrhagic Shock
- Rapid volume replacement with crystalloids; packed RBCs for hemorrhage
- Control the bleeding source
- Vasopressors are a temporary bridge; definitive management is volume and hemorrhage control
Anaphylactic Shock
- Epinephrine IM (0.3-0.5 mg, 1:1000) is the cornerstone treatment
- IV fluids, antihistamines, corticosteroids, and bronchodilators as adjuncts
- IV epinephrine infusion if refractory
Drug-Induced Hypotension (e.g., Antipsychotic Overdose)
- IV fluid resuscitation: 1-2 L crystalloid in adults (or 20-40 mL/kg in children)
- If refractory: direct-acting α-agonists (phenylephrine or norepinephrine) preferred
- Dopamine (indirect-acting) is not recommended after antipsychotic overdose
- Manage QT prolongation with IV magnesium sulfate 2 g if QTc >500 ms
Step 6: Orthostatic Hypotension (Chronic/Neurogenic)
This is a distinct entity (BP drop ≥20/10 mmHg on standing) usually from autonomic failure.
Non-pharmacologic first (mandatory):
- Patient education: rise slowly, avoid hot environments, large carbohydrate-rich meals, alcohol
- Increase salt intake (10-20 g/day) and fluid intake (2-2.5 L/day)
- Compression garments, postural countermaneuvers
- Elevate head of bed 30-45 degrees
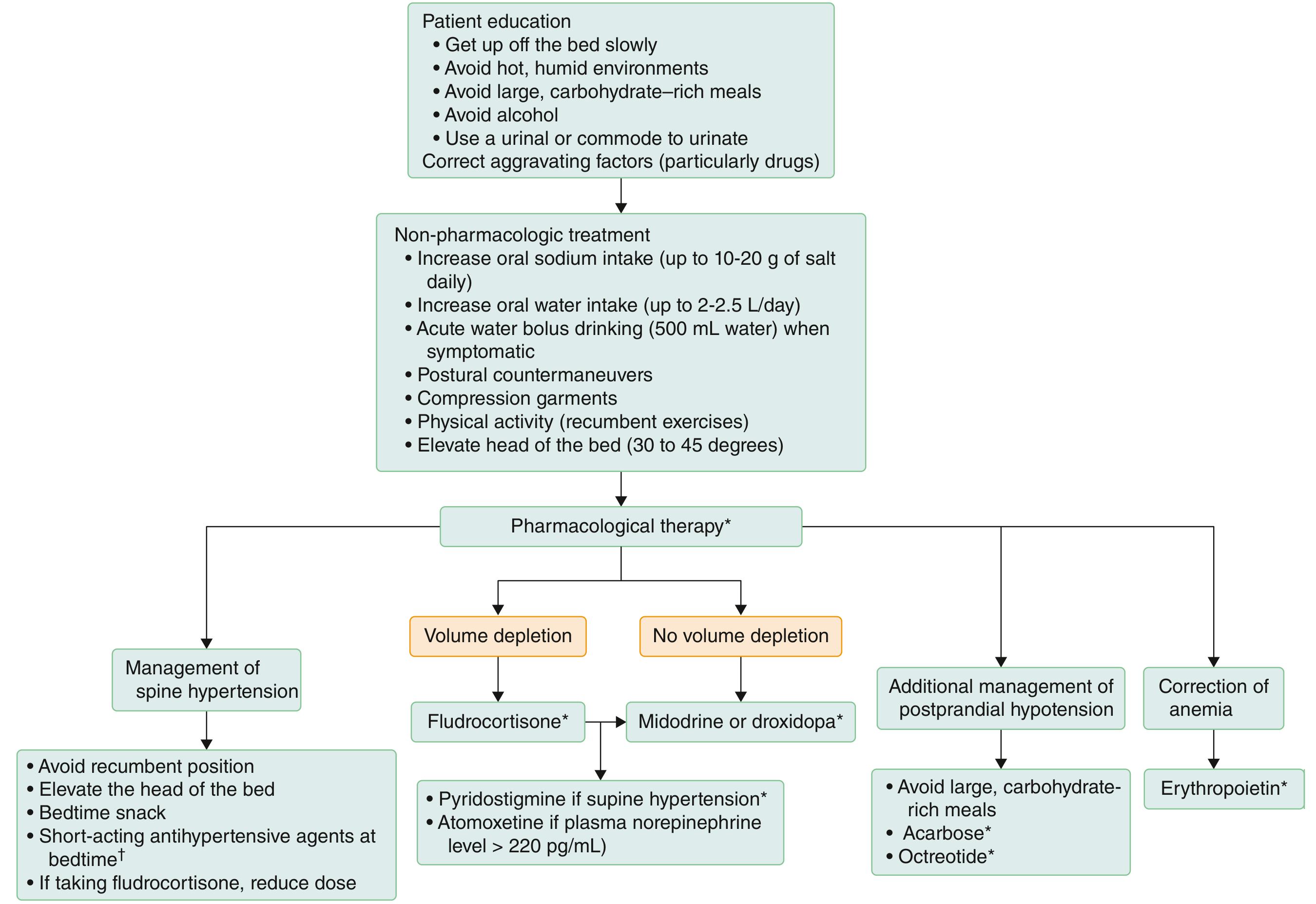
Pharmacologic therapy:
| Drug | Dose | Key Notes |
|---|---|---|
| Fludrocortisone | 0.1-0.2 mg oral daily | Volume expander; risk of supine hypertension and hypokalemia |
| Midodrine (α1 agonist) | 5-10 mg oral TID | Take before rising; no later than 3-4 hrs before bedtime |
| Droxidopa (norepinephrine precursor) | 100-600 mg oral TID | Same timing as midodrine; avoid supine use |
| Pyridostigmine | 30-60 mg TID | Useful when supine hypertension limits fludrocortisone/midodrine |
| Atomoxetine | 10-18 mg BID | Better for patients with preserved sympathetic terminals |
| Acarbose / Octreotide | Various | Adjuvant for postprandial hypotension |
| Erythropoietin | 25-75 U/kg SQ TIW | For anemia-driven worsening; requires iron supplementation |
- Goldman-Cecil Medicine
Monitoring Targets
| Parameter | Target |
|---|---|
| MAP | ≥65 mmHg (or higher in chronic hypertensives) |
| Urine output | ≥0.5 mL/kg/hr |
| Lactate | Trend to normalization (<2 mmol/L) |
| ScvO2 | >70% (if measured) |
Sources:
- Tintinalli's Emergency Medicine, Chapters 20, 15 (vasopressors, antipsychotic overdose)
- Miller's Anesthesia, 10e, Chapter 79 (sepsis/shock hemodynamic resuscitation)
- Goldman-Cecil Medicine, Chapter 366 (orthostatic hypotension)
- Rosen's Emergency Medicine, Frameworks for Internal Medicine (cardiogenic/obstructive shock)
Recent systematic review: Intraoperative hypotension management strategies (Lee et al., Anesth Analg 2025, PMID 38870081) confirms individualized blood pressure targets and vasopressor titration are superior to fixed thresholds in surgical patients.
This is a shared conversation. Sign in to Orris to start your own chat.