Anatomy of scarpas triangle with applied anatomy
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive content from the textbooks. Let me compile the full answer.
Scarpa's Triangle (Femoral Triangle) - Anatomy & Applied Anatomy
Scarpa's triangle is the clinical synonym for the femoral triangle - named after the Italian anatomist Antonio Scarpa. It is a wedge-shaped (triangular) depression formed by muscles in the upper anterior thigh at the junction between the anterior abdominal wall and the lower limb.
Boundaries
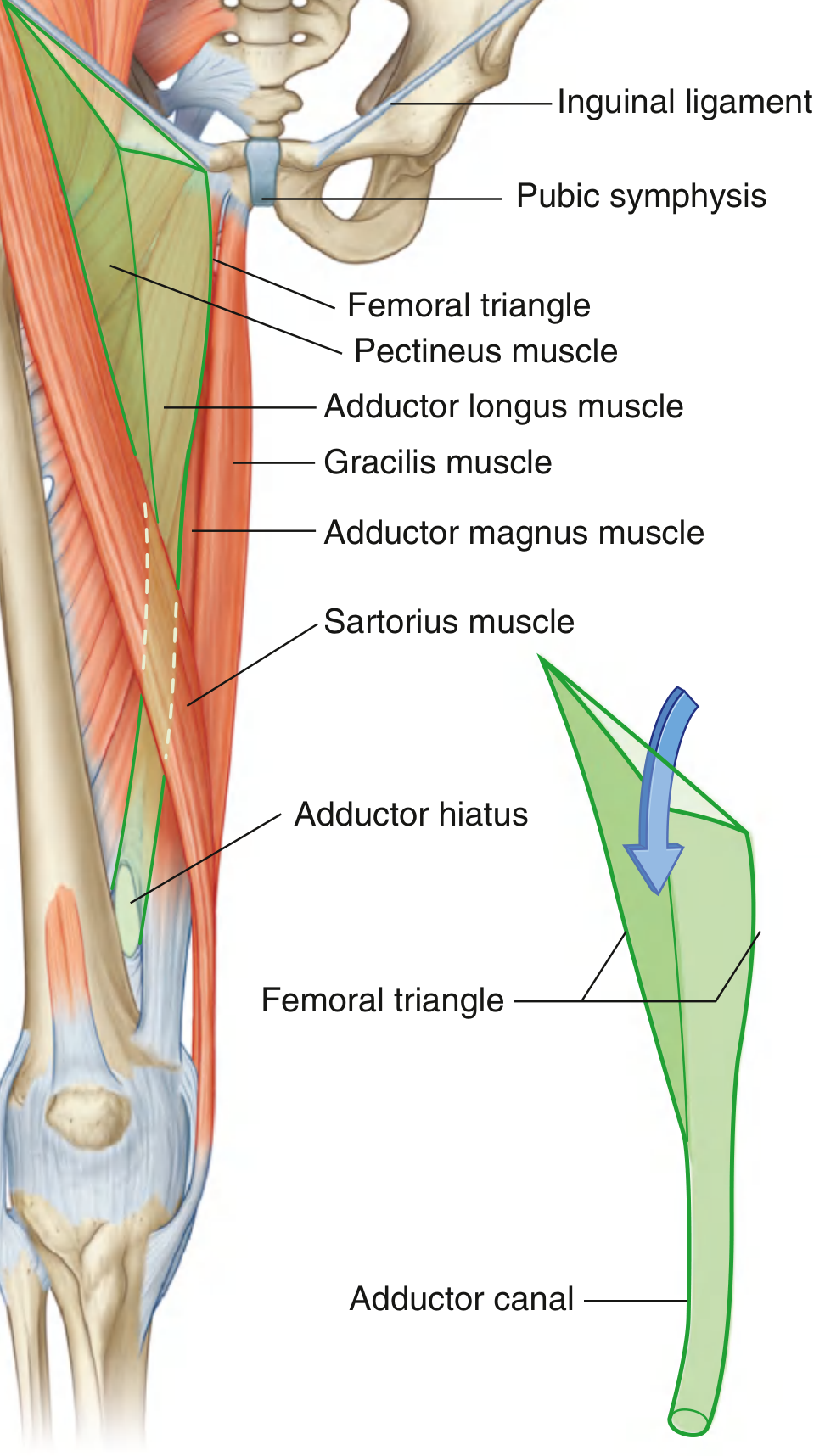
Fig. 6.42 - Boundaries of the Femoral Triangle (Gray's Anatomy for Students)
| Border | Structure |
|---|---|
| Base (superior) | Inguinal ligament (from ASIS to pubic tubercle) |
| Lateral border | Medial margin of the sartorius muscle |
| Medial border | Medial margin of the adductor longus muscle |
| Apex | Points inferiorly; where lateral and medial borders meet - continuous with the adductor canal |
Floor
The floor is formed by two muscles:
- Laterally: Iliopsoas muscle (descending from the abdomen)
- Medially: Pectineus and adductor longus muscles
Roof
- Fascia lata (deep fascia of the thigh), which is pierced by the great saphenous vein at the saphenous opening (fossa ovalis), covered by the cribriform fascia
- Overlying skin and subcutaneous fascia (superficial fascia = Camper's and Scarpa's layers)
Contents
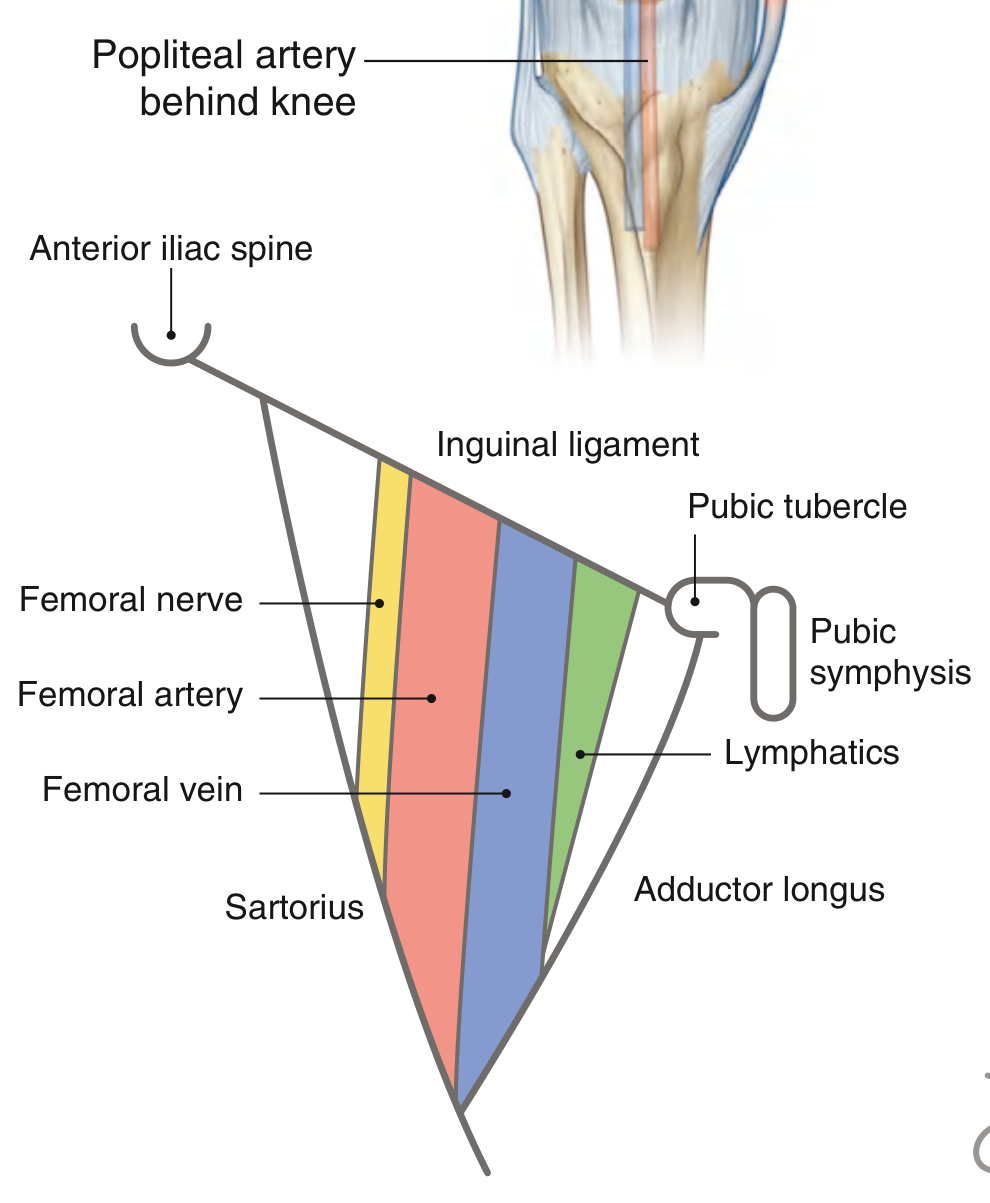
Fig. 6.43 - Contents of the Femoral Triangle (Gray's Anatomy for Students)
From lateral to medial (mnemonic: NAVY - Nerve, Artery, Vein, Y-fronts/lymphatics):
- Femoral nerve (L2, L3, L4) - lies outside the femoral sheath, most lateral
- Femoral artery - continuation of the external iliac artery; palpable just below the inguinal ligament at the midinguinal point (midpoint between ASIS and pubic symphysis)
- Femoral vein - drains into the external iliac vein; receives the great saphenous vein at the saphenofemoral junction
- Femoral canal (medial compartment) - contains lymphatics and the node of Cloquet/Rosenmüller; most medial structure
The Femoral Sheath
The femoral artery, vein, and femoral canal are enclosed within a funnel-shaped fascial sleeve - the femoral sheath:
- Continuous superiorly with the transversalis fascia (anteriorly) and iliac fascia (posteriorly)
- Contains three compartments: lateral (artery), middle (vein), medial (femoral canal with lymphatics)
- The femoral nerve is NOT enclosed within the sheath - it lies lateral to it
- The femoral canal's superior opening is the femoral ring, bounded:
- Anteriorly: inguinal ligament
- Posteriorly: pectineus muscle and its fascia
- Medially: lacunar (Gimbernat's) ligament
- Laterally: femoral vein
Apex and Continuation
The apex of the triangle points inferiorly and is continuous with the adductor canal (Hunter's canal), which descends medially down the thigh. The canal passes through the adductor hiatus in the adductor magnus to open into the popliteal fossa, where the femoral artery becomes the popliteal artery.
Applied Anatomy
1. Femoral Pulse and Vascular Access
The femoral artery is palpable in the femoral triangle just inferior to the inguinal ligament, midway between the pubic symphysis and the ASIS (midinguinal point). This is a critical landmark for:
- Emergency arterial/venous cannulation (femoral approach)
- Cardiac catheterization and coronary angiography/angioplasty
- Catheterization of cerebral, renal, gonadal vessels via femoral artery or vein
- Access to the right atrium, pulmonary artery, and superior vena cava via femoral vein
(Gray's Anatomy for Students, p. 675-676)
2. Femoral Hernia
A femoral hernia is a protrusion of extraperitoneal tissue and sometimes abdominal contents through the femoral canal. Key clinical points:
- Shape: Assumes a retort (flask) shape - remains narrow within the femoral canal, then bulges through the saphenous opening and turns upward, potentially extending above the inguinal ligament
- Location: Lies lateral to the pubic tubercle and below the inguinal ligament (distinguishes from inguinal hernia, which is medial to the pubic tubercle and above the inguinal ligament)
- Demographics: More common in women (2:1); right side more common (2:1); rare before age 20
- High strangulation risk: Because the femoral ring is bounded by rigid, unyielding structures (inguinal ligament, lacunar ligament, pectineus, femoral vein), the canal is rigid - femoral hernias strangulate frequently
- Differentiation from inguinal hernia: Cough impulse felt at the saphenous opening (~4 cm below and lateral to pubic tubercle); invagination test of the inguinal canal is negative
(S. Das Manual of Clinical Surgery, p. 611)
3. Aberrant Obturator Artery - Surgeon's Hazard
During femoral hernia repair, an aberrant obturator artery (a large pubic branch of the inferior epigastric artery replacing the normal obturator artery) may curve along the margin of the lacunar ligament. Inadvertent division can cause serious hemorrhage. This vessel forms the so-called "Crown of Death" (Corona Mortis) when encircling the femoral ring.
(Gray's Anatomy for Students, p. 790)
4. Femoral Lymph Nodes and Lymphatics
The deep inguinal lymph nodes, including the node of Cloquet (Rosenmüller) within the femoral canal, drain lymph from the lower limb and perineum. Enlarged nodes here may indicate:
- Lower limb infections or malignancy
- Pelvic or perineal tumors
- Lymphoma
5. Femoral Nerve Block
The femoral nerve lies just lateral to the femoral artery within the femoral triangle, outside the sheath. Ultrasound-guided femoral nerve block in the femoral triangle provides anesthesia/analgesia for the anterior thigh and knee - used in hip fracture pain management and knee surgery.
6. Saphenofemoral Junction (SFJ)
The great (long) saphenous vein drains into the femoral vein at the saphenofemoral junction within the femoral triangle, at the saphenous opening. This junction is ligated during surgery for varicose veins (Trendelenburg's operation).
7. Psoas Abscess
An abscess tracking down the iliopsoas muscle from a spinal infection (e.g., Pott's disease - TB spine) can present as a fluctuant swelling in the femoral triangle - a classic cold (psoas) abscess presenting below the inguinal ligament, which may be confused with a femoral hernia.
8. Femoral Artery Aneurysm and Pseudo-aneurysm
Repeated arterial cannulation (e.g., in IV drug users or post-catheterization) can lead to pseudo-aneurysm formation in the femoral triangle - presenting as a pulsatile, expansile mass at this site.
Summary Table
| Feature | Detail |
|---|---|
| Base | Inguinal ligament |
| Lateral border | Medial margin, sartorius |
| Medial border | Medial margin, adductor longus |
| Floor (lateral) | Iliopsoas |
| Floor (medial) | Pectineus + adductor longus |
| Roof | Fascia lata + cribriform fascia + skin |
| Contents (lat→med) | Femoral nerve, artery, vein, canal/lymphatics |
| Apex continues into | Adductor canal → popliteal fossa |
| Femoral artery pulse | Midinguinal point (midpoint ASIS-pubic symphysis) |
Sources:
- Gray's Anatomy for Students (9780323934237), p. 675-676, 790
- THIEME Atlas of General Anatomy and Musculoskeletal System (9781626237186), p. 573
- Fischer's Mastery of Surgery, 8e (9781975176433), p. 2012-2013
- S. Das A Manual on Clinical Surgery, 13th ed. (9788190568104), p. 611
This is a shared conversation. Sign in to Orris to start your own chat.