Rational use of division
Asking for Preferences
Digoxin in heart failure
Reading File
Finding Sources
Searching PubMed
"digoxin" AND "heart failure"
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive information from Braunwald's Heart Disease and other sources. Let me compile the full answer.
Digoxin in Heart Failure
Mechanism of Action
Digoxin is a cardiac glycoside derived from the foxglove plant (Digitalis lanata), first described by William Withering in 1775. It works through two main mechanisms:
-
Inhibition of Na+/K+-ATPase on cardiac myocytes - raises intracellular Na+, which reduces Na+/Ca2+ exchange activity, increasing intracellular calcium and thereby enhancing myocardial contractility (positive inotropy).
-
Sensitization of vagal afferent nerves - inhibits Na+/K+-ATPase in vagal afferents, increasing vagal tone. This counterbalances the heightened adrenergic activation seen in advanced heart failure and slows AV conduction. This is now considered the primary mechanism in HF, rather than the inotropic effect.
-
Renal effects - inhibits tubular Na+/K+-ATPase, mildly blunting sodium reabsorption.
- Braunwald's Heart Disease, Cardiac Glycosides section
Clinical Evidence: The DIG Trial
The landmark Digitalis Investigation Group (DIG) trial is the key reference:
- Result: Digoxin had a neutral effect on all-cause mortality but significantly reduced HF hospitalizations and favorably affected the combined endpoint of death or hospitalization for worsening HF.
- A trend toward decreased deaths from pump failure (p = 0.06) was offset by increased sudden and non-pump failure cardiac deaths (p = 0.04).
- Serum level is critical: Trough levels of 0.5-1.0 ng/mL are recommended. In men, levels of 0.6-0.8 ng/mL were associated with decreased mortality.
- Sex difference: A post-hoc analysis showed digoxin was associated with a ~23% higher all-cause mortality in women (not men), possibly due to weight-based dosing rather than trough level-based dosing.
- The DIG trial was conducted before widespread beta-blocker use; no large trial with contemporary GDMT (ACEi + beta-blocker + MRA + SGLT2i) exists.
- Braunwald's Heart Disease, p. 160-161
Rational Use in Heart Failure
Indications
| Indication | Class |
|---|---|
| Symptomatic HFrEF (NYHA II-IV) persisting despite ACEi/ARNi + beta-blocker + MRA + SGLT2i - to reduce hospitalizations | IIa |
| HFrEF with concurrent AF for rate control (especially when hemodynamics preclude beta-blockers/CCBs) | IIa |
| Acute rate control in AF with HF when other agents are unsafe | IIa |
Where Digoxin Fits in the Treatment Ladder
- First-line (guideline-directed medical therapy): ACEi/ARB or ARNi + beta-blocker + MRA + SGLT2i/2 inhibitor
- Digoxin is second/third-line: Added only when patients remain symptomatic on optimized GDMT, primarily to reduce hospitalizations.
- It does not reduce mortality and should never replace the four pillars of HFrEF therapy.
Dosing
- Standard maintenance dose: 0.125 mg/day (the dose of choice for most patients)
- Higher doses (0.25 mg/day) are rarely used and not recommended for HF in sinus rhythm or AF
- Target serum trough level: < 1.0 ng/mL (ideally 0.5-0.8 ng/mL)
- Dose must be adjusted for renal function (renally cleared): CL = 0.88 × CrCl + 0.33 mL/min/kg
- Oral bioavailability ~70%; therapeutic index is narrow (~2-3x)
- Goodman & Gilman's Pharmacological Basis, Box 2-4
Adverse Effects and Toxicity
The principal adverse effects form three categories:
| System | Manifestations |
|---|---|
| Cardiac | Heart block (especially elderly), AV block, ectopic/reentrant rhythms, ventricular arrhythmias |
| Neurologic | Visual disturbances (yellow-green halos/xanthopsia), disorientation, confusion |
| GI | Anorexia, nausea, vomiting (often early signs of toxicity) |
Factors that Increase Toxicity Risk
- Hypokalemia (most important - digoxin and K+ compete for the same ATPase binding site)
- Renal impairment (reduced clearance)
- Drug interactions: quinidine, verapamil, spironolactone, flecainide, propafenone, amiodarone all raise serum digoxin levels
- Elderly patients and women (lower lean body mass)
- Patients with advanced heart block (contraindicated without a pacemaker)
Treatment of Toxicity
- Purified Digoxin-specific Fab fragments (Digibind/DigiFab) for life-threatening toxicity - rapidly reverses toxicity
- Monitor serum K+ carefully, especially with concomitant aldosterone antagonists
- Braunwald's Heart Disease, p. 161
Current Perspective (2024-2026)
Recent systematic reviews and network meta-analyses confirm digoxin's role remains limited:
- A 2023 systematic review/meta-analysis in Curr Drug Targets specifically examined digoxin in HFpEF and found no clear benefit - it is generally not recommended in preserved ejection fraction HF.
- The 2024 JACC Heart Failure network meta-analysis of pharmacological treatments in HFmrEF/HFpEF similarly does not support digoxin in these populations.
- A 2025 expert consensus on digoxin toxicity highlights that toxicity remains a significant clinical concern and requires careful therapeutic drug monitoring.
- Overall use is declining due to equivocal trial data and the dominance of GDMT with mortality benefit.
Summary: Key Points for Rational Use
| Point | Detail |
|---|---|
| Role | Symptom control + hospitalization reduction; no mortality benefit |
| Population | HFrEF + symptomatic on GDMT; or HFrEF + AF for rate control |
| NOT for | HFpEF, asymptomatic LV dysfunction, replacing GDMT |
| Dose | 0.125 mg/day in most; target trough 0.5-1.0 ng/mL |
| Monitor | Serum level, renal function, serum K+ |
| Avoid with | Advanced AV block without pacemaker, hypokalemia, pregnancy |
| Watch interactions | Quinidine, amiodarone, verapamil raise digoxin levels |
From kdt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a comprehensive Katzung-based answer. Here is the full response:
Digoxin in Heart Failure - Katzung's Basic & Clinical Pharmacology (16th Ed.)
(Chapter 13: Drugs Used in Heart Failure)
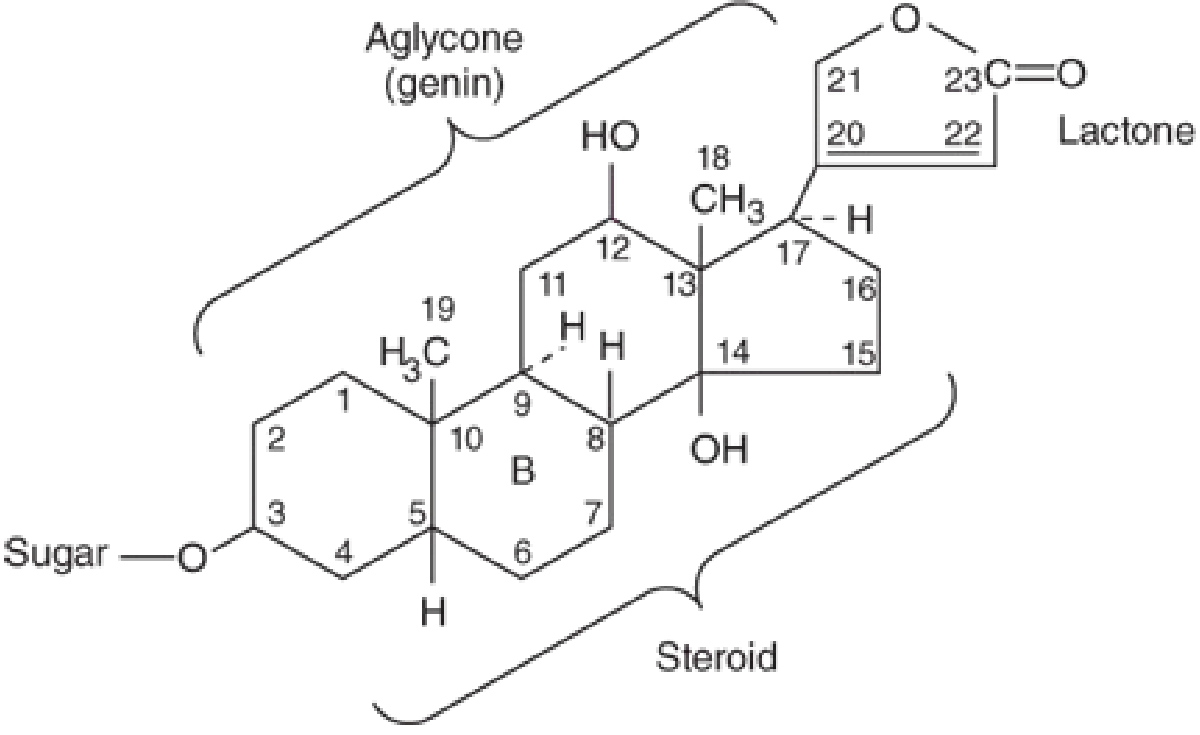
Chemistry
All cardiac glycosides (cardenolides) share a common structure: a steroid nucleus linked to a lactone ring at position 17 and sugars at carbon 3. The sugar-steroid-lactone combination is called the aglycone (genin). They lack ionizable groups, so solubility is not pH-dependent.
Digoxin is obtained from Digitalis lanata (white foxglove). Common plants like oleander, lily of the valley, and milkweed also contain cardiac glycosides.
Pharmacokinetics
| Parameter | Details |
|---|---|
| Oral bioavailability | 65-80% absorbed |
| Distribution | Wide, including CNS |
| Metabolism | Minimal; ~2/3 excreted unchanged by kidneys |
| Renal clearance | Proportional to creatinine clearance |
| Half-life | 36-40 hours (normal renal function) |
| Dose adjustment | Required in renal impairment (nomograms available) |
- Katzung, Chapter 13
Pharmacodynamics
A. Molecular Mechanism
Digoxin inhibits Na+/K+-ATPase (the sodium pump) in all tissues. This is responsible for both its therapeutic and toxic effects.
Two-step inotropic mechanism:
- Na+/K+-ATPase inhibition → ↑ intracellular Na+
- ↑ intracellular Na+ → reduced Ca2+ expulsion via Na+/Ca2+ exchanger (NCX) → ↑ intracellular Ca2+ → Ca2+ stored in SR → released during systole → ↑ contractility
Note: An endogenous digitalis-like steroid (possibly ouabain or marinobufagenin) is hypothesized to exist, given the highly conserved receptor on Na+/K+-ATPase.
B. Mechanical Effects (Figure 13-5)
In isolated myocardium, therapeutic concentrations produce:
- Increased rate of tension development and relaxation
- Little or no change in time to peak tension
- Increased contractility in both normal and failing myocardium
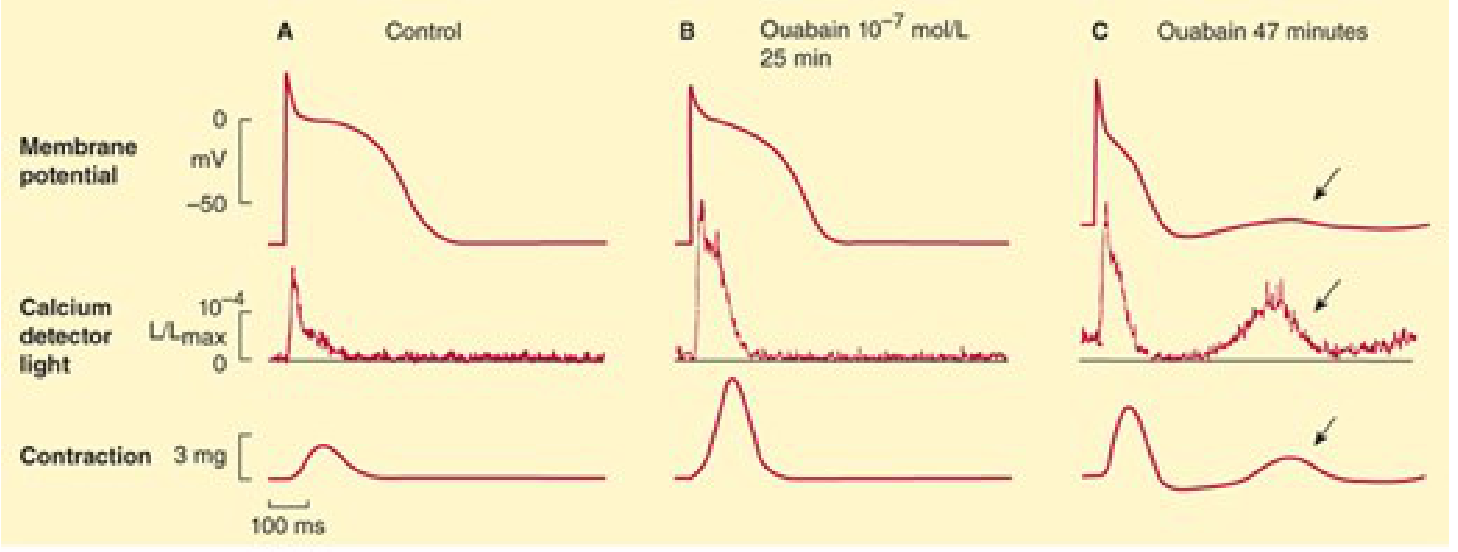
Panel A = Control. Panel B = Therapeutic dose (increased Ca2+, increased contraction). Panel C = Toxic dose (oscillatory depolarizations - Delayed After-Depolarizations/DADs appear, arrows).
C. Electrical Effects (Table 13-2 from Katzung)
| Tissue / Variable | Therapeutic Dose | Toxic Dose |
|---|---|---|
| Sinus node | ↓ Rate | ↓ Rate |
| Atrial muscle | ↓ Refractory period | ↓ Refractory period, arrhythmias |
| AV node | ↓ Conduction velocity, ↑ refractory period | ↓ Refractory period, arrhythmias |
| Purkinje / Ventricular | Slight ↓ refractory period | Extrasystoles, tachycardia, fibrillation |
| ECG | ↑ PR interval, ↓ QT interval | Tachycardia, fibrillation, arrest |
How toxicity causes arrhythmias: Toxic concentrations cause oscillatory Delayed After-Depolarizations (DADs) due to calcium overload in the SR. When DADs reach threshold, they trigger ectopic beats. Repeated DADs can cause bigeminy → ventricular tachycardia → ventricular fibrillation (rapidly fatal if uncorrected).
Autonomic (indirect) effects:
- Therapeutic doses: Cardioselective parasympathomimetic effect (vagal stimulation, baroreceptor sensitization, muscarinic facilitation) - primarily affects atria and AV node
- Toxic doses: ↑ sympathetic outflow - exaggerates all toxic effects
Most common cardiac toxic manifestations: AV junctional rhythm, PVCs, bigeminal rhythm, ventricular tachycardia, 2nd-degree AV block.
D. Interactions with Electrolytes
| Electrolyte | Effect on Digoxin |
|---|---|
| Hypokalemia | Enhances Na+/K+-ATPase inhibition → ↑ toxicity |
| Hyperkalemia | Inhibits Na+/K+-ATPase binding → ↓ toxicity |
| Hypercalcemia | Accelerates intracellular Ca2+ overload → ↑ arrhythmia risk |
| Magnesium | Opposite to calcium → protective |
- Katzung, Chapter 13
E. Extracardiac Effects
| System | Effects |
|---|---|
| GI tract (most common extracardiac toxicity) | Anorexia, nausea, vomiting, diarrhea (direct + CNS-mediated) |
| CNS | Vagal/chemoreceptor trigger zone stimulation; disorientation, hallucinations (elderly); visual disturbances (color perception aberrations - yellow-green) |
| Endocrine (rare) | Gynecomastia in men |
Clinical Pharmacology: Rational Use of Digitalis in HF
Indication
Digoxin is indicated in patients with:
- HF + atrial fibrillation (primary indication)
- Symptomatic HFrEF - only when diuretics and ACE inhibitors have failed to control symptoms
"Only about 50% of patients with normal sinus rhythm (usually those with documented systolic dysfunction) will have relief of heart failure from digitalis." - Katzung, Ch. 13
Dosing
| Method | Regimen |
|---|---|
| Slow loading (preferred) | 0.125-0.25 mg/day orally - safer, equally effective |
| Rapid digitalization (loading) | 0.5-0.75 mg IV/oral every 8 hours x 3 doses, then 0.125-0.25 mg/day |
Target serum concentration: ≤ 1 ng/mL
- Mortality is reduced at serum digoxin concentrations < 0.9 ng/mL
- Mortality is increased at concentrations > 1.5 ng/mL
- Higher concentrations may be needed in AF for rate control
What Digoxin Does and Does NOT Do
| Effect | Status |
|---|---|
| Reduce hospitalization | ✅ Yes (well established) |
| Reduce deaths from progressive HF | Trend toward ↓ (offset by ↑ sudden death) |
| Reduce all-cause mortality | ❌ Neutral overall (DIG trial) |
| Reduce symptoms | ✅ Yes (in ~50% with sinus rhythm) |
Katzung: "Although the net effect of the drug on mortality is mixed, it reduces hospitalization and deaths from progressive heart failure at the expense of an increase in sudden death."
Place in Therapy (ACC/AHA Stage C)
Digoxin is not first-line. The treatment ladder per Katzung is:
- Diuretics (furosemide, SGLT2 inhibitors) - first-line for congestion
- ACE inhibitors / ARBs / ARNIs - reduce preload, afterload, remodeling
- Beta-blockers (bisoprolol, carvedilol, metoprolol, nebivolol) - reduce mortality
- Aldosterone antagonists (spironolactone, eplerenone) - reduce mortality
- Digoxin - add when symptoms persist despite the above; primarily to reduce hospitalizations and for HF + AF
Summary Table (from Katzung Chapter 13)
| Feature | Digoxin |
|---|---|
| Drug class | Cardiac glycoside |
| Mechanism | Na+/K+-ATPase inhibition → ↑ intracellular Ca2+ → ↑ contractility + parasympathomimetic effect (slowed SA node, slowed AV conduction) |
| Effects | Positive inotropy, ↓ HR, ↓ AV conduction |
| Clinical use | Chronic symptomatic HF; rapid ventricular rate in AF; has NOT been shown to reduce mortality but does reduce rehospitalization |
| Pharmacokinetics | Oral/parenteral; half-life 36-40 h; renally cleared |
| Toxicity | Nausea, vomiting, diarrhea; cardiac arrhythmias (bigeminy, VT, VF, AV block); visual disturbances |
| Key interaction | Hypokalemia (↑ toxicity); quinidine, amiodarone, verapamil (↑ digoxin levels) |
- Katzung's Basic and Clinical Pharmacology, 16th Ed., Chapter 13
Which antiarhythmic drugs is used in vaentriculr tachycardia
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
This is a shared conversation. Sign in to Orris to start your own chat.