Hyperkalemia treatment
Reading File
Finding Sources
Searching PubMed
hyperkalemia treatment management
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of hyperkalemia treatment, organized by urgency.
Hyperkalemia Treatment
Overview
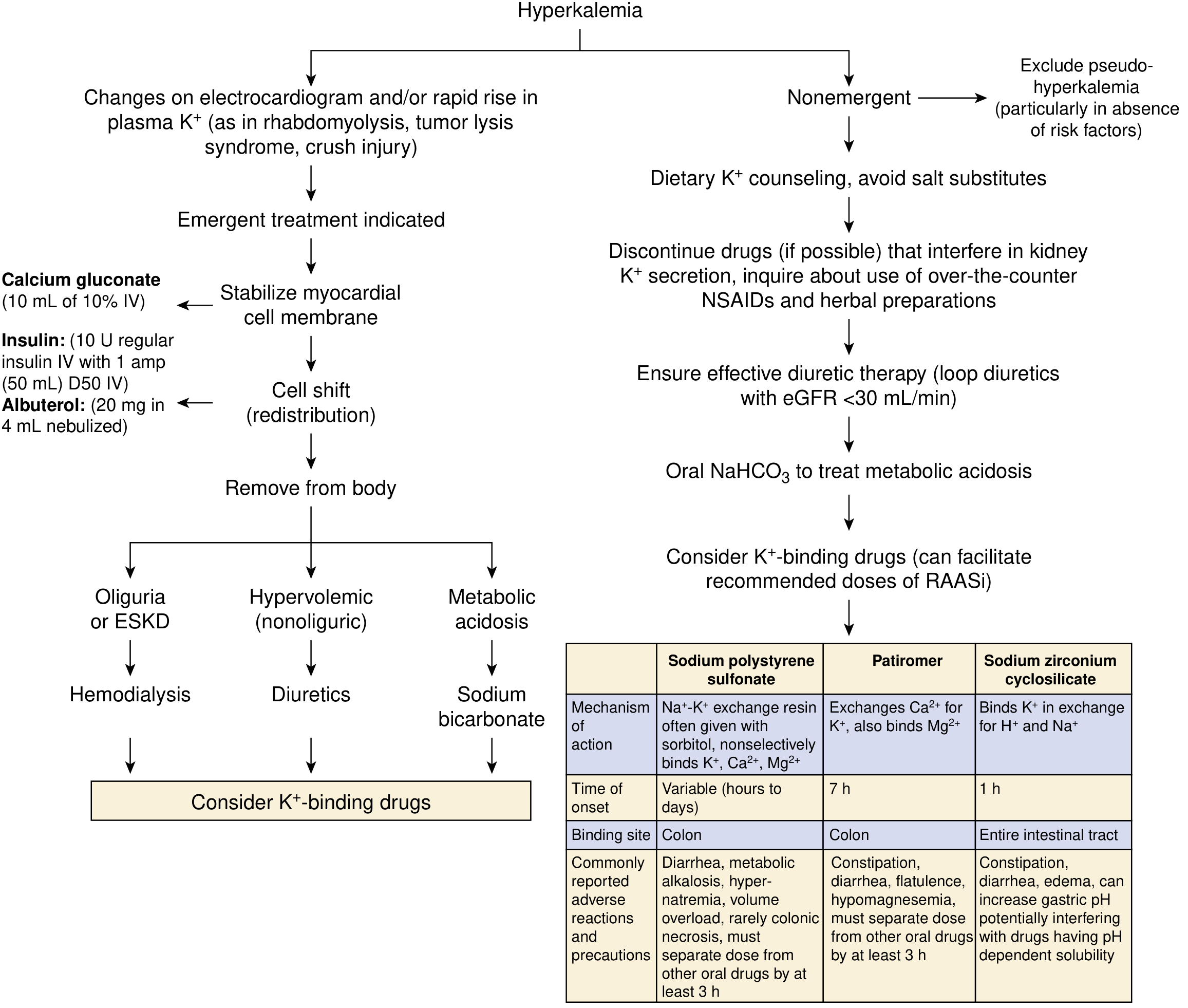
There is no single K⁺ threshold that defines "severe" hyperkalemia, but values >6–6.5 mEq/L or any ECG changes warrant emergency intervention. First, always stop all potassium infusions and identify/eliminate contributing causes (K⁺-sparing drugs, NSAIDs, dietary excess).
Treatment Algorithm
National Kidney Foundation Primer on Kidney Diseases, 8e
Emergent Treatment (ECG Changes Present)
Step 1 — Cardiac Membrane Stabilization
Calcium gluconate or calcium chloride — does not lower K⁺ but directly antagonizes cardiac membrane effects.
| Agent | Dose | Onset |
|---|---|---|
| Calcium gluconate 10% | 10 mL IV over 1–3 min | Near-immediate |
| Calcium chloride 10% | 3–5 mL IV | Near-immediate |
- Repeat in 3–5 minutes if no ECG improvement
- Prefer calcium gluconate peripherally (calcium chloride causes skin necrosis if it extravasates)
- Caution in digoxin toxicity — calcium potentiates digoxin cardiotoxicity
Step 2 — Intracellular Shift (Redistribution)
These agents lower plasma K⁺ temporarily; they do not remove K⁺ from the body.
Insulin + Glucose
- 10 units regular insulin IV + 50 mL of 50% dextrose (D50) bolus, then D5W infusion at 100 mL/hr to prevent late hypoglycemia
- Onset: ~15 minutes; monitor glucose closely (hypoglycemia is a common complication, especially in kidney failure)
- If glucose >300 mg/dL, insulin can be given without dextrose
- Never give dextrose alone — may worsen hyperkalemia if endogenous insulin is insufficient
Beta-2 Agonists (Albuterol)
- 20 mg nebulized albuterol over 10 minutes (concentrated 5 mg/mL formulation)
- Onset: ~30 minutes
- Effect is additive to insulin
- Note: the dose needed to lower K⁺ is much higher than for asthma
Sodium Bicarbonate
- Useful mainly when severe metabolic acidosis (HCO₃⁻ <10 mmol/L) is present
- 50–100 mEq IV over 10–20 minutes
- Does not enhance insulin or albuterol effects and has limited benefit without residual kidney function
Step 3 — Potassium Removal
Once cardiac membrane has been stabilized and redistribution initiated, definitive removal is required:
| Method | Indication | Notes |
|---|---|---|
| Loop diuretics | Adequate kidney function | Forced kaliuresis; thiazides can be added |
| Hemodialysis | AKI/ESKD, or refractory hyperkalemia | Definitive therapy; fastest removal |
| Potassium binders | Adjunct/chronic management | Slow onset; not for emergencies alone |
Non-Emergent / Chronic Management
For biochemical hyperkalemia without ECG changes:
- Dietary counseling — reduce high-K⁺ foods, avoid salt substitutes
- Discontinue offending drugs — ACE inhibitors, ARBs, K⁺-sparing diuretics, NSAIDs, trimethoprim
- Loop diuretics — especially with eGFR <30 mL/min
- Oral sodium bicarbonate — for underlying metabolic acidosis
- Potassium binders (see below)
Potassium Binders (Chronic)
| Agent | Mechanism | Onset | Key AEs |
|---|---|---|---|
| Sodium polystyrene sulfonate (SPS/Kayexalate) | Na⁺–K⁺ exchange resin in colon | Hours to days | Colonic necrosis (rare, especially with sorbitol), hypernatremia, metabolic alkalosis |
| Patiromer | Ca²⁺–K⁺ exchange in colon | ~7 hours | Constipation, hypomagnesemia; separate from other oral drugs by 3 hrs; start 8.4 g once daily |
| Sodium zirconium cyclosilicate (SZC) | Binds K⁺ in exchange for H⁺/Na⁺; entire GI tract | ~1 hour | Constipation, edema, may raise gastric pH |
- SPS has an FDA black box warning for intestinal necrosis — avoid in patients with abnormal bowel function
- Patiromer and SZC are FDA-approved for chronic hyperkalemia; neither should be used as sole emergency therapy
- SZC has 9× higher K⁺-binding capacity per gram than SPS
- Patiromer reduces K⁺ by ~1 mmol/L in CKD patients on RAASi therapy; SZC reduces by ~0.5–1 mEq/L
Special Situations
- Hypoaldosteronism: treat with fludrocortisone
- Digoxin use: avoid calcium salts if possible; calcium potentiates digoxin toxicity
- Pre-operative/perioperative: elective surgery contraindicated with significant hyperkalemia; avoid succinylcholine (can worsen K⁺) and K⁺-containing IV fluids
- Metabolic acidosis: bicarbonate promotes cellular uptake and enhances renal K⁺ excretion
- Massive transfusion: β-agonists (e.g., low-dose epinephrine infusion) are useful
Sources: National Kidney Foundation Primer on Kidney Diseases, 8e | Morgan & Mikhail's Clinical Anesthesiology, 7e | Sabiston Textbook of Surgery, 11e
This is a shared conversation. Sign in to Orris to start your own chat.