I have my university exam of 1 st year of subject physiology These are the important long answer give me answer of this question "Short-term & long-term regulation of blood pressure" and remeber it's a long question
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the content I need to write a complete, exam-quality long answer. Let me compile the full response.
Short-Term & Long-Term Regulation of Blood Pressure
Sources: Guyton and Hall Textbook of Medical Physiology; Costanzo Physiology 7th Edition
INTRODUCTION
Blood pressure (BP) is the driving force for blood flow to all tissues, and the body must maintain mean arterial pressure (Pa) at approximately 100 mm Hg at all times. BP is governed by the fundamental equation:
Mean Arterial Pressure (Pa) = Cardiac Output (CO) × Total Peripheral Resistance (TPR)
Since BP can be altered by changing CO, TPR, or both, the body uses a hierarchy of overlapping control mechanisms that operate at different speeds:
- Short-term (rapid) regulators - act within seconds to minutes (neural mechanisms)
- Intermediate-term regulators - act within minutes to hours (hormonal mechanisms)
- Long-term regulators - act over days to weeks (renal-body fluid mechanisms)
PART I: SHORT-TERM REGULATION OF BLOOD PRESSURE
Short-term regulation is primarily neural and operates through rapid reflex arcs involving the autonomic nervous system.
1. BARORECEPTOR REFLEX (Most Important Short-Term Mechanism)
This is the single most important rapid BP regulator, operating within seconds.
Location of Baroreceptors
- Carotid sinus baroreceptors - located in the wall of the internal carotid artery just above the bifurcation of the common carotid artery; respond to both increases and decreases in pressure
- Aortic arch baroreceptors - located in the aortic arch; respond primarily to increases in pressure (operate at pressures ~30 mm Hg higher than carotid receptors)
Nature of Baroreceptors
Baroreceptors are mechanoreceptors (stretch receptors). An increase in arterial pressure increases stretch on the vessel wall, which depolarizes the receptor and increases action potential frequency in afferent nerves. They respond maximally to pressures between 60-180 mm Hg and are most sensitive at the normal operating range of ~100 mm Hg.
Important: Baroreceptors are more sensitive to rate of change of pressure than to static pressure. A rapidly rising pressure causes a firing rate twice that seen with a stationary pressure at the same level.
Afferent Pathway
- From carotid sinus: via Hering's nerve -> Glossopharyngeal nerve (CN IX) -> Nucleus Tractus Solitarius (NTS) in medulla
- From aortic arch: via Vagus nerve (CN X) -> NTS in medulla
Vasomotor Center (Integration Center)
Located in the reticular formation of the medulla and lower pons, it has:
- Vasoconstrictor area (C1 area) - in anterolateral upper medulla; tonically active; sends sympathetic impulses via spinal cord
- Vasodilator area - in anterolateral lower medulla; inhibits the vasoconstrictor area
- Sensory area (NTS) - receives baroreceptor signals; primary integration site
Response to INCREASED Blood Pressure
When BP rises above normal:
- Baroreceptors are stretched more -> increased firing rate in carotid sinus nerve
- NTS is activated -> inhibits vasoconstrictor area and excites vagal center
- Parasympathetic outflow increases to SA node -> Heart rate decreases
- Sympathetic outflow decreases:
- To SA node -> heart rate decreases further
- To myocardium -> contractility decreases -> stroke volume falls -> CO decreases
- To arterioles -> vasodilation -> TPR decreases
- To veins -> venodilatation -> increased venous capacitance -> decreased venous return
- Net result: CO decreases + TPR decreases -> Pa falls back toward normal
Response to DECREASED Blood Pressure (e.g., Hemorrhage)
The exact opposite:
- Decreased stretch -> decreased baroreceptor firing
- NTS reduces inhibition of vasomotor center -> increased sympathetic outflow + decreased parasympathetic outflow
- Heart rate increases, contractility increases -> CO increases
- Arteriolar vasoconstriction -> TPR increases
- Venoconstriction -> venous return increases (Frank-Starling mechanism)
- Net result: Pa rises back toward normal
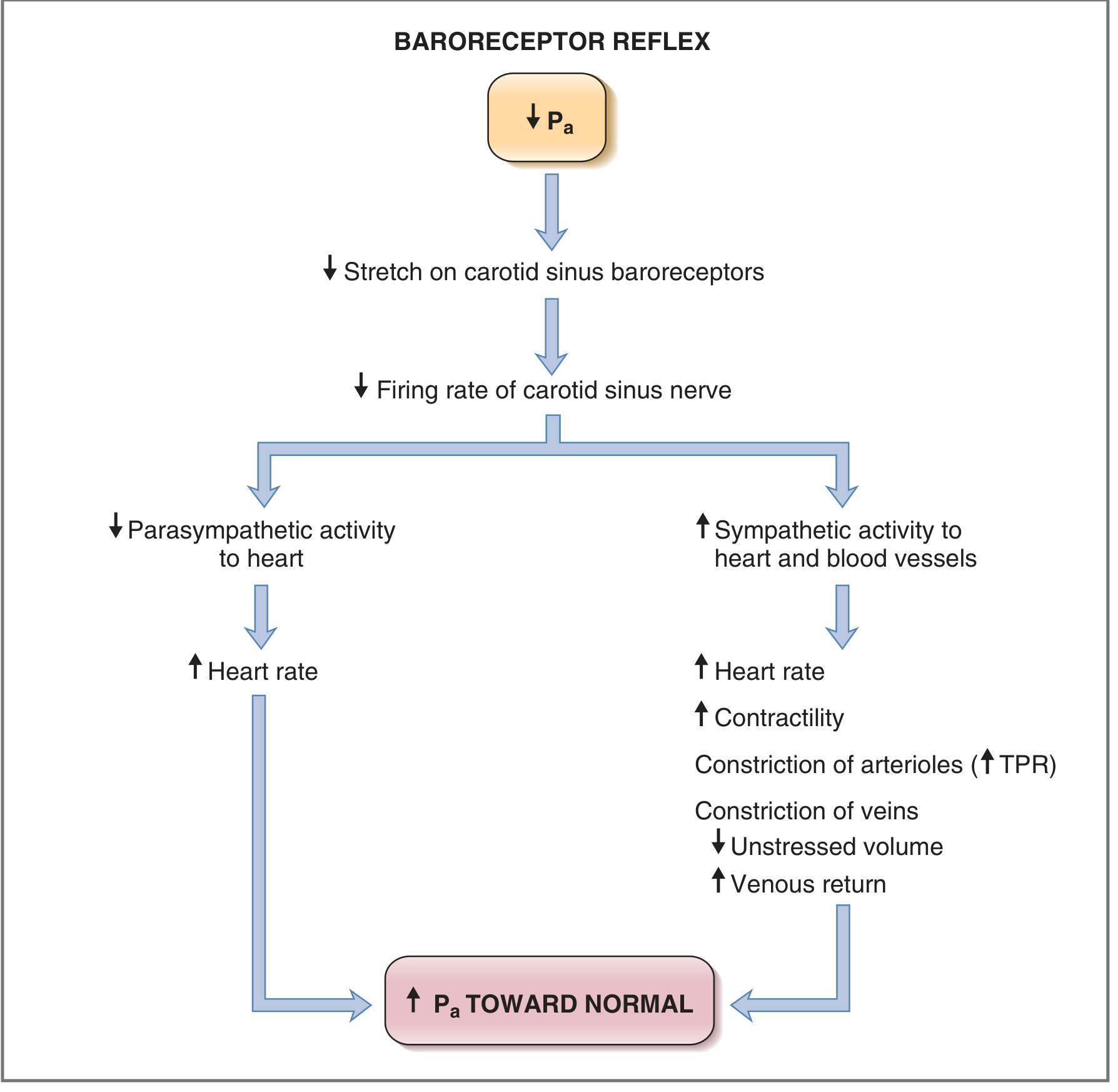
Fig: Baroreceptor reflex response to acute hemorrhage (decreased Pa). (Costanzo Physiology)
Limitation of Baroreceptor Reflex
- Baroreceptors adapt within 1-2 days to sustained changes in BP (resetting)
- In chronic hypertension, baroreceptors reset to the higher level, and the reflex then defends the new, elevated pressure instead of correcting it
- Therefore, they are not effective for long-term BP regulation - only short-term
2. CHEMORECEPTOR REFLEX
Peripheral chemoreceptors are located in the carotid bodies (near carotid bifurcation) and aortic bodies (along aortic arch). They have extremely high blood flow relative to their metabolic needs.
Stimulus
- Primarily respond to decreased PO2 (hypoxia)
- Also respond to increased PCO2 and decreased pH (especially when combined with low PO2)
Response
When O2 falls (as in severe hypotension reducing blood flow):
- Increased firing -> activates sympathetic vasoconstrictor centers
- Arteriolar vasoconstriction in skeletal muscle, renal, and splanchnic beds
- Transient bradycardia (quickly overcome by secondary respiratory stimulation causing tachycardia)
- Net effect: vasoconstriction -> increased TPR -> increased BP
This reflex is activated most powerfully when BP falls below ~80 mm Hg and serves as a backup system when baroreceptors are less effective.
3. CNS ISCHEMIC RESPONSE (Cushing Reflex)
When blood flow to the vasomotor center in the medulla becomes severely reduced (systolic BP < 60 mm Hg):
- CO2 accumulates in the vasomotor center, strongly exciting it
- Results in the most powerful sympathetic stimulation in the entire body
- Can raise systolic BP to as high as 250 mm Hg
- This is an emergency, last-resort mechanism
Cushing Reaction: A special type where increased cerebrospinal fluid (CSF) pressure compresses cerebral arteries -> brain ischemia -> vasomotor center activation -> BP rises until cerebral perfusion is restored.
4. OTHER SHORT-TERM MECHANISMS
Stress Relaxation and Reverse Stress Relaxation
- When BP suddenly increases, blood vessels gradually relax (stress relaxation) over minutes, allowing increased volumes without proportional pressure rise
- When BP falls, vessels constrict (reverse stress relaxation) to maintain pressure
Capillary Fluid Shift Mechanism
- When BP rises, increased capillary hydrostatic pressure pushes fluid from capillaries into interstitial spaces, reducing blood volume and therefore reducing BP
- When BP falls, fluid is drawn from interstitium back into capillaries, partly restoring blood volume
PART II: INTERMEDIATE-TERM REGULATION (Minutes to Hours)
1. RENIN-ANGIOTENSIN-ALDOSTERONE SYSTEM (RAAS)
The RAAS begins to act within minutes and reaches full effect over hours to days.
Trigger
- Decreased BP (decreased renal perfusion pressure)
- Decreased Na+ delivery to macula densa
- Increased sympathetic stimulation of JG cells
Cascade
- Juxtaglomerular (JG) cells in the afferent arteriole secrete renin
- Renin cleaves angiotensinogen (made by liver) -> Angiotensin I (inactive decapeptide)
- Angiotensin I is converted by ACE (Angiotensin Converting Enzyme, found mainly in pulmonary endothelium) -> Angiotensin II (active octapeptide)
Actions of Angiotensin II
| Action | Effect on BP |
|---|---|
| Powerful arteriolar vasoconstriction | Increases TPR -> increases Pa |
| Stimulates aldosterone release from adrenal cortex | Na+ and water retention -> increases blood volume |
| Acts on hypothalamus | Increases thirst (polydipsia) |
| Acts on posterior pituitary | Increases ADH release -> water retention |
| Constricts efferent arteriole more than afferent | Maintains GFR during hypotension |
| Directly stimulates Na+ reabsorption in proximal tubule | Increases blood volume |
Aldosterone Actions
- Released from zona glomerulosa of adrenal cortex
- Acts on principal cells of collecting duct and distal tubule
- Increases Na+ reabsorption and K+ excretion
- Water follows Na+ osmotically -> increased ECF volume -> increased blood volume -> increased BP
2. ADH (Vasopressin) - ANTIDIURETIC HORMONE
- Released from posterior pituitary in response to increased plasma osmolarity, decreased blood volume, or Angiotensin II
- Acts on V2 receptors in collecting duct -> inserts aquaporin-2 (AQP2) channels -> water reabsorption
- At high concentrations, also acts on V1 receptors on vascular smooth muscle -> vasoconstriction (hence the name vasopressin)
- Net effect: water retention -> increased blood volume -> increased BP
3. ATRIAL NATRIURETIC PEPTIDE (ANP) - Antagonizes RAAS
- Released from atrial cardiomyocytes when atria are stretched (indicating increased blood volume/pressure)
- Causes vasodilation of afferent arterioles
- Increases GFR and inhibits Na+ reabsorption
- Inhibits renin and aldosterone secretion
- Net effect: natriuresis and diuresis -> decreased blood volume -> decreased BP
- Acts as a counter-regulatory hormone opposing the RAAS
PART III: LONG-TERM REGULATION OF BLOOD PRESSURE
Long-term regulation (days to weeks) is primarily the function of the kidneys, working through the renal-body fluid system (pressure natriuresis and diuresis).
1. RENAL-BODY FLUID SYSTEM (Pressure Natriuresis & Diuresis)
This is the most powerful and the only truly infinite gain mechanism for BP control.
Basic Principle
If blood volume increases and arterial pressure rises, the kidneys excrete the excess salt and water (pressure natriuresis and pressure diuresis), returning BP toward normal. This feedback loop has essentially infinite gain - it will not stop correcting until BP is back to exactly the set point.
Pressure Natriuresis
- A small increase in arterial pressure (as little as a few mm Hg) causes a doubling of urinary sodium output (natriuresis) and water output (diuresis)
- This is mediated by:
- Increased GFR
- Decreased proximal tubule Na+ reabsorption
- Decreased loop of Henle reabsorption
- Reduced Angiotensin II and aldosterone activity
- Reduced sympathetic activity to kidneys
Quantitative Relationship
- At Pa = 50 mm Hg: urine output nearly zero
- At Pa = 100 mm Hg: normal urine output
- At Pa = 200 mm Hg: urine output 4-6 times normal
Chronic vs. Acute Renal Output Curve
The chronic renal output curve is much steeper than the acute curve (see diagram below), because chronic pressure elevation also:
- Decreases sympathetic activity (via baroreceptor resetting)
- Reduces Angiotensin II and aldosterone levels
This means in the long term, even large changes in salt intake cause only minimal changes in blood pressure in healthy individuals with normal kidneys.
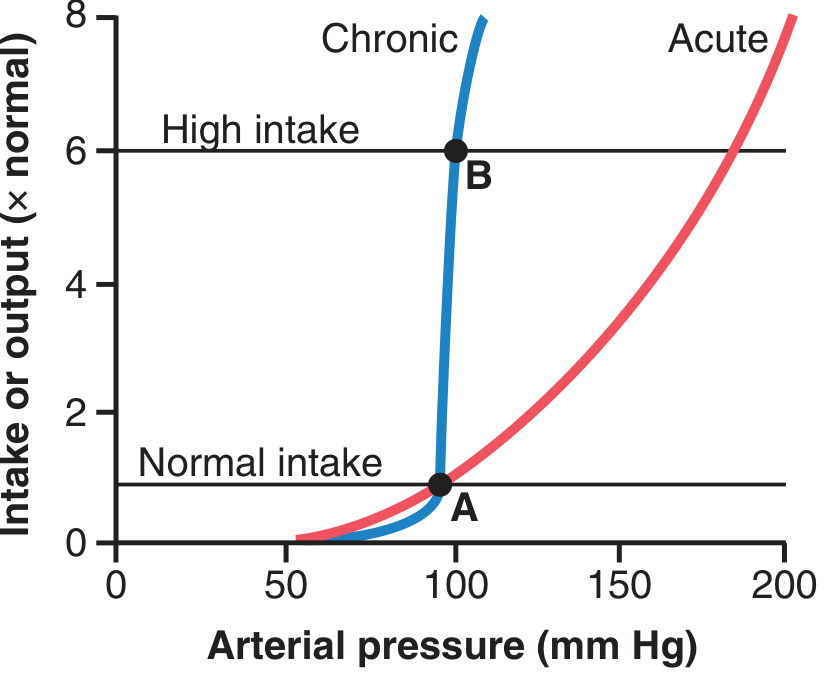
Fig: Chronic renal output curve (blue) is much steeper than the acute curve (red). Points A and B show that even a 6x increase in salt intake causes only a tiny change in equilibrium pressure. (Guyton & Hall)
2. ALDOSTERONE SYSTEM IN LONG-TERM CONTROL
As part of the RAAS, aldosterone provides sustained long-term control:
- Chronic aldosterone excess (as in primary hyperaldosteronism / Conn's syndrome) leads to sustained hypertension
- Destruction of the adrenal cortex (Addison's disease) can lead to severe hypotension
3. ROLE OF THE KIDNEYS - THE SET POINT CONCEPT
In the long term, only the kidneys can set the mean arterial pressure. The concept is:
- The kidney has a specific "renal function curve" - a relationship between arterial pressure and urine output
- Steady-state BP is the pressure at which fluid intake = fluid output (the equilibrium point on the renal function curve)
- Any change that shifts the renal function curve permanently changes the long-term BP set point
Conditions that raise the set point (hypertension):
- Decreased nephron mass (renal artery stenosis, chronic kidney disease)
- Excess aldosterone
- Excess Angiotensin II
- Increased renal sympathetic activity
Conditions that lower the set point (hypotension):
- ANP excess
- ACE inhibition (e.g., captopril)
- Angiotensin receptor blockers
SUMMARY TABLE
| Feature | Short-Term | Intermediate-Term | Long-Term |
|---|---|---|---|
| Onset | Seconds | Minutes to hours | Days to weeks |
| Main mechanism | Baroreceptor reflex, CNS ischemic response, chemoreceptors | RAAS, ADH, ANP | Renal-body fluid, pressure natriuresis |
| Effect on CO | Yes | Indirect (via volume) | Via volume |
| Effect on TPR | Yes (vasoconstriction) | Yes (Ang II) | Minimal direct |
| Effect on blood volume | Minimal | Yes | Primary effect |
| Gain (power) | Moderate | Moderate | Infinite (infinite gain) |
| Adapts/resets? | Yes (baroreceptors reset in 1-2 days) | Partly | No - maintains set point indefinitely |
| Clinical relevance | Hemorrhage, postural changes, exercise | Hypertension, heart failure | Chronic hypertension, CKD |
CLINICAL CORRELATIONS
-
Orthostatic hypotension: Failure of baroreceptor reflex to compensate when a person stands up. BP momentarily drops; if reflex is intact, immediate sympathetic activation restores it within 1-2 seconds.
-
Renal artery stenosis (renovascular hypertension): Stenosis reduces renal perfusion pressure -> kidney "thinks" BP is low -> activates RAAS -> sustained hypertension. Treated with ACE inhibitors (e.g., captopril) or ARBs.
-
Salt-sensitive hypertension: In patients with reduced nephron mass or impaired kidneys, the renal function curve is less steep (resembles the acute curve). Even moderate Na+ intake causes substantial BP increase.
-
Valsalva maneuver: A bedside test of baroreceptor reflex integrity. Straining against a closed glottis raises intrathoracic pressure, reduces venous return, lowers CO and BP -> baroreceptor reflex is activated.
CONCLUSION
Blood pressure regulation is a multi-tiered, redundant system:
- Seconds: Baroreceptor reflex (most important) + chemoreceptor reflex + CNS ischemic response
- Minutes to hours: RAAS + ADH + ANP (hormonal fine-tuning of volume and vascular tone)
- Days to weeks: Renal pressure natriuresis/diuresis (the ultimate, infinite-gain controller)
No single mechanism operates in isolation - they are tightly integrated. However, the kidney is the final arbiter of long-term BP, as it is the only organ capable of permanently altering the body's fluid volume set point.
Sources: Guyton & Hall Textbook of Medical Physiology (Ch. 18 & 19); Costanzo Physiology 7th Edition (Ch. 4)
This topic is present in which chapter of guyton
Based on the content I already retrieved in the previous session from Guyton & Hall, I can answer this directly:
The topic of Short-Term & Long-Term Regulation of Blood Pressure is covered across two chapters in Guyton & Hall Textbook of Medical Physiology:
Chapter 18
"Nervous Regulation of the Circulation and Rapid Control of Arterial Pressure"
Covers all short-term mechanisms:
- Autonomic nervous system anatomy
- Sympathetic vasoconstrictor system
- Vasomotor center in the medulla
- Baroreceptor reflex (carotid sinus + aortic arch)
- Chemoreceptor reflex
- CNS ischemic response (Cushing reflex)
- Stress relaxation
Chapter 19
"Role of the Kidneys in Long-Term Control of Arterial Pressure and in Hypertension: The Integrated System for Arterial Pressure Regulation"
Covers all long-term mechanisms:
- Renal-body fluid system
- Pressure natriuresis and pressure diuresis
- Renin-Angiotensin-Aldosterone System (RAAS)
- Acute vs. chronic renal output curves
- Salt sensitivity and hypertension
Quick tip for your exam: Chapter 18 = short-term (neural), Chapter 19 = long-term (renal/hormonal). These two chapters together form the complete answer to this long question.
This is a shared conversation. Sign in to Orris to start your own chat.