Metabolic response to injury surgery topic explain for my exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple surgical textbooks. Let me compile the full exam-oriented answer.
Metabolic Response to Injury/Surgery
Overview
The metabolic response to injury is a complex, graded, systemic reaction to tissue damage. It was first described by Sir David Cuthbertson in the 1930s using the classic "ebb and flow" model. The more severe the injury, the greater the response - ranging from a modest transient rise in temperature/heart rate after elective surgery, to full-blown SIRS, hypermetabolism, and MODS after major trauma, sepsis, or burns.
Bailey & Love's Short Practice of Surgery, 28th Ed
Phase 1: The Ebb Phase (Shock Phase)
- Onset: immediately after injury, lasting ~12-24 hours
- Characterized by hypometabolism (reduced oxygen consumption)
- Features:
- Hypovolaemia
- Decreased basal metabolic rate (BMR)
- Reduced cardiac output
- Hypothermia
- Lactic acidosis
- Decreased insulin secretion
- Purpose: conserve circulating volume and energy stores
- Dominant hormones: catecholamines, cortisol, aldosterone (via renin-angiotensin activation)
- If the patient is NOT resuscitated, this progresses to death
Pye's Surgical Handicraft, 22nd Ed; Bailey & Love 28th Ed
Phase 2: The Flow Phase (Hypermetabolic/Catabolic Phase)
Following adequate resuscitation, the ebb phase transitions into the flow phase, which corresponds to SIRS (Systemic Inflammatory Response Syndrome).
Features:
- Hypermetabolism (increased BMR)
- Increased cardiac output
- Raised body temperature (pyrexia)
- Leukocytosis
- Increased oxygen consumption
- Tissue oedema (from vasodilation + capillary leakage)
- Increased gluconeogenesis
- Net negative nitrogen balance
Duration varies with injury severity:
- Gastrectomy: ~5 days
- Fractured femur: ~2 weeks
- Major burn: months
- Severe sepsis superimposed on burns: metabolic rate can reach 2x normal
Pye's Surgical Handicraft 22nd Ed; Bailey & Love 28th Ed; Sabiston Textbook of Surgery
Phase 3: The Anabolic Phase
- Occurs after the acute catabolic response resolves
- Characterized by:
- Positive nitrogen balance
- Restoration of fat stores
- Muscle protein synthesis
- Normalization of hormonal milieu
- Recovery of function
Mediators of the Metabolic Response
1. Damage-Associated Molecular Patterns (DAMPs)
When tissue is injured, cells release DAMPs (also called alarmins) - intracellular fragments including:
- Heat shock proteins
- High mobility group protein B1 (HMGB1)
- S100 proteins
- Fragments of nucleic acids
These are sensed by pattern recognition receptors (PRRs) - specifically Toll-like receptors (TLRs) and NOD-like receptors (NLRs) - on innate immune cells (macrophages, neutrophils, dendritic cells).
2. The Inflammasome Cascade
PRR activation triggers formation of inflammasomes (intracellular protein complexes), which activate caspases, which in turn release key cytokines:
- IL-1 (interleukin-1)
- IL-6 (interleukin-6)
- TNF-α (tumour necrosis factor-alpha)
- Interferons, chemokines
This produces a sterile systemic inflammatory cascade - local inflammation first, then SIRS if sufficiently severe.
Bailey & Love 28th Ed
3. Neuroendocrine Response
Nociceptive afferent neurones from the injury site travel via the spinal cord to the hypothalamus and pituitary, triggering:
| Hormone | Source | Effect |
|---|---|---|
| CRF (corticotropin-releasing factor) | Hypothalamus | Stimulates ACTH release |
| ACTH | Anterior pituitary | Stimulates adrenal cortisol |
| Cortisol | Adrenal cortex | Gluconeogenesis, protein catabolism, immunosuppression |
| Adrenaline/noradrenaline | Adrenal medulla + SNS | Glycogenolysis, lipolysis, tachycardia |
| ADH (vasopressin) | Posterior pituitary | Water retention, Na retention |
| Aldosterone | Adrenal cortex | Na and water retention, K loss |
| Glucagon | Pancreas | Gluconeogenesis |
| GH (growth hormone) | Anterior pituitary | Lipolysis, insulin resistance |
Bailey & Love 28th Ed
Secondary triggers that amplify the response:
- Sepsis
- Haemorrhage and massive transfusion
- Acidosis
- Crush syndrome
- Ischaemia-reperfusion injury
Metabolic Changes in Detail
A. Carbohydrate Metabolism
- Hyperglycaemia ("pseudodiabetes" or "diabetes of injury")
- Causes:
- Increased gluconeogenesis (from amino acids, glycerol, lactate)
- Increased glycogenolysis
- Insulin resistance - peripheral tissues cannot take up glucose despite elevated insulin; mediated by proinflammatory cytokines and reduced sensitivity of insulin-regulated glucose transporters (GLUT)
- Relative glucagon excess
- Insulin resistance is proportional to injury severity; can persist ~2 weeks after major abdominal surgery
B. Protein Metabolism
- Net negative nitrogen balance - protein breakdown exceeds synthesis
- Skeletal muscle is broken down to release amino acids via the ubiquitin-proteasome pathway
- Amino acids are redirected to the liver for:
- Gluconeogenesis (glucose production)
- Synthesis of acute-phase proteins (see below)
- Glutamine becomes the preferred fuel for immune cells (used to synthesize the antioxidant glutathione)
- Urinary nitrogen losses increase - monitored by 24-hour urine urea
Muscle wasting consequences: immobility, poor wound healing, hypostatic pneumonia, prolonged recovery, increased mortality if severe.
C. Fat Metabolism
- Lipolysis is activated by catecholamines, cortisol, and glucagon
- Free fatty acids (FFAs) and glycerol are released from adipose tissue
- FFAs are oxidized for energy
- Fat stores fuel the hypermetabolic state
- If the patient cannot eat, they "waste away" - fat then lean mass is depleted
D. Fluid and Electrolyte Changes
- Na and water retention (via ADH and aldosterone)
- Potassium loss (urinary)
- Oedema - from increased capillary permeability (leaky capillaries secondary to DAMPs activating endothelial cells and platelets)
- Reduced urine output initially
Pye's Surgical Handicraft, 22nd Ed
The Acute-Phase Protein Response (Liver)
Under the influence of IL-1, IL-6, and TNF-α, the liver reprioritizes protein synthesis:
| Type | Examples | Change |
|---|---|---|
| Positive acute-phase reactants | CRP, fibrinogen, complement, alpha-1 antitrypsin, ferritin | Plasma level increases |
| Negative acute-phase reactants | Albumin, transferrin, pre-albumin | Plasma level falls |
- The fall in albumin is mainly due to increased transcapillary escape (increased microvascular permeability) rather than reduced hepatic synthesis
- Albumin transcapillary escape rate can triple after major injury/sepsis
Bailey & Love 28th Ed
SIRS, CARS, and PICS
After the initial inflammatory phase, the body launches a counter-regulatory response:
- SIRS (Systemic Inflammatory Response Syndrome) - the initial proinflammatory response
- CARS (Compensatory Anti-inflammatory Response Syndrome) - the counter-regulatory immunosuppressive phase; increases susceptibility to nosocomial (opportunistic) infection
- PICS (Persistent Inflammation, Immunosuppression, and Catabolism Syndrome) - affects 30-50% of ICU patients with prolonged organ dysfunction; does NOT respond well to nutritional interventions
Bailey & Love 28th Ed; Sabiston Textbook of Surgery
Magnitude of the Response (Graded)
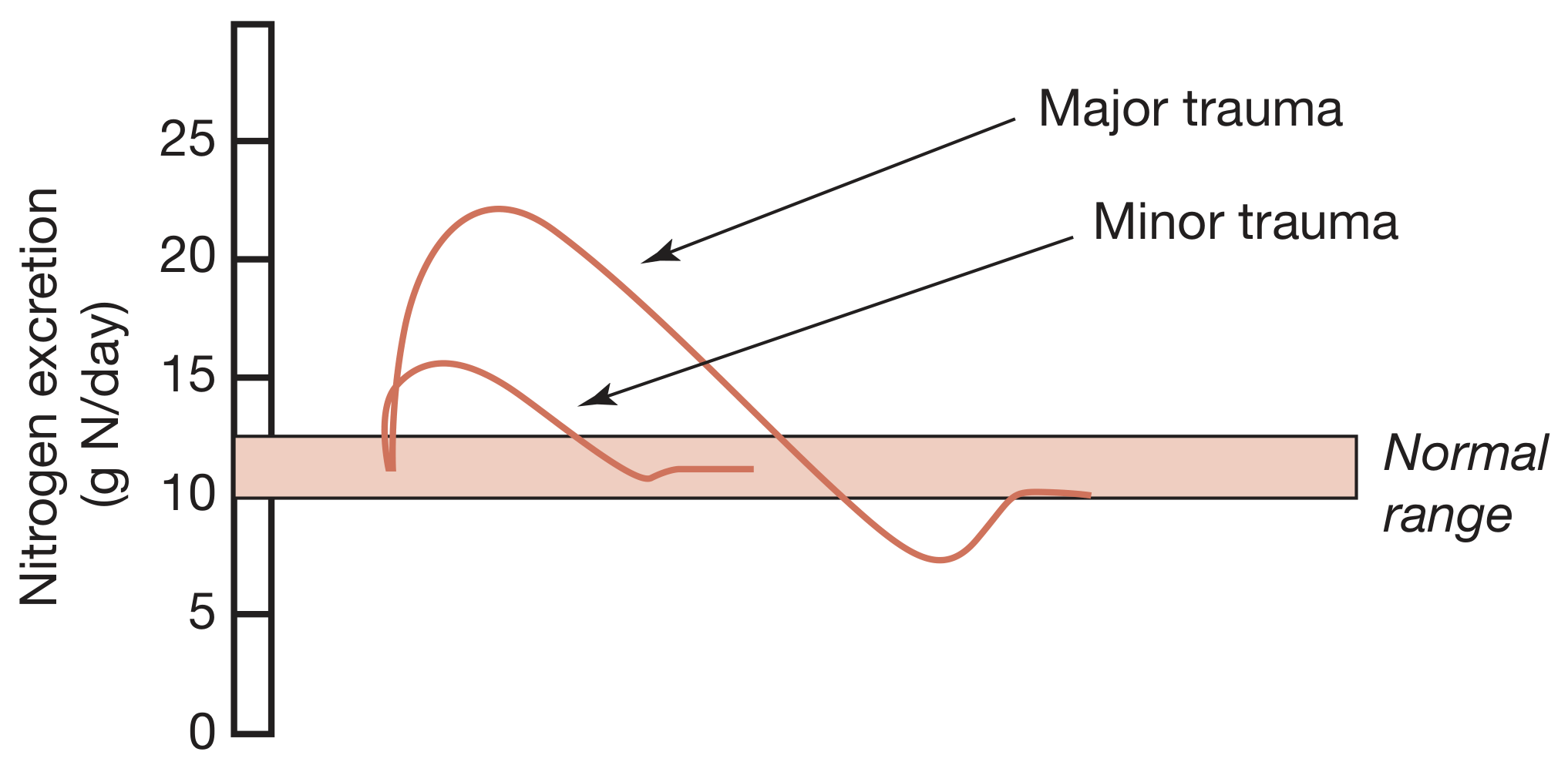
Figure: Hypermetabolism and increased nitrogen excretion are closely related to the magnitude of the initial injury and show a graded response. (Bailey & Love 28th Ed)
Overfeeding - A Clinical Pitfall
Excessive carbohydrate administration causes:
- Carbohydrates to be stored as fat in the liver (hepatomegaly)
- High CO2 production - for every 3 O2 molecules inspired, 29 CO2 molecules must be expired (increased respiratory quotient)
- Respiratory acidosis from inability to eliminate CO2 (hyperventilation, then failure)
- Particularly dangerous with IV nutrition
Pye's Surgical Handicraft, 22nd Ed
Modulating the Response (Clinical Relevance)
| Intervention | Effect |
|---|---|
| Adequate resuscitation | Limits ebb phase, reduces secondary DAMPs |
| Early enteral nutrition | Preferred over parenteral; early feeding reduces catabolism |
| Regional/neuraxial anaesthesia | Blunts neuroendocrine limb |
| Minimally invasive surgery | Reduces magnitude of response |
| Enhanced Recovery After Surgery (ERAS) protocols | Reduces surgical stress ("stress-free" perioperative care) |
| Beta-blockade | Shown benefit mainly in severe burn patients |
| TNF-α/IL-1/IL-6 blockade | Has NOT improved outcomes in ICU clinical trials |
Sabiston Textbook of Surgery; Bailey & Love 28th Ed
Key Summary for Exam
| Feature | Ebb Phase | Flow Phase | Anabolic Phase |
|---|---|---|---|
| Timing | Immediate (0-12h) | Hours-days/weeks | Weeks-months |
| Metabolism | Hypometabolic | Hypermetabolic | Anabolic |
| BMR | Decreased | Increased | Normal/increasing |
| Temperature | Decreased | Increased | Normal |
| Cardiac output | Decreased | Increased | Normal |
| Insulin | Decreased | Resistance | Normal |
| Blood glucose | Decreased/normal | High (hyperglycaemia) | Normal |
| Nitrogen balance | Negative | Strongly negative | Positive |
| Key hormones | Catecholamines, cortisol | Cortisol, catecholamines, glucagon | GH, IGF-1 |
| Main purpose | Survival/conservation | Mobilize energy for repair | Rebuild |
Key exam buzzwords: Cuthbertson's ebb and flow, DAMPs, PRRs, inflammasome, IL-6, TNF-α, insulin resistance, pseudodiabetes of injury, ubiquitin-proteasome pathway, acute-phase proteins (CRP up, albumin down), SIRS, CARS, PICS, negative nitrogen balance, gluconeogenesis, lipolysis.
Sources: Bailey & Love's Short Practice of Surgery 28th Ed; Pye's Surgical Handicraft 22nd Ed; Sabiston Textbook of Surgery; Schwartz's Principles of Surgery 11th Ed
Surgical site of injection in detailed for surgery topic exam
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have everything needed for a comprehensive exam answer. Here it is:
Surgical Site Infection (SSI) - Complete Exam Guide
Definition
SSI is an infection that occurs at or near a surgical incision within 30 days of an operative procedure (or within 1 year if an implant is placed and the infection appears related to the procedure). It is defined and classified by the CDC/NHSN (National Healthcare Safety Network).
SSIs account for approximately 20% of all healthcare-associated infections and are the most common and costly complication of surgery.
Mulholland & Greenfield's Surgery 7th Ed; Fischer's Mastery of Surgery 8th Ed
CDC Classification of SSI (3 Types)
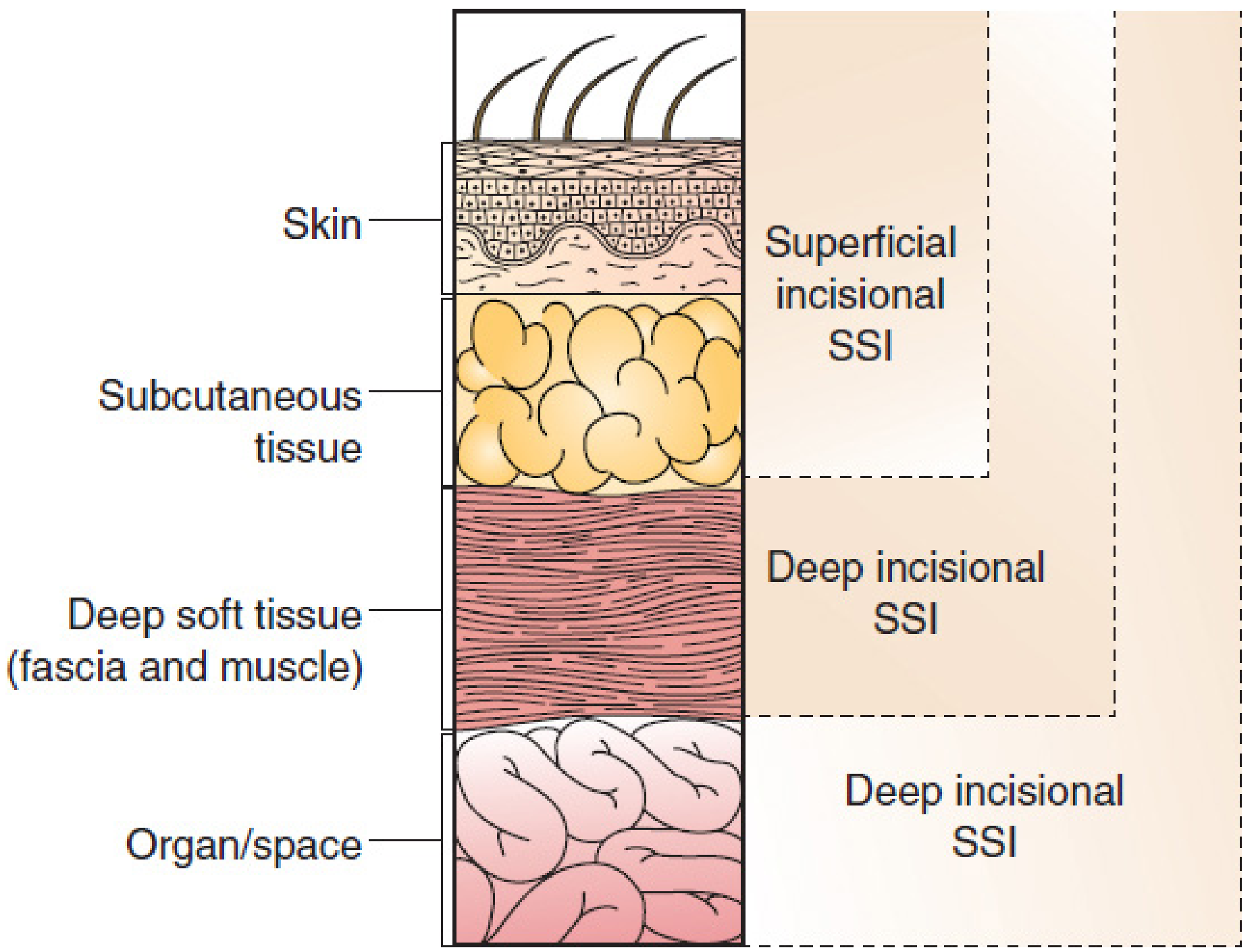
1. Superficial Incisional SSI
- Involves: skin and subcutaneous tissue only
- Timing: within 30 days of surgery
- Diagnosis requires at least one of:
- a. Purulent drainage from the superficial incision
- b. Organisms isolated from aseptically obtained culture of fluid/tissue
- c. Signs/symptoms (pain, tenderness, localized swelling, redness, heat) AND deliberate opening by surgeon, with positive/not cultured wound
- d. Diagnosis by the surgeon or attending physician
- Excluded: cellulitis, stitch abscess/granuloma, stab incision infection
- Most common type (e.g., most hernia repairs)
2. Deep Incisional SSI
- Involves: deep soft tissues - fascia and muscle layers
- Timing: within 30 days (no implant) OR within 1 year (with implant in place)
- Diagnosis requires at least one of:
- a. Purulent drainage from deep incision (not from organ/space)
- b. Spontaneous or deliberate wound dehiscence + fever (>38°C) or localized pain/tenderness
- c. Abscess or evidence of infection found on direct examination, reoperation, histopathology or radiology
- d. Diagnosis by surgeon or attending physician
3. Organ/Space SSI
- Involves: any part of the body opened or manipulated during surgery, excluding the incision/fascia/muscle
- Examples: intra-abdominal abscess, thoracic empyema, mediastinitis, osteomyelitis
- Diagnosis requires:
- Purulent drainage from organ/space drain
- Organisms isolated from aseptically obtained culture from organ/space
- Abscess/evidence on direct examination, reoperation, histopathology, or radiology
- Diagnosis by surgeon or attending physician
Mulholland & Greenfield's Surgery 7th Ed; Fischer's Mastery of Surgery 8th Ed
Wound Classification (CDC/NHSN - 4 Classes)
This is a key exam table - SSI risk correlates directly with wound class:
| Class | Definition | Expected SSI Rate |
|---|---|---|
| Clean (Class I) | Uninfected wound, no inflammation, no entry into respiratory/GI/GU/biliary tract. Closed primarily, drained with closed drainage if needed. | 1-5% |
| Clean-Contaminated (Class II) | Controlled entry into respiratory, alimentary, genital, or urinary tract without unusual contamination. Includes biliary tract, appendix, vagina, oropharynx with no evidence of infection. | 3-11% |
| Contaminated (Class III) | Fresh open accidental wounds; break in sterile technique; leakage from GI tract; acute non-purulent inflammation (including necrotic tissue without purulent drainage). | 10-17% |
| Dirty/Infected (Class IV) | Old traumatic wounds with devitalized tissue; existing clinical infection; perforated viscera. Organisms present in operative field before surgery. | >27% |
Key fact: 70-95% of all SSIs are caused by the patient's own endogenous flora.
Fischer's Mastery of Surgery 8th Ed; Sabiston Textbook of Surgery; Mulholland & Greenfield's Surgery 7th Ed
Risk Factors for SSI
A. Patient-Related (Intrinsic) Risk Factors
| Risk Factor | Mechanism |
|---|---|
| Diabetes mellitus | Hyperglycaemia impairs neutrophil function and wound healing |
| Obesity | Poor vascularity of fat, technical difficulty, increased dead space |
| Malnutrition | Impaired anabolism, immune dysfunction, poor wound healing |
| Smoking | Vasoconstriction, tissue hypoxia, impaired collagen synthesis |
| Immunosuppression (steroids, chemotherapy, HIV) | Impaired immune response |
| Staphylococcal nasal colonization | ~1/3 of population colonized; S. aureus is #1 cause of SSI |
| ASA score 3, 4, or 5 | Captures comorbidity burden |
| Anaemia | Tissue hypoxia |
| Blood transfusion | Immunomodulatory effect |
| Age extremes | Reduced immune competence |
| Previous irradiation | Poor tissue vascularity |
B. Procedure-Related (Extrinsic) Risk Factors
| Risk Factor | Notes |
|---|---|
| Wound classification | Higher class = higher risk (see above) |
| Operative duration >75th percentile for that procedure | Reflects difficulty + increased contamination exposure time |
| Emergency vs. elective surgery | Emergency surgery has higher SSI rates |
| Inappropriate antibiotic prophylaxis | Wrong timing, wrong drug, or too long |
| Hair shaving (vs. clipping) | Shaving increases SSI vs. clipping |
| Hypothermia | Impairs neutrophil function, vasoconstriction |
| Hyperglycaemia perioperatively | Even in non-diabetics |
| Blood loss/transfusion | Immunosuppressive |
| Inadequate skin preparation | Insufficient antisepsis |
C. NHSN/NNIS Risk Index
Three independent risk factors form the SSI Risk Index (0-3 points):
- ASA score of 3, 4, or 5
- Wound class contaminated (III) or dirty/infected (IV)
- Operative duration >75th percentile cut-point for that procedure
- Laparoscopic approach: modified index - scored as 1 (lower SSI risk than open)
- The patient's SSI risk category = number of these factors present
Microbiology of SSI
| Wound Type | Common Organisms |
|---|---|
| Clean wounds (skin only violated) | Gram-positive: S. aureus, coagulase-negative Staphylococcus |
| Clean-contaminated (GI, biliary) | Gram-negative enteric organisms + anaerobes (E. coli, Bacteroides, Klebsiella) |
| Contaminated/Dirty | Polymicrobial: gram-positives + gram-negatives + anaerobes |
| Implant-related | Coagulase-negative Staphylococcus, MRSA |
Trend: S. aureus has grown from 22.5% (1986-2003) to 30% (2006-2007) of SSI isolates. MRSA now comprises ~49% of all S. aureus SSI isolates and is the leading cause in vascular surgery.
Mulholland & Greenfield's Surgery 7th Ed
Prevention of SSI
1. Antibiotic Prophylaxis (Most Important)
- Timing: within 30-60 minutes before incision (give within 1 hour for most antibiotics; within 2 hours for fluoroquinolones and vancomycin)
- SIP-1: IV prophylaxis initiated within 1 hour before incision
- SIP-2: Antibiotic selection consistent with published guidelines
- SIP-3: Discontinue prophylaxis within 24 hours after surgery (48h for cardiac surgery)
- Redose for long procedures (e.g., re-dose cefazolin every 4 hours for operations >4 hours)
- Giving antibiotics too early (>2 hours) or too late (after incision) both increase SSI risk
Common agents:
- Clean surgery: Cefazolin (gram-positive coverage)
- Colorectal surgery: Cefazolin + Metronidazole OR oral neomycin + erythromycin base
- MRSA colonization/allergy: Vancomycin
2. Skin Preparation
- Chlorhexidine-alcohol preferred over povidone-iodine for skin antisepsis
- Adequate time for drying/contact
3. Hair Removal
- Clip (do not shave) - shaving creates micro-lacerations and increases SSI
- Remove only if necessary and only immediately before surgery
4. Normothermia
- Maintain intraoperative temperature >36°C; hypothermia impairs neutrophil oxidative killing
5. Glycaemic Control
- Target blood glucose <200 mg/dL intraoperatively and postoperatively
- Hyperglycaemia impairs neutrophil function even in non-diabetics
6. Supplemental Oxygen
- 80% FiO2 intraoperatively may reduce SSI (enhances oxidative killing by neutrophils)
7. Surgical Technique
- Minimize dead space
- Avoid excessive electrocautery
- Use closed-suction drains where indicated
- Wound protectors (especially in colorectal surgery)
- Aseptic technique, minimize operative time
8. MRSA Decolonization (Pre-op Screening)
- Screen high-risk patients (orthopedic, cardiac)
- Mupirocin nasal ointment + chlorhexidine skin wash if MRSA carrier
- MRSA Bundle: PCR nasal screening, contact isolation, hand hygiene, cultural transformation, monitoring
9. Bowel Preparation
- Mechanical bowel prep + oral antibiotics reduces SSI for colorectal surgery
Mulholland & Greenfield's Surgery 7th Ed; Sabiston Textbook of Surgery
Treatment of SSI
Superficial/Deep Incisional SSI:
- Open the wound - drain pus, debride necrotic tissue
- Culture - Gram stain + cultures (essential in era of resistant organisms)
- Empiric antibiotics - start early, cover likely organisms
- De-escalate - tailor antibiotics once culture sensitivities available
- Wound care - dressing changes, secondary closure or healing by secondary intention
Organ/Space SSI:
- Source control is the priority:
- Percutaneous drainage (interventional radiology) for intra-abdominal abscess
- Open surgical drainage if required
- Culture abscess fluid
- Empiric antibiotics, de-escalate with sensitivities
Surveillance Time Periods (Key Exam Fact)
| SSI Type | No Implant | With Implant |
|---|---|---|
| Superficial incisional | 30 days | 30 days only |
| Deep incisional | 30 days | 1 year |
| Organ/space | 30 days | 1 year |
Key Exam Summary Box
| Topic | High-Yield Point |
|---|---|
| Most common SSI type | Superficial incisional |
| Most common causative organism | S. aureus (MRSA increasingly) |
| Highest-risk wound class | Dirty/infected (>27% SSI rate) |
| SSI risk index components | ASA ≥3 + contaminated/dirty wound + prolonged operation |
| Antibiotic timing | 30-60 min before incision (within 1 hr) |
| Stop antibiotics by | 24 hours post-op |
| Avoid hair shaving | Clip instead |
| Deepest SSI type | Organ/space |
| Implant SSI surveillance window | 1 year |
| 70-95% SSIs caused by | Patient's own endogenous flora |
Sources: Mulholland & Greenfield's Surgery 7th Ed; Fischer's Mastery of Surgery 8th Ed; Sabiston Textbook of Surgery; Katzung's Basic & Clinical Pharmacology 16th Ed
Create a PPT summary on SSI prevention bundles for SCIP compliance
Reading File
Reading File
Reading File
Finding Sources
Running Command
Running Command
Writing File
Running Command
Running Command
Your presentation is ready!
SSI Prevention Bundles SCIP
Presentation · PPTX
What's Inside (12 Slides)
The deck uses a deep navy + teal + amber palette - dark backgrounds for key slides, card-based layouts, color-coded sections, and accent bars throughout.
| Slide | Content |
|---|---|
| 1 - Title | SSI Prevention Bundles / SCIP Compliance cover |
| 2 - What is SSI? | CDC definition + 3 SSI types (Superficial / Deep / Organ-Space) |
| 3 - Wound Classification | 4-class CDC/NHSN table with SSI rate badges per class |
| 4 - SCIP Overview | What SCIP is, SIP-1/SIP-2/SIP-3 performance measures |
| 5 - Preoperative Bundle | Antibiotic prophylaxis, hair removal, skin prep, MRSA decolonization, nutrition |
| 6 - Intraoperative Bundle | Normothermia, glycaemic control, supplemental O₂, aseptic technique, wound protectors, OR environment |
| 7 - Postoperative Bundle | Antibiotic discontinuation, wound care, glucose control, nutrition, surveillance, SSI treatment |
| 8 - Risk Index | NHSN Risk Index (0-3 points) + patient & procedure risk factors |
| 9 - Antibiotic Guide | Procedure-by-procedure antibiotic selection table |
| 10 - MRSA Bundle | 5-component MRSA bundle + outcome data |
| 11 - ERAS & Compliance | ERAS integration + SCIP compliance monitoring metrics |
| 12 - Key Takeaways | 6-point visual summary of the entire bundle |
This is a shared conversation. Sign in to Orris to start your own chat.