Bile duct
Reading File
Asking for Preferences
Finding Sources
Searching Images
bile duct anatomy diagram
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of bile duct anatomy and physiology, drawn from authoritative surgical and histology textbooks.
Bile Duct — Anatomy & Physiology
Overview
The bile duct system (biliary tree) conducts bile from the liver to the duodenum. It is divided into intrahepatic and extrahepatic portions. The extrahepatic biliary system comprises the hepatic ducts, cystic duct, common bile duct, ampulla of Vater, and sphincter of Oddi.
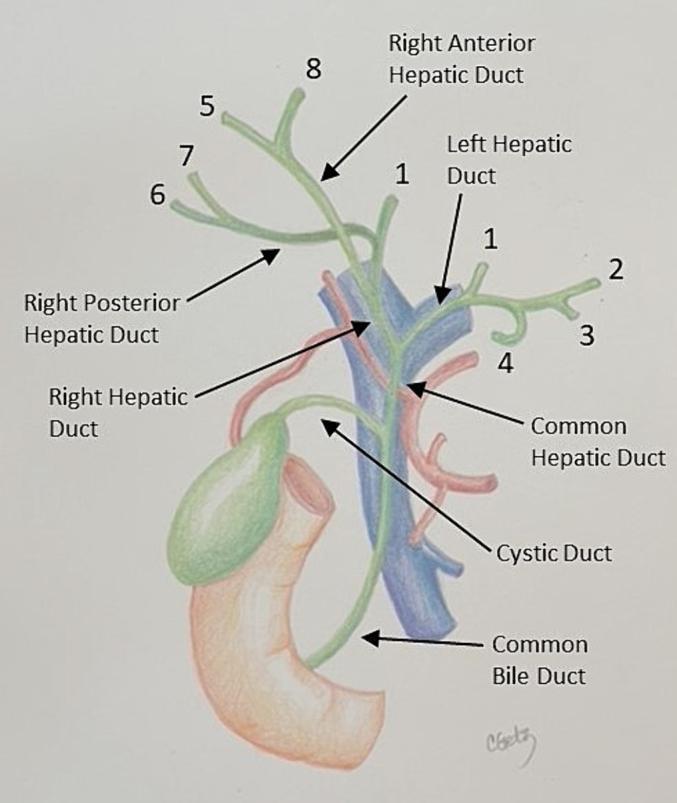
1. Hepatic Ducts
The right hepatic duct is formed by the union of the right anterior and right posterior sectoral ducts. This occurs in ~60–65% of individuals; in ~12%, the right anterior and posterior branches converge directly at the confluence (trifurcation). In ~20% of cases, the right anterior duct joins the common hepatic duct separately.
The left hepatic duct drains segments 1–4 and is typically longer and more superficial than the right.
The common hepatic duct (CHD) is formed by the union of the right and left hepatic ducts — in 95% of people this union occurs outside the liver, just below the porta hepatis; in 5% it occurs within the liver substance. The CHD lies anterior to the portal vein and to the right of the hepatic artery within the hepatoduodenal ligament. Its length ranges from 2 to 6.5 cm. An accessory right hepatic duct is present in ~10% of individuals.
The confluence of the right and left hepatic ducts lies anterior to the portal venous bifurcation, typically overlying the origin of the right portal vein branch.
— Yamada's Textbook of Gastroenterology, 7th ed.
2. Triangle of Calot
Described in 1891, the triangle of Calot is bounded:
- Superiorly — hilum of the liver
- Right — cystic duct
- Left — common hepatic duct
Critical structures passing through it include the right hepatic artery, cystic artery, 90% of accessory hepatic ducts, and 95% of aberrant right hepatic arteries. Careful dissection here is essential to avoid iatrogenic injury during cholecystectomy.
3. Cystic Duct
The cystic duct arises from the neck of the gallbladder. Its lumen is typically 1–3 mm (occasionally up to 10 mm). In 70% of individuals it joins the common hepatic duct directly; however, its insertion can vary widely — from the right hepatic duct to the level of the ampulla — and its length ranges from 0.5 to 8 cm.
Within the cystic duct, the mucosa forms 5–10 spiral (crescent-shaped) folds — the spiral valves of Heister — which prevent excessive distension or collapse with pressure changes and impede stone passage into the common bile duct. The cystic duct lacks a true sphincter; it functions mainly as a passive conduit.
— Yamada's Textbook of Gastroenterology, 7th ed.; Histology: A Text and Atlas
4. Common Bile Duct (CBD)
Formed by the union of the cystic duct and common hepatic duct. Key measurements:
- Length: ~7.5 cm
- Diameter: mean ~6 mm (dilates with distal obstruction)
The CBD has four segments:
| Segment | Length | Relations |
|---|---|---|
| Supraduodenal | ~2.5 cm | Right border of hepatoduodenal ligament; anterior to portal vein, right of hepatic artery |
| Retroduodenal | 2.5–4 cm | Posterior to first part of duodenum; runs left toward gastroduodenal artery |
| Pancreatic | variable | Retropancreatic or within pancreatic head; obstructed early in pancreatic head cancer |
| Intraduodenal | ~2 cm | Traverses duodenal wall obliquely with pancreatic duct; opens at major papilla (ampulla of Vater), 7–10 cm from pylorus |
In 29% of cases, a septum persists between the bile duct and pancreatic duct, forming separate ostia on the papilla rather than a shared ampulla.
— Yamada's Textbook of Gastroenterology, 7th ed.
5. Ampulla of Vater & Sphincter of Oddi
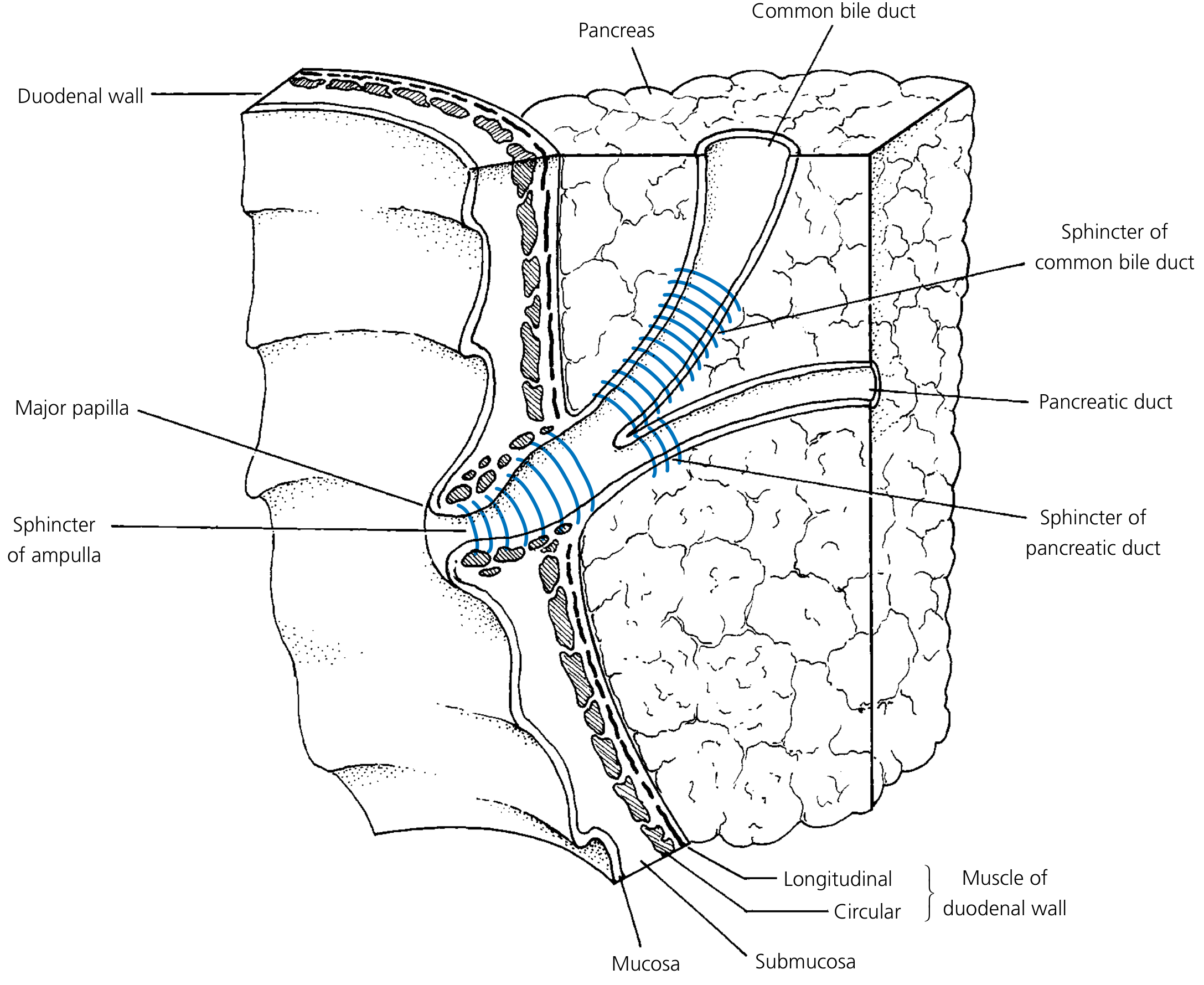
The ampulla of Vater is formed where the CBD joins the main pancreatic duct. It is present as a channel >2 mm in 46% of people, <2 mm in 32%, and absent (no junction) in 29%.
The sphincter of Oddi is the collective term for smooth muscle surrounding the intraduodenal segment:
- Sphincter choledochus (of Boyden) — surrounds the preampullary CBD; the primary regulator of bile flow
- Sphincter pancreaticus — surrounds the distal pancreatic duct (when present)
- Sphincter of the ampulla — surrounds the common channel
The CBD narrows significantly as it passes through the duodenal wall; these narrowings are the commonest sites for gallstones to impact and for injury during common duct exploration.
6. Blood Supply
The blood supply to the extrahepatic bile ducts is segmental:
- Hepatic ducts + supraduodenal CBD — branches of the cystic artery
- Retroduodenal CBD — retroduodenal and posterior superior pancreaticoduodenal arteries
- Pancreatic + intraduodenal CBD — anterior and posterior superior pancreaticoduodenal arteries
Because of this segmental pattern, extensive mobilization of the CBD risks ischemic injury and postoperative stricture.
7. Venous & Lymphatic Drainage
- Veins from the hepatic ducts and proximal CBD drain directly into the liver
- Veins from the lower CBD drain into the portal vein
- Lymphatics from the upper biliary tree flow to porta hepatis nodes, then to celiac lymph nodes
- Some drainage from the inferior CBD reaches deep pancreatic nodes near the superior mesenteric artery origin
8. Histology
The mucosa of the extrahepatic bile ducts is lined with tall columnar epithelium containing mucous glands, surrounded by connective tissue. Smooth muscle in the hepatic ducts and proximal CBD is sparse and discontinuous (arranged longitudinally or circularly). Muscle becomes progressively more substantial approaching the duodenum, culminating in the distinct sphincter of Oddi complex.
The common hepatic duct is approximately 3 cm long and lacks a muscularis mucosae (unlike the rest of the alimentary canal).
— Histology: A Text and Atlas, 8th ed.
9. Physiology: Bile Flow
The liver secretes ~1 L of bile per day. Bile flow is regulated by:
| Stimulus | Effect |
|---|---|
| CCK, gastrin, motilin (released during digestion) | Increase bile flow; gallbladder contraction |
| Parasympathetic stimulation | Gallbladder contraction + sphincter of Oddi relaxation |
| Estrogen (e.g., in pregnancy) | Decreases bile secretion |
| Portal blood bile salt concentration | Regulates hepatocyte bile salt synthesis |
Bile functions:
- Emulsification and absorption of dietary fat
- Vehicle for hepatic excretion of cholesterol, bilirubin, iron, and copper
Enterohepatic circulation: ~90% of bile salts are reabsorbed by the terminal ileum and returned to the liver via portal blood, where they are re-secreted. Cholesterol, phospholipid lecithin, most electrolytes, and water are similarly recycled. Bilirubin glucuronide is not recycled — it is excreted in feces (giving them their color); failure of conjugation or secretion produces jaundice.
— Histology: A Text and Atlas, 8th ed.; Yamada's Textbook of Gastroenterology, 7th ed.
This is a shared conversation. Sign in to Orris to start your own chat.