Usg doppler bilateral lower limb interpretation in very detail
Reading File
Finding Sources
Finding Sources
Searching Images
USG Doppler bilateral lower limb arterial venous waveform interpretation
Finding Sources
Finding Sources
Loading Image
Reading File
Searching Images
peripheral arterial disease PAD ankle brachial index ABI Doppler waveform triphasic biphasic monophasic
Loading Image
Loading Image
Searching Images
DVT deep vein thrombosis compression ultrasound non-compressible vein thrombus
Loading Image
Loading Image
Here is a comprehensive guide to USG Doppler Bilateral Lower Limb Interpretation, covering both arterial and venous systems in detail.
USG Doppler Bilateral Lower Limb — Detailed Interpretation Guide
PART 1: TECHNICAL BASICS
Modes Used
| Mode | Purpose |
|---|---|
| B-mode (Greyscale) | Vessel wall, lumen, compressibility, thrombus echogenicity |
| Color Doppler | Flow direction, patency, turbulence |
| Power Doppler | Sensitive low-flow detection (no directional info) |
| Spectral (Pulsed Wave) Doppler | Waveform analysis, velocity measurements |
| Continuous Wave Doppler | High-velocity stenosis (less commonly used) |
Patient Positioning
- Arterial study: Supine; leg slightly externally rotated. Popliteal artery: prone or lateral decubitus
- Venous study: Supine with legs slightly dependent (Trendelenburg reversed) to distend veins; or sitting upright for calf veins
Transducer Selection
- Linear high-frequency (7–15 MHz): Superficial femoral, popliteal, tibial vessels, veins
- Curvilinear (3–5 MHz): Aortoiliac segment, obese patients
PART 2: ARTERIAL DOPPLER — BILATERAL LOWER LIMB
2.1 Vessels Examined (Proximal → Distal)
| Segment | Vessels |
|---|---|
| Aortoiliac | Distal aorta, common iliac artery |
| Thigh | Common femoral artery (CFA), profunda femoris, superficial femoral artery (SFA) |
| Knee | Popliteal artery |
| Leg | Anterior tibial artery (ATA), posterior tibial artery (PTA), peroneal artery |
| Foot | Dorsalis pedis artery (DPA) |
2.2 Normal Arterial Waveform — Triphasic Pattern
A normal peripheral artery at rest has a triphasic (high-resistance) waveform with three distinct components:
- Phase 1 — Forward systolic peak: Rapid high-amplitude upstroke during ventricular systole
- Phase 2 — Brief reverse diastolic flow: Due to peripheral arterial elasticity and vasoconstriction (a small below-baseline deflection)
- Phase 3 — Forward low-velocity late diastolic flow: Elastic recoil of arterial wall propels a small second forward wave
Biphasic waveform: Loss of phase 3 — still normal in elderly or during exercise/warmth (vasodilation)
Monophasic waveform: Loss of phases 2 and 3 — indicates proximal stenosis or obstruction (parvus-tardus pattern)
2.3 Arterial Waveform Changes with Disease
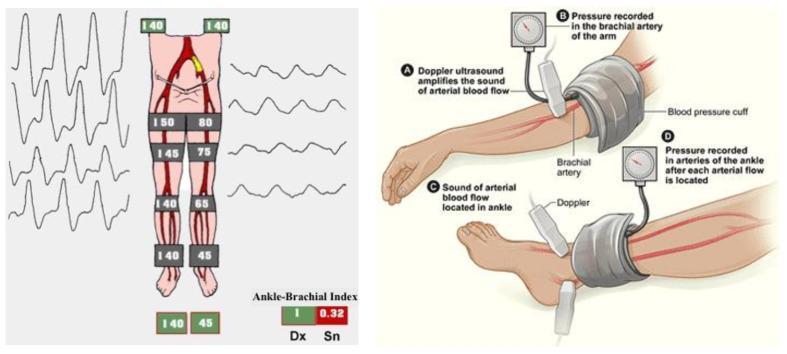
Left: Normal triphasic waveforms with equal bilateral pressures (ABI ~1.0) vs stenotic side with progressively dropping segmental pressures and flattened monophasic waveforms (ABI 0.32). Right: ABI measurement technique using Doppler probe and cuff.
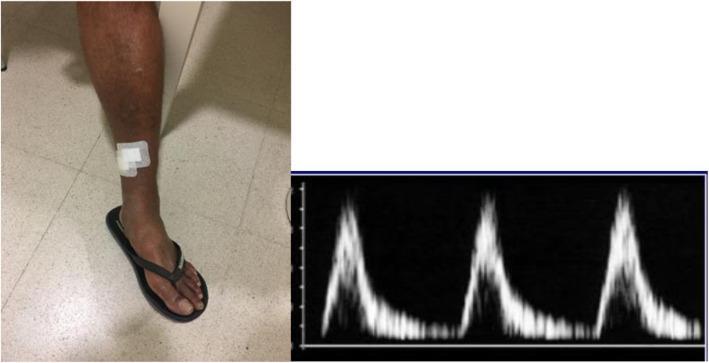
Clinical ischemic ulcer (left) with corresponding Doppler showing loss of triphasic pattern — delayed systolic upstroke and monophasic flow indicating suprapopliteal stenosis.
| Waveform | Appearance | Significance |
|---|---|---|
| Triphasic | 3 peaks; reverse diastolic component present | Normal high-resistance peripheral artery |
| Biphasic | 2 peaks; reverse component absent | Elderly, vasodilated, or mild disease |
| Monophasic | Single broad peak; no reverse flow | Significant proximal stenosis/occlusion |
| Parvus-tardus | Low amplitude + slow systolic rise time | Classic for proximal stenosis (e.g., iliac occlusion) |
| Spectral broadening | Waveform fills below baseline curve | Turbulent flow at or distal to stenosis |
2.4 Velocity Criteria for Stenosis
| Finding | Significance |
|---|---|
| Peak systolic velocity (PSV) ratio >2:1 (stenotic:prestenotic) | ≥50% diameter stenosis |
| PSV ratio >4:1 | ≥75% stenosis |
| PSV at stenosis >200 cm/s with ratio >2 | Hemodynamically significant stenosis |
| No detectable flow on Color + Spectral Doppler | Occlusion |
| Collateral waveforms (low-velocity, monophasic) | Chronic occlusion with collateral formation |
2.5 Ankle-Brachial Index (ABI)
Measured with a continuous-wave Doppler probe and blood pressure cuff:
ABI = Ankle systolic pressure ÷ Brachial systolic pressure
Use the higher of posterior tibial and dorsalis pedis pressures at each ankle; use higher arm pressure for denominator.
| ABI | Interpretation |
|---|---|
| >1.3 | Non-compressible vessels (medial calcification — diabetes, CKD); unreliable |
| 1.0–1.3 | Normal |
| 0.9–1.0 | Borderline |
| 0.7–0.9 | Mild PAD |
| 0.4–0.7 | Moderate PAD (claudication) |
| <0.4 | Severe PAD / critical limb ischemia |
2.6 Specific Arterial Pathologies
Peripheral Arterial Disease (PAD)
- Plaque: hyperechoic/heterechoic wall thickening on B-mode
- Post-stenotic turbulence: color aliasing, spectral broadening
- Occlusion: absent color fill + no Doppler signal; collaterals visible
- Bilateral comparison is key — asymmetric PSV ratio or waveform change indicates disease
Popliteal Artery Aneurysm
- Focal dilatation >8 mm (or 1.5× diameter of adjacent segment)
- May contain mural thrombus; risk of distal embolization
Aortoiliac Occlusion (Leriche Syndrome)
- Bilateral monophasic/absent CFA signals
- Bilateral thigh claudication + impotence
PART 3: VENOUS DOPPLER — BILATERAL LOWER LIMB
3.1 Vessels Examined
| Segment | Veins |
|---|---|
| Groin | Common femoral vein (CFV), great saphenous vein (GSV) junction |
| Thigh | Femoral vein (FV), profunda femoris vein |
| Popliteal fossa | Popliteal vein (PopV), small saphenous vein (SSV) junction |
| Leg | Posterior tibial veins (PTVs), peroneal veins, anterior tibial veins, gastrocnemius/soleal veins |
3.2 Normal Venous Criteria — "SCAPR" Mnemonic
| Feature | Normal Finding |
|---|---|
| S — Spontaneous flow | Flow present without augmentation in proximal veins (femoral, popliteal) |
| C — Compressibility | Vein collapses completely with gentle transducer pressure |
| A — Augmentation | Flow increases with distal limb compression or Valsalva release |
| P — Phasicity | Flow varies with respiration (increases with expiration in legs) |
| R — Reflux absent | No retrograde flow >0.5 s on augmentation/Valsalva |
3.3 Normal Venous Spectral Waveform
- Spontaneous, phasic (respiratory phasicity): Flow decreases/stops with inspiration (when intra-abdominal pressure rises) and increases with expiration
- Low-velocity, continuous or gently undulating
- Augments briskly with distal compression (calf squeeze)
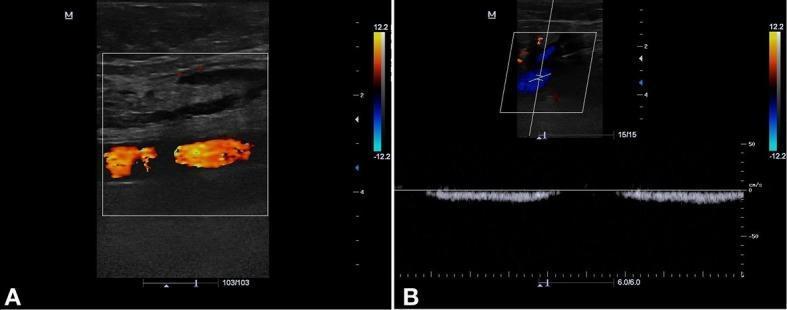
Panel A: Normal superficial femoral artery (orange/red color flow). Panel B: Normal common femoral vein (CFV) with color Doppler blue signal + spectral waveform showing phasic respiratory variation — classic normal venous flow pattern.
3.4 Deep Vein Thrombosis (DVT) — Key Findings
Primary Sign
Non-compressibility — the most specific and sensitive criterion:
- Normal vein completely collapses when compressed
- Thrombosed vein fails to collapse
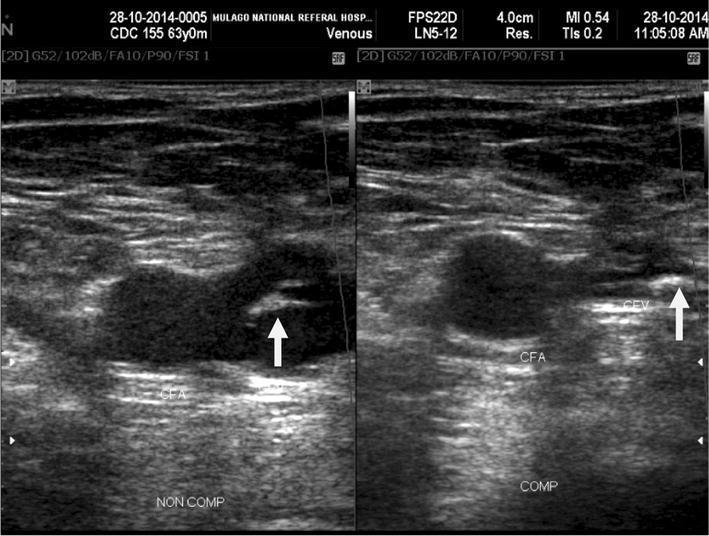
Left (NON COMP): Common femoral vein (CFV) with arrow pointing to echogenic intraluminal thrombus, adjacent to common femoral artery (CFA). Right (COMP): Vein remains non-compressible — confirming acute/chronic DVT. CFA, as expected, is non-compressible regardless.
Secondary Signs
| Sign | Finding |
|---|---|
| Intraluminal echoes | Echogenic material within vein lumen |
| Vein distension | Thrombus expands lumen compared to artery |
| Absent color flow | No color fill within thrombosed segment |
| Absent/reduced phasicity | Loss of respiratory variation |
| Absent augmentation | No flow increase with distal compression |
| Continuous (non-phasic) flow | Proximal obstruction (iliac occlusion) |
Acute vs Chronic Thrombus
| Feature | Acute DVT | Chronic DVT |
|---|---|---|
| Echogenicity | Hypoechoic/anechoic (soft) | Hyperechoic (bright, calcified) |
| Vein lumen | Distended | Contracted/irregular |
| Wall | Smooth | Thickened, irregular |
| Compressibility | Partially compressible | Rigid, non-compressible |
| Flow | Absent or marginal | Recanalized channels may appear |
| Collaterals | Uncommon | Common |
3.5 Chronic Venous Insufficiency (CVI) / Reflux
Venous reflux = retrograde (reverse) flow after augmentation or Valsalva
Normal: Reverse flow cessation within 0.5 s in superficial veins; 1.0 s in deep veins
Abnormal (reflux): Retrograde flow >0.5 s (superficial/perforators) or >1.0 s (deep veins)
| Vein | Threshold for Reflux |
|---|---|
| Great saphenous vein (GSV) | >0.5 s |
| Small saphenous vein (SSV) | >0.5 s |
| Perforator veins | >0.5 s + >3.5 mm diameter |
| Femoral vein | >1.0 s |
| Popliteal vein | >1.0 s |
Clinical Correlation (CEAP Classification):
- C0–C1: No visible disease / telangiectasias
- C2: Varicose veins
- C3: Edema
- C4a/b: Skin changes (lipodermatosclerosis, eczema)
- C5: Healed venous ulcer
- C6: Active venous ulcer
PART 4: BILATERAL COMPARISON — REPORTING STRUCTURE
A standard bilateral lower limb Doppler report addresses:
Arterial Section
- Waveform morphology at each level (triphasic / biphasic / monophasic)
- PSV values at CFA, SFA proximal/mid/distal, popliteal, ATA, PTA bilaterally
- PSV ratios at any stenotic segment
- B-mode: plaque, calcification, aneurysmal dilatation
- ABI (right and left, with individual vessel pressures)
- Impression: Normal / PAD grade / Level of disease (inflow vs. outflow vs. infrainguinal)
Venous Section
- Compressibility at every level (CFV → FV → PopV → calf veins)
- Spontaneous flow and phasicity
- Augmentation response
- Reflux testing (if varicosities or CVI suspected)
- B-mode thrombus characteristics (if DVT identified)
- Impression: No DVT / Acute DVT (site/extent) / Chronic DVT / Reflux (site/grade)
PART 5: BILATERAL LOWER LIMB STUDY — BILATERAL POSTERIOR TIBIAL ARTERIES
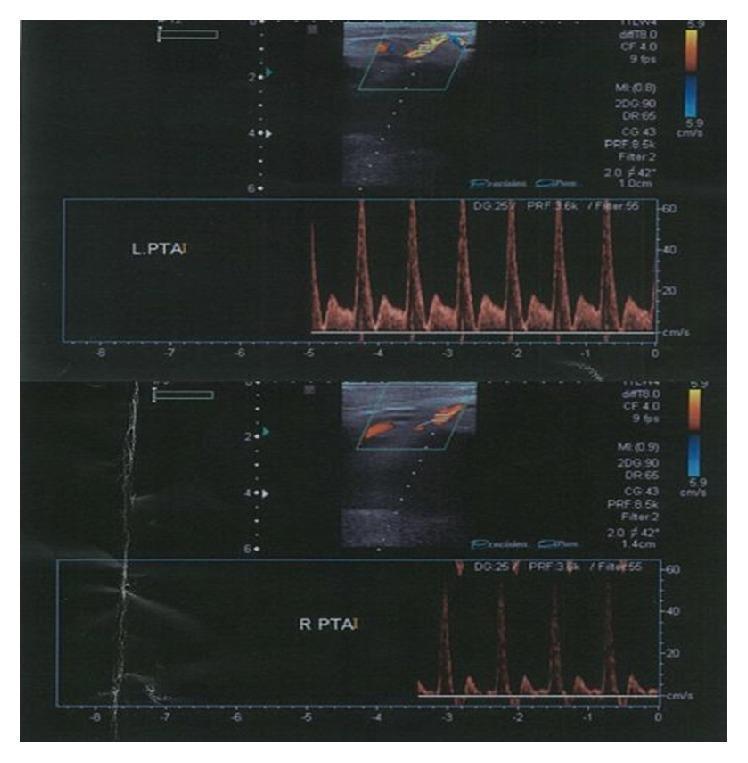
Bilateral duplex at ankle level: Left PTAI (top) — normal biphasic waveform, sharp systolic peak, ~60 cm/s PSV. Right PTAI (bottom) — diminished waveform amplitude suggesting asymmetric flow. Such side-to-side PSV comparison guides localization of disease.
PART 6: PITFALLS AND LIMITATIONS
| Pitfall | Solution |
|---|---|
| Calcified vessels (diabetics, elderly) — ABI >1.3 | Use toe-brachial index (TBI <0.7 = abnormal) |
| Non-visualized tibial veins (edema/obesity) | Increase compression force; use lower frequency |
| Isolated calf DVT missed on 2-point compression | Whole-leg ultrasound protocol |
| Hyperechoic acute thrombus mistaken for normal | Always confirm with compression; use color + spectral |
| Absent phasicity in normal patient (obese) | Repeat with Valsalva or positional changes |
| Overlying bowel gas for iliac vessels | CT angiography when ultrasound inconclusive |
SUMMARY TABLE
| Parameter | Arterial (Normal) | Venous (Normal) | Abnormal Finding |
|---|---|---|---|
| Waveform | Triphasic | Phasic, low-velocity | Monophasic / Non-phasic |
| Compressibility | N/A (arteries do not compress) | Complete collapse | Partial/no collapse → DVT |
| Color fill | Complete | Complete | Absent → occlusion |
| PSV | Segment-specific normal ranges | Low (<30 cm/s) | >2× step-up → stenosis |
| Reflux | None | None | >0.5–1.0 s → CVI |
| ABI | 0.9–1.3 | N/A | <0.9 → PAD |
This covers the complete systematic approach to bilateral lower limb Doppler interpretation — from normal physiology and waveform patterns to pathological findings in PAD, DVT, and chronic venous insufficiency.
This is a shared conversation. Sign in to Orris to start your own chat.