Mediastinal syndrome
Reading File
Finding Sources
Finding Sources
Searching PubMed
"mediastinal syndrome" superior vena cava
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from Harrison's, Tintinalli's, Harriet Lane, and Frameworks for Internal Medicine. Here is the complete answer:
Mediastinal Syndrome (Superior Vena Cava / Superior Mediastinal Syndrome)
Definition
Superior vena cava syndrome (SVCS) is the clinical manifestation of SVC obstruction causing severe reduction in venous return from the head, neck, and upper extremities.
Superior mediastinal syndrome (SMS) is SVCS with the addition of tracheal compression. In children, these two terms are used interchangeably because mediastinal pathology almost always causes both vascular and airway compromise simultaneously.
- Harrison's Principles of Internal Medicine 22E, p. 629
- Tintinalli's Emergency Medicine, p. 1005
Causes / Etiology
Malignant (majority of cases)
| Cause | Notes |
|---|---|
| Lung cancer (small-cell, squamous cell) | ~85% of malignant SVCS cases |
| Mediastinal lymphoma (non-Hodgkin's, T-lymphoblastic) | Leading cause in young adults |
| Hodgkin lymphoma | Involves mediastinum commonly but rarely causes SVCS |
| Primary mediastinal germ cell tumor | Consider in young man with mediastinal mass |
| Neuroblastoma | Especially in children |
| Metastatic disease (testicular, breast) | Small proportion |
Benign (now ~40% of adult cases due to expanding use of intravascular devices)
- Central venous catheter-related thrombosis / stenosis
- Pacemaker and defibrillator leads
- Goiter / thyromegaly
- Aortic aneurysm
- Fibrosing mediastinitis (post-irradiation, histoplasmosis, Behcet's syndrome)
In children, the most common causes are: non-Hodgkin lymphoma, ALL, neuroblastoma, and germ cell tumors.
Clinical Features
Symptoms
- Dyspnea, cough, stridor, wheezing (airway compression)
- Facial and neck swelling (especially periorbital)
- Headache, nasal congestion, epistaxis
- Hoarseness, dysphagia
- Syncope / dizziness (reduced cardiac output)
- Orthopnea - symptoms worsen lying flat or bending forward
- In severe cases: obtundation, tongue/laryngeal edema, proptosis
Signs
- Dilated neck veins, elevated JVP
- Prominent collateral veins over the anterior chest wall (see image below)
- Cyanosis and edema of face, arms, and upper chest
- Facial plethora (worsens when supine)
- Pemberton's sign: facial plethora/JVP elevation when raising arms overhead
- Horner's syndrome if sympathetic chain involved (e.g. Pancoast tumor)

SVC syndrome showing prominent collateral chest and neck veins (Tintinalli's Emergency Medicine)
Diagnosis
Imaging
Chest X-ray (two-view):
- Most common finding: widening of the superior mediastinum, predominantly right-sided
- Pleural effusion in ~25% of patients (usually right-sided, often exudative, occasionally chylous)
- A normal CXR does not exclude SVCS if clinical features are present
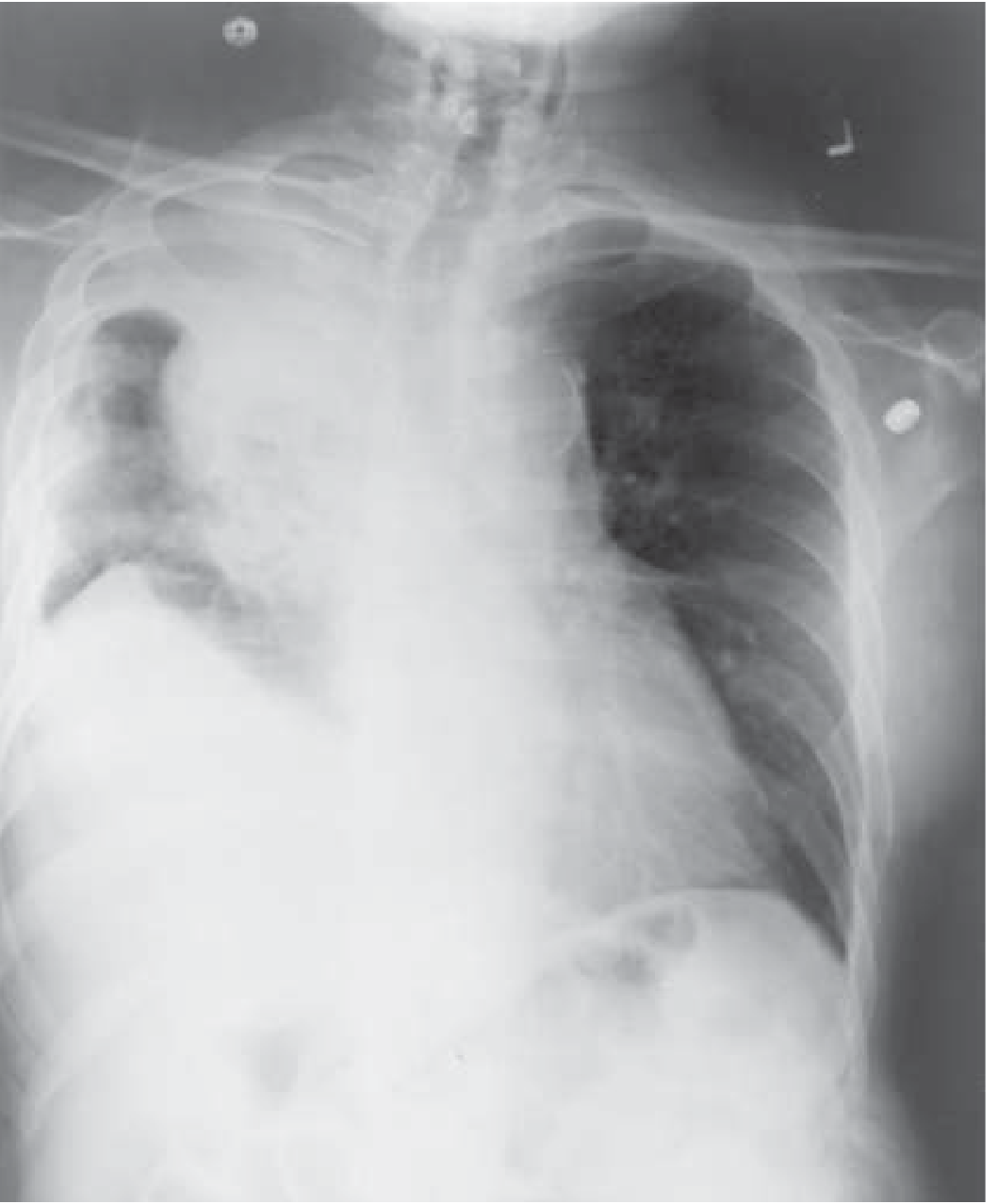
CXR: right paratracheal mass with right pleural effusion in SVCS (Harrison's, Fig. 80-1A)
CT scan (contrast-enhanced):
- Most reliable view of mediastinal anatomy
- Demonstrates extent of obstruction, collateral vessel development, and underlying mass
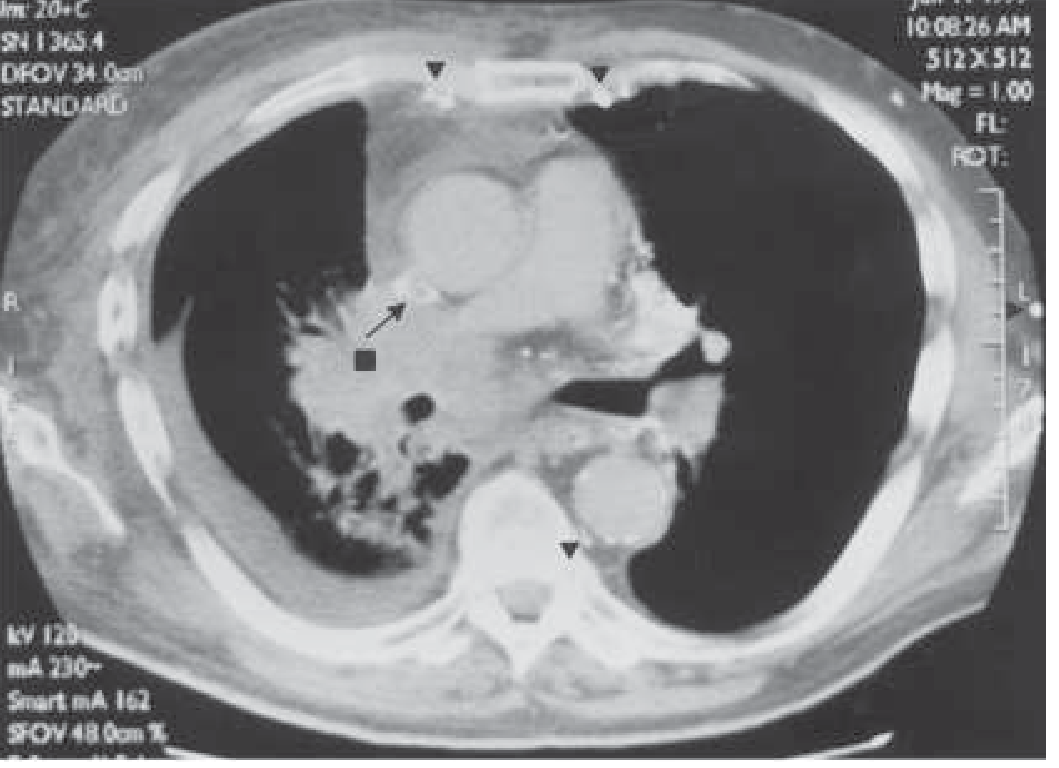
CT chest: SVC obstruction from mediastinal mass (Harrison's, Fig. 80-1B)
Important caveats for children: Supine positioning for imaging may critically compromise the airway - prefer prone position in older cooperative children. Avoid sedation - high risk for complete airway obstruction.
Tissue Diagnosis (if needed)
Pursue by the least invasive means:
- Peripheral blood flow cytometry
- Percutaneous lymph node biopsy
- Pleural / pericardial effusion drainage
Management
Emergency / Supportive
- Airway first - the one potentially life-threatening complication is tracheal obstruction; upper airway obstruction demands emergent therapy
- Head-of-bed elevation (upright/sitting position)
- High-flow supplemental oxygen
- BiPAP / heliox as temporizing measures
- Diuretics with low-salt diet for symptomatic relief
- Glucocorticoids - limited role; effective for mediastinal lymphoma masses; avoid in suspected leukemia/lymphoma without oncology consult (can mask the diagnosis)
Critical warning: Superior mediastinal syndrome is one of the few conditions in which rapid-sequence induction and intubation may be lethal if the endotracheal tube cannot bypass the site of tracheal compression. The mass is usually too distal for intubation to be effective.
Definitive Treatment (based on underlying cause)
| Underlying etiology | Treatment |
|---|---|
| Non-small-cell lung cancer, solid tumor metastases | Radiation therapy (primary) |
| Small-cell carcinoma, lymphoma, germ cell tumor | Chemotherapy |
| Thrombotic occlusion / CVC-related | Fibrinolytic therapy ± catheter removal, anticoagulation |
| Recurrent SVCS (10-30% of cases) | Intravascular self-expanding stents |
| Non-malignant mediastinal fibrosis | Surgery |
Stenting
- Endovascular stenting is increasingly used as first-line for rapid symptom relief with fewer complications
- Particularly indicated for: cerebral/laryngeal edema, postural hypotension, severe symptoms
- Caution: rapid increase in venous return post-stenting can precipitate acute heart failure
- Complications: hematoma at insertion, SVC perforation, stent migration, pulmonary embolism
Prognosis
- Most patients show clinical improvement, partly due to development of collateral circulation
- Mortality is determined by the underlying cause, not by the caval obstruction itself
- Cerebral or laryngeal edema portend a worse prognosis
Special Note: Children vs. Adults
In children, the small and compliant airway means SMS is nearly always present alongside SVCS. Young children are at disproportionate risk from airway compromise even when seemingly asymptomatic. Any planned anesthesia or sedation requires extreme caution and multidisciplinary preparation.
- Harriet Lane Handbook 23rd ed., p. 791
- Tintinalli's Emergency Medicine, p. 1005
- Harrison's Principles of Internal Medicine 22E, p. 629
This is a shared conversation. Sign in to Orris to start your own chat.