Cataract,externum hordeolum,chalazion *internum hordeolum
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I have all the information needed for a thorough comparison. Here is the complete breakdown:
Cataract, Hordeolum Externum, Chalazion, and Hordeolum Internum
1. CATARACT
Definition
Cataract is any opacity of the crystalline lens. It is the commonest cause of reversible visual disability in the world. There is no medical treatment to prevent or halt its progression - surgery is the only effective intervention. - Kanski's Clinical Ophthalmology, 10th ed.
Lens Anatomy (context for understanding cataracts)
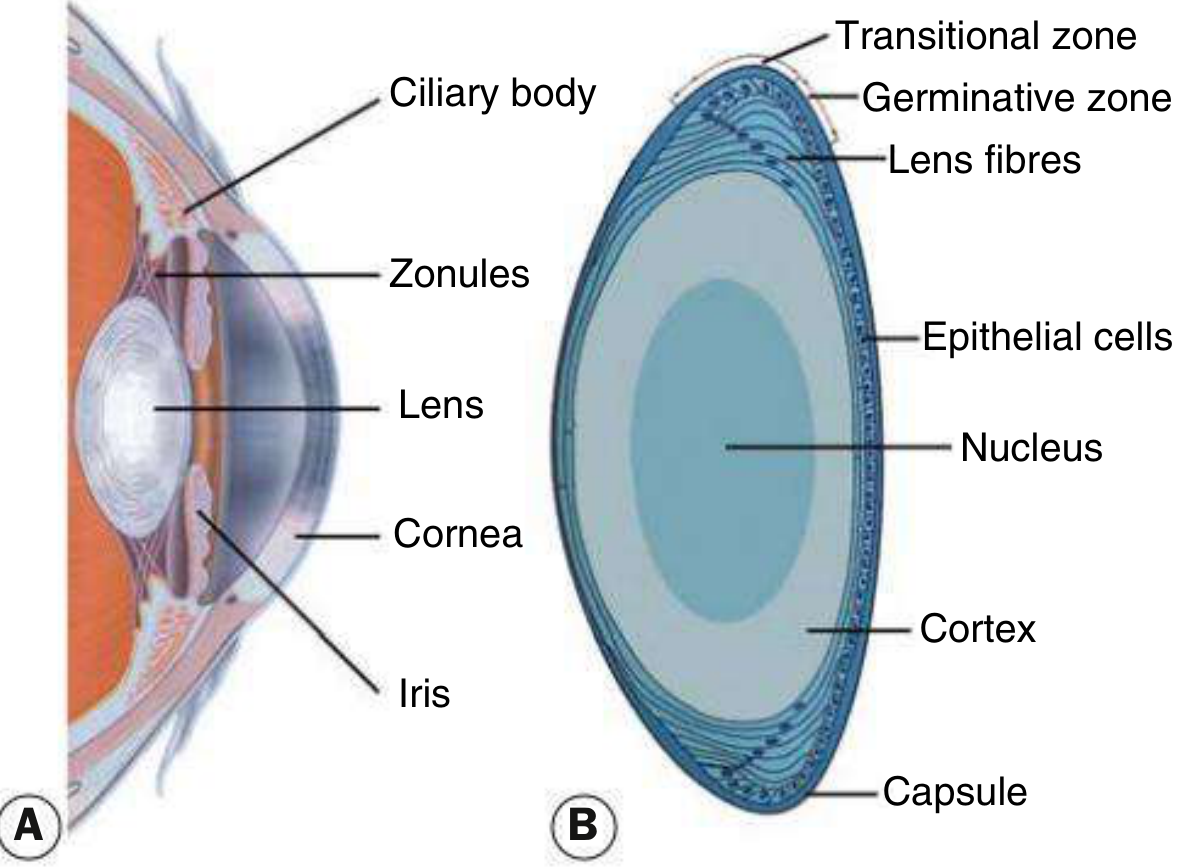
Fig. 10.1 - Kanski's Clinical Ophthalmology
The lens consists of:
- Capsule - acellular outer membrane
- Epithelial cells - cuboid, under the anterior capsule; divide in the germinative zone to form lens fibers
- Cortex - peripheral lens substance
- Nucleus - central, denser core, held by zonules from the ciliary body
Types of Acquired (Age-Related) Cataract
| Type | Location | Key Features |
|---|---|---|
| Posterior subcapsular (PSC) | Just anterior to posterior capsule | Granular/plaque-like on oblique slit lamp; black and vacuolated on retroillumination (Wedl/bladder cells); profound effect on vision due to nodal point location; glare, worse in bright light and near work |
| Nuclear sclerotic | Central nucleus | Yellowish hue (urochrome pigment); associated myopia ("second sight of the aged"); good red reflex on retroillumination; turns brown (brunescent) when advanced |
| Cortical | Anterior, posterior, or equatorial cortex | Clefts and vacuoles due to cortical hydration; cuneiform (wedge/spoke-like) opacities, often inferonasal initially; glare common |
| Christmas tree | Deep cortex and nucleus | Polychromatic needle-like formations; uncommon |
Symptoms
- Gradual, painless visual loss
- Glare (especially PSC and cortical types)
- Monocular diplopia
- Myopic shift in nuclear sclerosis ("second sight")
Causes of Non-Age-Related (Secondary) Cataract
- Metabolic: Diabetes (osmotic cortical cataract; "snowflake" in young diabetics), galactosaemia (oil-drop nuclear cataract), Wilson disease, hypocalcaemia
- Drugs: Corticosteroids (PSC), chlorpromazine, amiodarone, miotics
- Ocular disease: Uveitis, high myopia, acute angle-closure glaucoma, retinitis pigmentosa
- Radiation: Ionizing or infrared (posterior subcapsular)
- Trauma: Rosette-shaped opacities; penetrating injuries; electric injury
- Systemic: Myotonic dystrophy (Christmas tree + PSC), neurofibromatosis type 2, atopic dermatitis
Management
- Phacoemulsification with intraocular lens (IOL) implantation - the most common surgical procedure in the world
- Extracapsular extraction (ECCE) for very dense/mature cataracts
- Posterior capsule opacification (PCO) post-surgery treated with Nd:YAG laser capsulotomy
2. HORDEOLUM EXTERNUM (External Stye)
Definition
An acute, tender infection (abscess) of the glands of Zeis (sebaceous glands associated with eyelash follicles) or the hair follicle itself on the eyelid margin. - Wills Eye Manual
Key Features
- Location: Eyelid margin (external, pointing outward toward skin)
- Gland affected: Gland of Zeis (or hair follicle)
- Nature: Acute, suppurative (infectious) infection
- Causative organism: Usually Staphylococcus species
- Presentation: Acutely painful, tender, erythematous swelling on the lid margin; may come to a head and drain purulent material
- The lesion is visible as a pustule or pointing abscess at the lid margin
3. HORDEOLUM INTERNUM (Internal Stye)
Definition
An acute, tender abscess of the meibomian gland within the tarsal plate. - Wills Eye Manual
Key Features
- Location: Inside the eyelid (tarsal plate), pointing toward the conjunctival surface
- Gland affected: Meibomian gland
- Nature: Acute suppurative (infectious) - usually Staphylococcus spp.
- Presentation: Larger, more painful swelling than externum; eyelid erythema and edema; may be visible on eversion of eyelid as a conjunctival-side pointing abscess
- Can evolve into preseptal (periorbital) cellulitis if not treated
4. CHALAZION
Definition
A focal, chronic sterile granulomatous inflammation of a meibomian gland (or occasionally gland of Zeis), caused by obstruction of the gland orifice leading to lipogranuloma formation. - Wills Eye Manual; Rosen's Emergency Medicine

FIGURE 6.2.1 Chalazion - Wills Eye Manual
Key Features
- Location: Tarsal plate (usually upper lid)
- Gland affected: Meibomian gland (primarily); sometimes gland of Zeis
- Nature: Chronic, sterile, granulomatous - NOT an acute infection
- Presentation: Well-defined, firm, non-tender (or mildly tender) subcutaneous nodule; no acute redness or warmth; NOT painful unless acutely inflamed
- May evolve from an incompletely resolved hordeolum internum
- Associated with blepharitis and acne rosacea
Comparison Table
| Feature | Hordeolum Externum | Hordeolum Internum | Chalazion |
|---|---|---|---|
| Gland | Gland of Zeis / hair follicle | Meibomian gland | Meibomian gland (mainly) |
| Location | Eyelid margin (external) | Within tarsal plate (internal, points conjunctivally) | Tarsal plate, anywhere in lid |
| Nature | Acute infection (suppurative) | Acute infection (suppurative) | Chronic sterile granuloma |
| Pain | Acutely painful, tender | Acutely painful, tender | Usually non-tender or mildly tender |
| Organism | Staphylococcus spp. | Staphylococcus spp. | Sterile (no organisms) |
| Inflammation | Acute bacterial | Acute bacterial | Lipogranulomatous |
| Pointing | Outward (skin side) | Inward (conjunctival side) | Does not point (encapsulated nodule) |
| Relationship | Independent | Can evolve into chalazion | May arise from unresolved hordeolum internum |
Treatment (Hordeolum and Chalazion)
(Wills Eye Manual, 6.2)
-
Warm compresses - at least 10 minutes, 4x/day with gentle massage over the lesion (first-line for all)
-
Topical antibiotics (for hordeolum):
- Bacitracin, tobramycin, or erythromycin ointment b.i.d. x 1-2 weeks
-
Topical antibiotic/steroid (for chalazion):
- Neomycin/polymyxin B/dexamethasone ointment b.i.d. x 1-2 weeks
-
Systemic doxycycline 20-50 mg p.o. daily-b.i.d. for recurrent/multiple chalazia or ocular rosacea (antibacterial + anti-inflammatory)
-
Incision and drainage (I&D) - if hordeolum worsens or fails to respond; manage as preseptal cellulitis if spreading
-
Incision and curettage (I&C) OR intralesional triamcinolone (0.2-1.0 mL of 40 mg/mL triamcinolone mixed 1:1 with 2% lidocaine with epinephrine) for chalazia persisting >3-4 weeks
- Note: steroid injection can cause permanent depigmentation (especially in dark-skinned individuals) and rarely retrograde intra-arterial infiltration causing central retinal artery occlusion
-
All excised chalazia (especially recurrent/atypical ones) should be sent for histopathology - to exclude sebaceous carcinoma
Red Flags / Differential to Exclude
- Sebaceous gland carcinoma - suspect in older patients with recurrent chalazia, madarosis, eyelid thickening, or chronic unilateral blepharitis
- Preseptal cellulitis - lid erythema, warmth, edema extending beyond lesion
- Pyogenic granuloma - deep-red, pedunculated conjunctival lesion sometimes associated with chalazia
Sources: Kanski's Clinical Ophthalmology: A Systematic Approach, 10th ed.; Wills Eye Manual, 7th ed.; Rosen's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.