Anterior tibial artery
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive information. Here is a detailed summary of the anterior tibial artery:
Anterior Tibial Artery
Origin
The anterior tibial artery is one of the two terminal branches of the popliteal artery, arising at the inferior border of the popliteus muscle. In 92% of individuals it originates as a single branch at knee joint level (90%) or in a high position (2%); in the remaining 8% it arises as an anterior tibioperoneal trunk. When the popliteal artery trifurcates (instead of bifurcates), the anterior tibial artery has the largest diameter of the three branches.
- Imaging Anatomy, Vol. 3 (Thieme), p. 371
- Gray's Anatomy for Students, p. 730
Course
1. Entry into the anterior compartment
After its origin, the artery curves anteriorly and passes through an aperture in the upper part of the interosseous membrane to enter the anterior compartment of the leg - the only structure in the leg that crosses from posterior to anterior in this way.
2. Descent in the leg
It descends anterior (ventral) to the interosseous membrane, accompanied by the deep peroneal (fibular) nerve. It runs between:
- Tibialis anterior (medially)
- Extensor digitorum longus (laterally)
In the lower leg, the extensor hallucis longus tendon crosses the artery from lateral to medial at the ankle level. Below this crossing, the artery is sandwiched between extensor hallucis longus (medially) and extensor digitorum longus (laterally).
3. Ankle and foot
At the ankle, it passes beneath the inferior extensor retinaculum (frondiform ligament) and continues onto the dorsum of the foot as the dorsalis pedis artery.
- Imaging Anatomy, Vol. 3 (Thieme), p. 848
- Gray's Anatomy for Students, p. 730
Branches
| Branch | Course / Distribution |
|---|---|
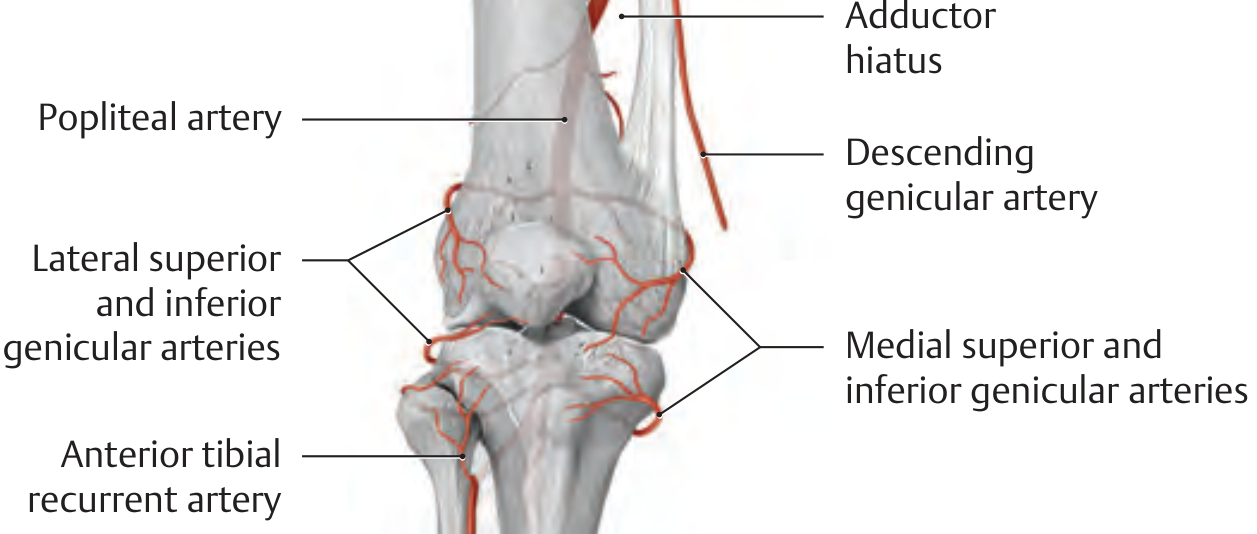
| Anterior tibial recurrent artery | Arises proximally; ascends to anastomose with inferior genicular branches of the popliteal artery around the knee |
| Posterior tibial recurrent artery | Arises proximally; ascends to knee anastomotic network |
| Muscular branches | Multiple perforating branches to anterior compartment muscles and skin |
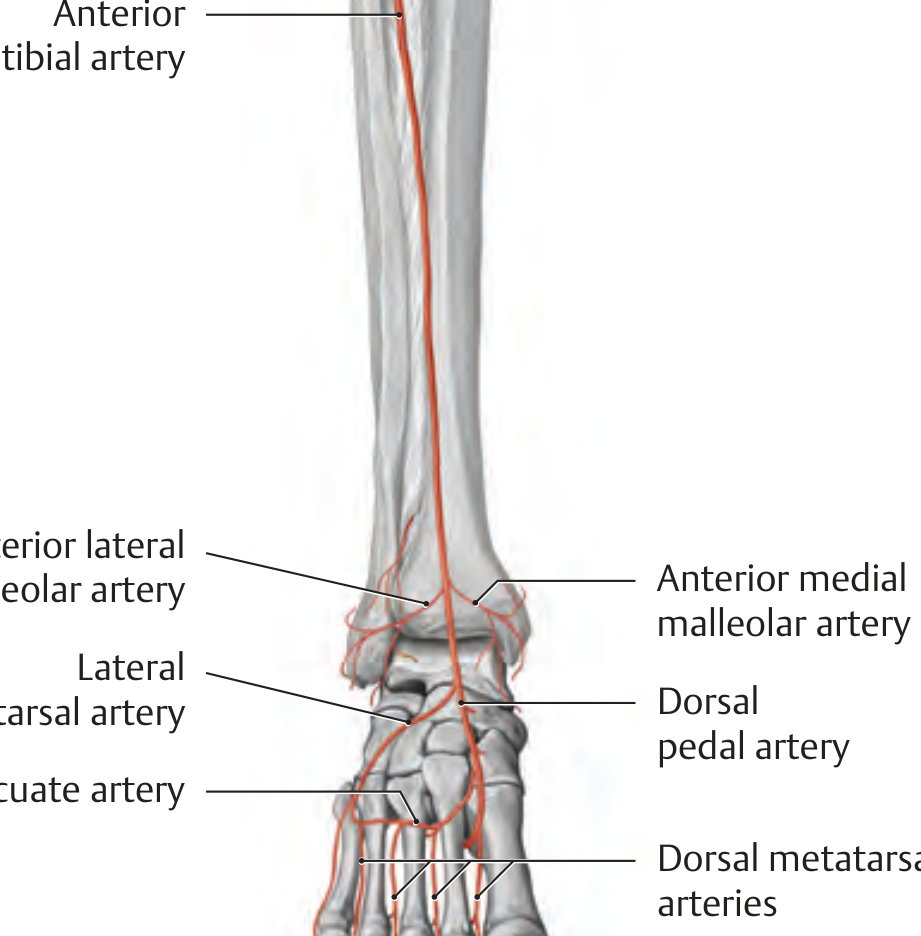
| Anterior medial malleolar artery | Passes to anteromedial ankle; anastomoses with posterior tibial and medial plantar arteries |
| Anterior lateral malleolar artery | Passes to lateral ankle; anastomoses with perforating branch of fibular artery and lateral tarsal artery |
| Dorsalis pedis artery (continuation) | Gives off: lateral tarsal artery, medial tarsal arteries, arcuate artery (→ dorsal metatarsal arteries → dorsal digital arteries) |
- THIEME Atlas of General Anatomy, p. 549
- Imaging Anatomy, Vol. 3 (Thieme), p. 371
Diagrams
Anterior tibial recurrent artery at the knee - anastomotic network:
Full course of the anterior tibial artery into the dorsalis pedis, with malleolar and tarsal branches:
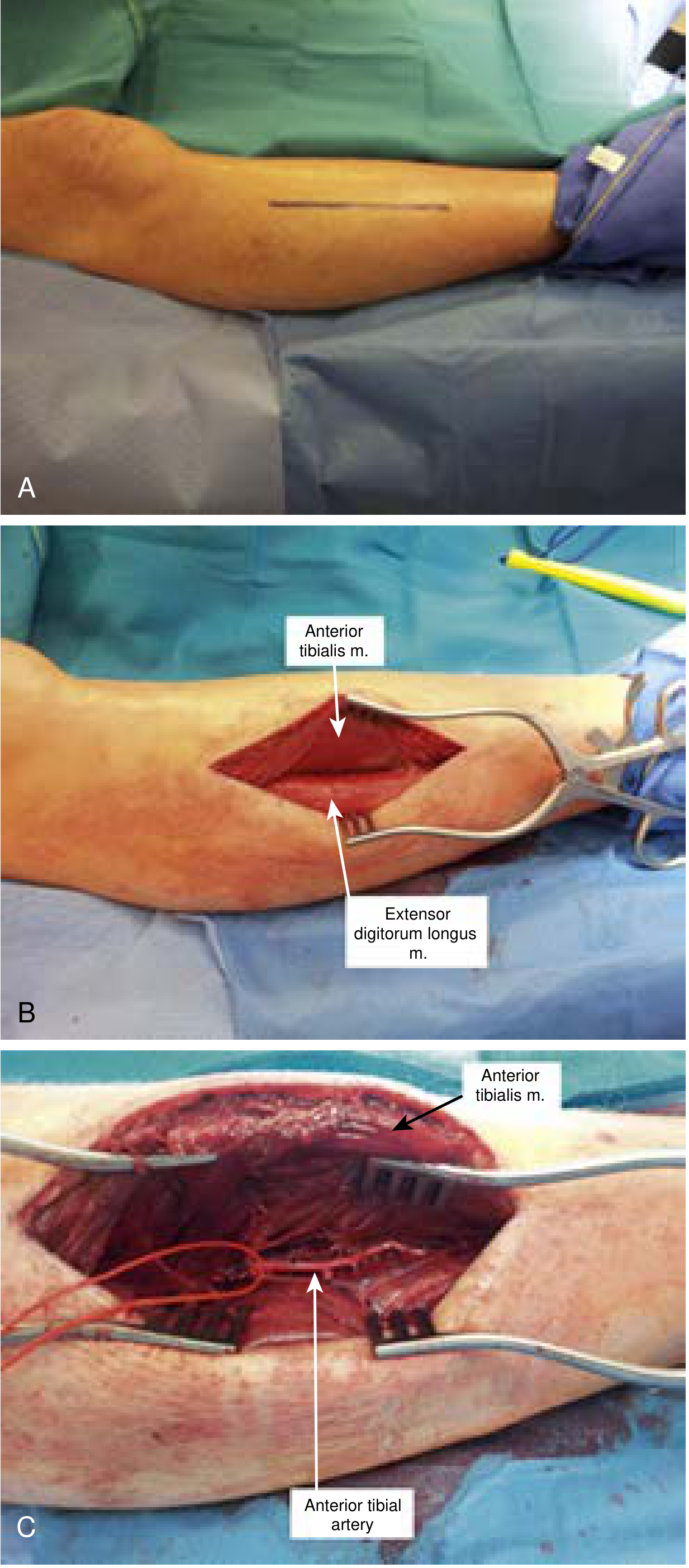
Relations (Surgical Anatomy)
The artery is exposed surgically through a longitudinal incision between the tibia and fibula. The fascial groove between tibialis anterior (medially) and extensor digitorum longus (laterally) is opened, revealing the artery alongside its accompanying veins and the deep peroneal nerve.
- Current Surgical Therapy 14e
Clinical Relevance
-
Peripheral artery disease / critical limb ischemia: The anterior tibial artery is a target for infrapopliteal bypass grafting (e.g., femoro-anterior tibial bypass with reversed or non-reversed great saphenous vein). Five-year limb salvage rates exceed 80% with autogenous conduit.
-
Anterior compartment syndrome: Raised pressure in the anterior compartment can compress the anterior tibial artery and deep peroneal nerve, causing ischaemia and foot drop.
-
Common peroneal neuropathy: Rare complication of anterior tibial artery occlusion due to shared proximity with the deep peroneal nerve.
-
Dorsalis pedis pulse: Clinically palpated between extensor hallucis longus and extensor digitorum longus tendons on the dorsum of the foot - this is the continuation of the anterior tibial artery. Absence suggests peripheral vascular disease.
-
Talus blood supply: The anterior tibial artery contributes 36.2% of the blood supply to the talus (posterior tibial 47.0%, peroneal 16.9%) - relevant in talar fractures and avascular necrosis risk.
-
Current Surgical Therapy 14e; Campbell's Operative Orthopaedics 15e; Rosen's Emergency Medicine
Superior extensor retinaculum
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
By bd chaurasia
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Unfortunately, BD Chaurasia's Human Anatomy is not available in the medical textbook library. The library does not contain that title.
Here is what I can tell you based on the standard BD Chaurasia description, which I can provide from memory (it closely matches other authoritative anatomy texts):
Superior Extensor Retinaculum - BD Chaurasia
Definition
A thickened band of deep fascia (crural fascia) situated in the distal part of the leg, just above the ankle joint.
Attachments
- Laterally: Lower end of the fibula (anterior surface / lateral malleolus)
- Medially: Lower end of the tibia (anterior surface / medial malleolus / anterior crest of tibia)
It is essentially a transverse rectangular band stretching between the two bones of the leg just above the ankle.
Structures Passing Deep to It
All four tendons of the anterior compartment pass beneath the superior extensor retinaculum from medial to lateral:
| Order (medial → lateral) | Structure |
|---|---|
| 1 | Tibialis anterior tendon |
| 2 | Extensor hallucis longus tendon |
| 3 | Anterior tibial vessels + deep peroneal nerve |
| 4 | Extensor digitorum longus tendon |
| 5 | Peroneus tertius tendon (when present) |
In about 25% of individuals, the tibialis anterior has its own separate tunnel formed by a split in the retinaculum fibers.
Function
Prevents bowstringing of the extensor tendons during dorsiflexion of the foot at the ankle.
Synovial Sheaths
The extensor tendons do not have synovial sheaths at the level of the superior extensor retinaculum (sheaths begin at the level of the inferior extensor retinaculum below). However, the tibialis anterior occasionally may have a sheath here.
Relation to Inferior Extensor Retinaculum
Lies above (proximal to) the inferior extensor retinaculum (which is Y-shaped / frondiform and is situated over the ankle joint and tarsus proper).
Note: BD Chaurasia's Human Anatomy is not available in this library's textbook database, so the above is based on standard anatomical descriptions consistent with Chaurasia's style and content. The structural details above are verified against Gray's Anatomy for Students and the Thieme Imaging Anatomy Atlas (Vol. 3) available in the library. If you have a specific page or topic from Chaurasia you want me to cross-reference, I am happy to do so using the available textbooks.
Calcium homeostasis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have comprehensive material. Here is a complete, well-illustrated answer:
Calcium Homeostasis
1. Body Calcium Distribution
An adult human body contains approximately 1000-1300 g of calcium, distributed as:
| Compartment | % of total |
|---|---|
| Bone and teeth (as hydroxyapatite) | 99.3% |
| Soft tissues (intracellular) | 0.6% |
| Extracellular fluid (incl. plasma) | 0.1% |
Intracellular free Ca²⁺ is maintained at a very low concentration (~100 nM / 0.1 µmol), creating a 10,000-fold gradient compared to extracellular Ca²⁺ (~1 mM). This gradient is physiologically critical.
- Brenner and Rector's The Kidney, p. 796
2. Plasma Calcium - Normal Values and Fractions
Normal total serum calcium: 8.6-10.3 mg/dL (2.15-2.57 mmol/L)
Calcium in blood exists in three fractions:
| Fraction | % | Notes |
|---|---|---|
| Protein-bound | 40% | 90% bound to albumin, 10% to globulins |
| Ionized (free) Ca²⁺ | 48% | Physiologically active; normal 4.65-5.28 mg/dL |
| Complexed (phosphate, citrate, lactate, bicarbonate) | 12% | Filterable but not active |
Ionized Ca²⁺ is the physiologically active form - it regulates CaSR signaling, cardiac contractility, neuromuscular activity, and bone mineralization.
Albumin Correction Formula
When albumin is low, total calcium falls but ionized calcium may be normal:
Adjusted Ca (mg/dL) = Measured Ca (mg/dL) + 0.8 × (4 - albumin [g/dL])
Important: Alkalosis decreases free Ca²⁺ (enhanced albumin binding); acidosis increases free Ca²⁺ (H⁺ displaces Ca²⁺ from albumin). A pH drop of 0.1 raises ionized Ca²⁺ by ~0.1 mEq/L.
- Brenner and Rector's The Kidney, pp. 796-797
3. The Three Organs and Three Hormones
Ca²⁺ homeostasis involves the coordinated interaction of three organ systems (intestine, kidney, bone) regulated by three hormones (PTH, Vitamin D, Calcitonin).
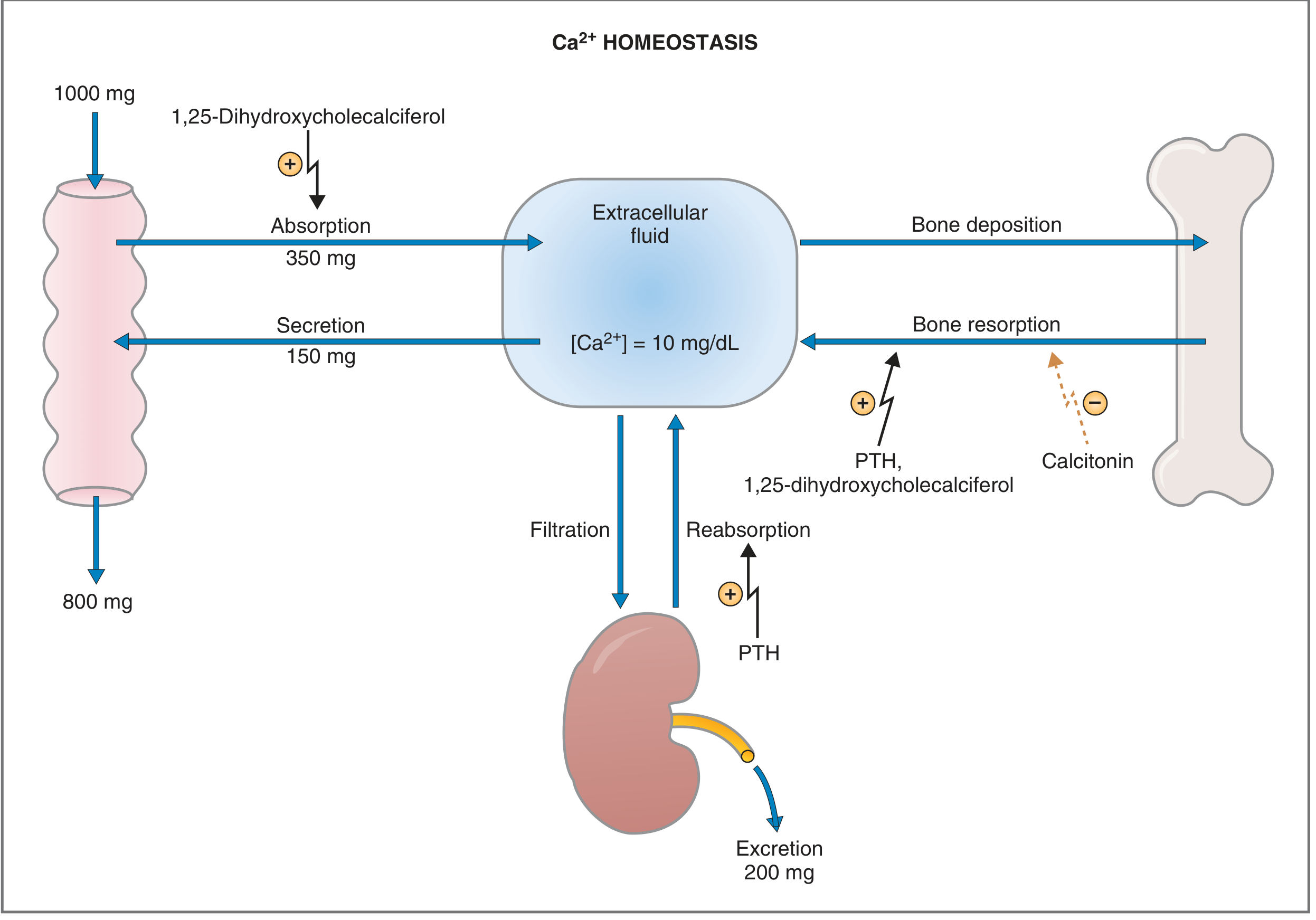
Fig. 9.35 - Costanzo Physiology: Ca²⁺ homeostasis in an adult eating 1000 mg/day elemental Ca²⁺
Daily Calcium Balance (in a person on 1000 mg/day)
- Ingested: 1000 mg/day
- GI absorption: 350 mg absorbed; 150 mg secreted back (salivary, pancreatic, intestinal fluids) → net absorption = 200 mg/day
- Fecal excretion: 800 mg/day
- Renal filtration: ~10 g/day filtered; ~200 mg excreted in urine (rest reabsorbed)
- Bone: 500 mg released (resorption) = 500 mg deposited (formation) → net zero in young adults
4. Parathyroid Hormone (PTH)
Structure
- 84-amino acid single-chain polypeptide
- Synthesized as preproPTH (115 aa) → signal peptide cleaved → proPTH (90 aa) → 6 more aa cleaved in Golgi → final PTH (84 aa)
- Biologic activity resides entirely in the N-terminal 34 amino acids
- Secreted by chief cells of the 4 parathyroid glands
Regulation of Secretion - Calcium-Sensing Receptor (CaSR)
The parathyroid cell membrane contains Ca²⁺-sensing receptors (CaSR) linked via Gq protein to phospholipase C:
- High extracellular Ca²⁺ → Ca²⁺ binds CaSR → activates phospholipase C → ↑ IP₃/Ca²⁺ → inhibits PTH secretion
- Low extracellular Ca²⁺ → decreased CaSR binding → stimulates PTH secretion (within seconds)
- PTH secretion is maximal when plasma Ca²⁺ falls to ~7.5 mg/dL
Other regulators of PTH secretion:
- Hypomagnesemia → stimulates PTH (but severe chronic hypomagnesemia, e.g. alcoholism, inhibits PTH synthesis and secretion)
- 1,25-dihydroxycholecalciferol → directly inhibits PTH synthesis and secretion
- Hyperphosphatemia and elevated FGF-23 → stimulate PTH
- Chronic hypocalcemia → secondary hyperparathyroidism (parathyroid hyperplasia, increased PTH synthesis over 24-48 hours)
Actions of PTH (all raise plasma Ca²⁺)
PTH receptor is coupled via Gs protein → adenylyl cyclase → ↑ cAMP → protein kinases
| Target | Action | Result |
|---|---|---|
| Bone | Indirect stimulation of osteoclasts via osteoblast-derived cytokines (RANKL) - receptors on osteoblasts, not osteoclasts | ↑ Bone resorption → releases Ca²⁺ and phosphate into ECF |
| Kidney - proximal tubule | Inhibits Na⁺-phosphate cotransport | ↓ Phosphate reabsorption → phosphaturia (clears phosphate that would otherwise complex ECF Ca²⁺) |
| Kidney - distal tubule | Stimulates Ca²⁺ reabsorption | ↑ Plasma Ca²⁺ |
| Kidney - proximal tubule | Activates renal 1α-hydroxylase | ↑ Conversion of 25-OH-D₃ → 1,25-(OH)₂-D₃ (active vitamin D) |
| Intestine | Indirect - via 1,25-(OH)₂-D₃ | ↑ Ca²⁺ absorption from gut |
Note: PTH phosphaturic action is critical - if phosphate released from bone were not cleared renally, it would complex with the released Ca²⁺ in ECF and blunt the rise in ionized Ca²⁺.
- Costanzo Physiology 7e, pp. 453-455
5. Vitamin D (Calcitriol)
Synthesis Pathway
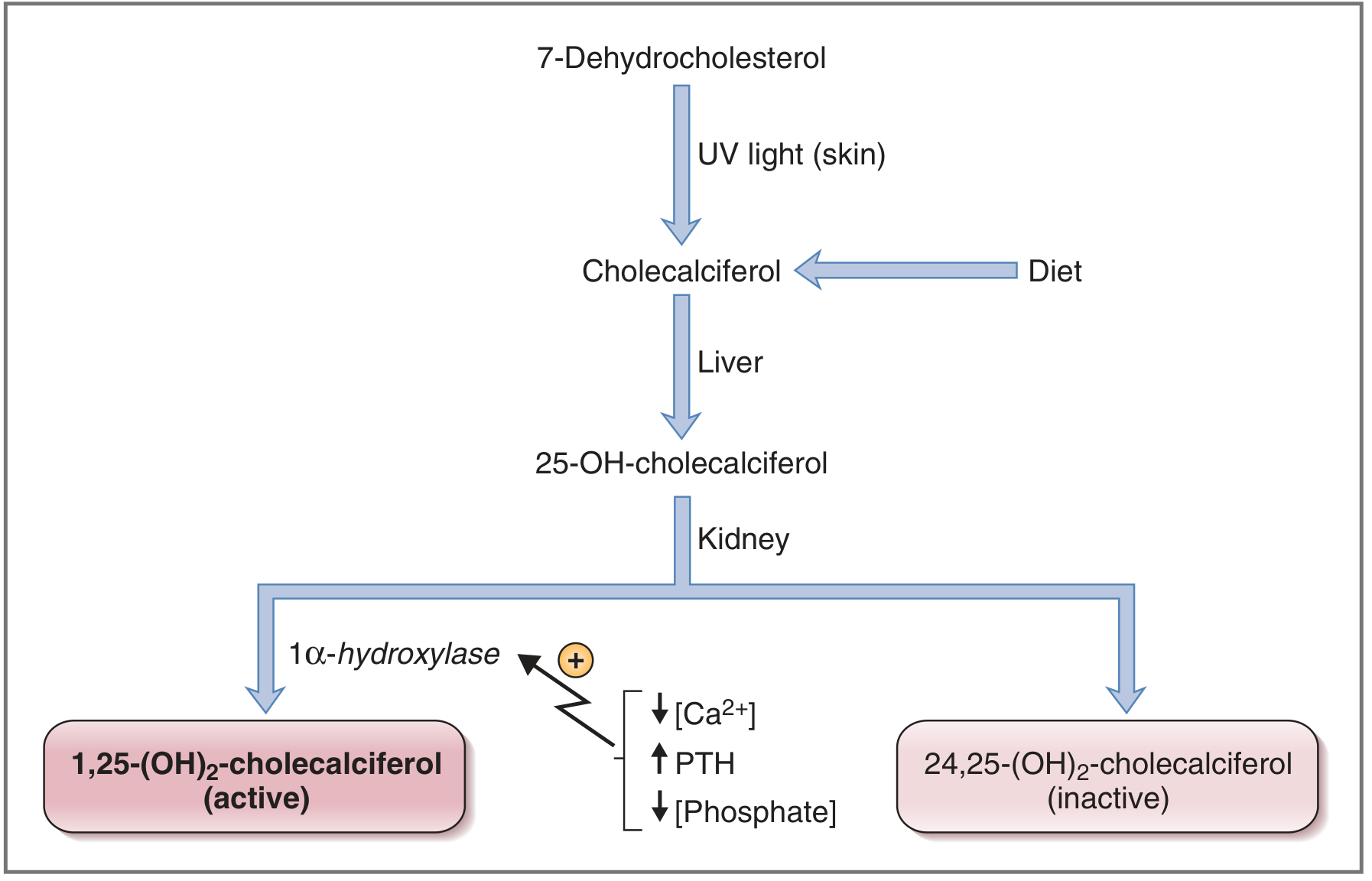
- Skin: 7-dehydrocholesterol → cholecalciferol (UV light) OR from diet
- Liver: Cholecalciferol → 25-hydroxycholecalciferol (25-OH-D₃) - the main circulating form, bound to α-globulin; biologically inactive
- Kidney (mitochondrial 1α-hydroxylase):
- If Ca²⁺ deficient → 1,25-(OH)₂-D₃ (calcitriol) - the active form
- If Ca²⁺ sufficient → 24,25-(OH)₂-D₃ - inactive
1α-hydroxylase is activated by: ↓ plasma Ca²⁺, ↑ PTH, ↓ plasma phosphate
Actions of 1,25-(OH)₂-D₃ (Calcitriol)
Acts as a steroid hormone - stimulates gene transcription and new protein synthesis:
| Target | Action |
|---|---|
| Intestine (major site) | Induces synthesis of calbindin D-28K (Ca²⁺-binding protein) → ↑ Ca²⁺ and phosphate absorption |
| Kidney | ↑ Ca²⁺ reabsorption AND ↑ phosphate reabsorption (unlike PTH which causes phosphaturia) |
| Bone | Acts synergistically with PTH → stimulates osteoclast activity → bone resorption to supply Ca²⁺/PO₄ for new bone mineralization |
Overall goal: raise Ca²⁺ × phosphate product to promote bone mineralization.
Intestinal Mechanism (Calbindin D-28K)
- Ca²⁺ diffuses across luminal membrane down electrochemical gradient
- Binds intracellularly to calbindin D-28K (a cytosolic shuttle/buffer)
- Ca²⁺-ATPase pumps Ca²⁺ across basolateral membrane into blood
6. Calcitonin
- Secreted by parafollicular C cells of the thyroid
- Released in response to hypercalcemia
- Inhibits osteoclast activity → ↓ bone resorption → ↓ plasma Ca²⁺
- Less potent than PTH in day-to-day calcium regulation; more important during growth, pregnancy, and lactation
- Clinically used pharmacologically in Paget's disease and hypercalcemia
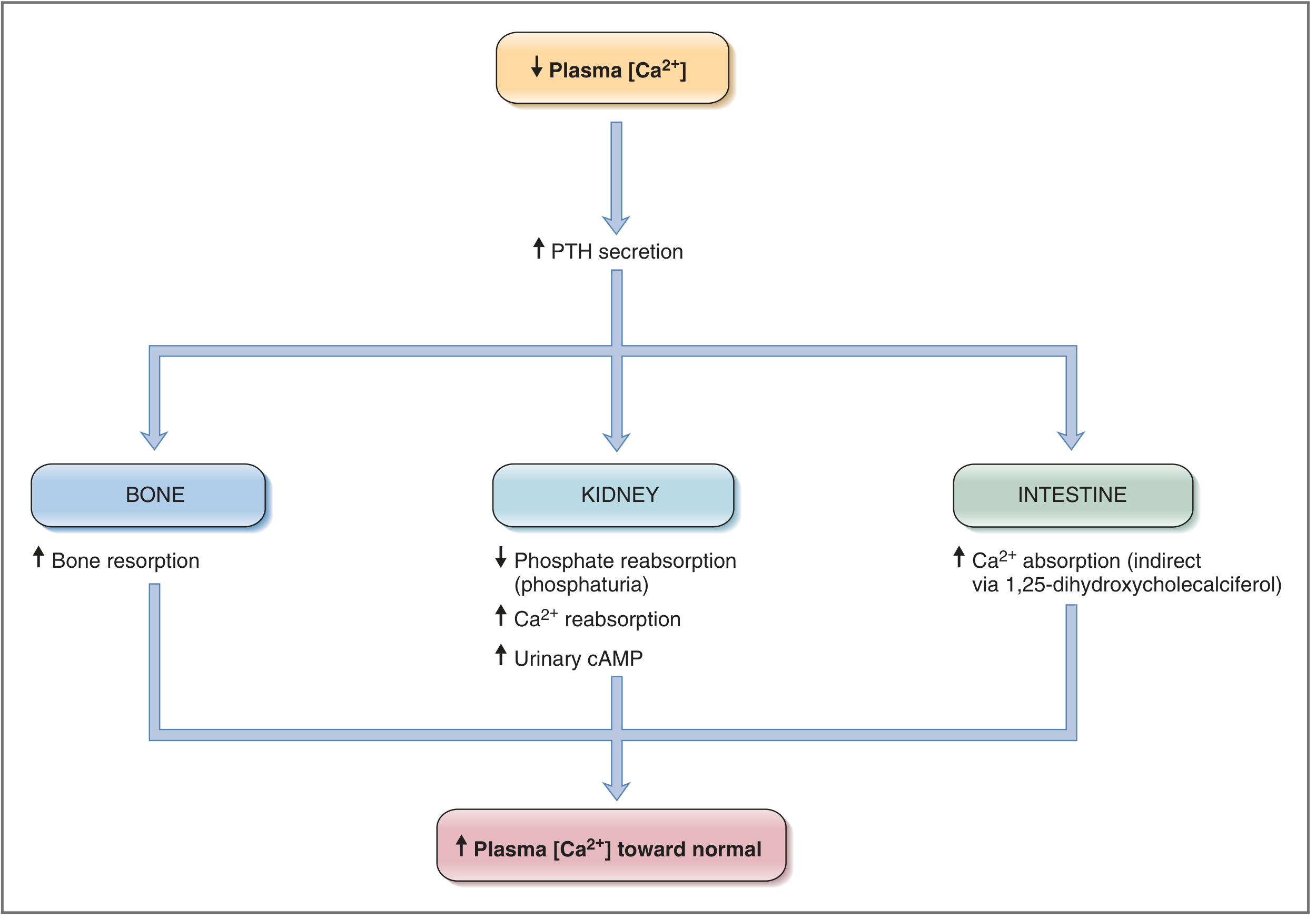
7. Summary: Response to Hypocalcemia
↓ Plasma Ca²⁺
↓
↑ PTH secretion (within seconds via CaSR)
├── Bone: ↑ osteoclast resorption → Ca²⁺ + PO₄ released
├── Kidney proximal: ↑ 1α-hydroxylase → ↑ active Vitamin D
├── Kidney proximal: ↓ phosphate reabsorption (phosphaturia) → prevents Ca-PO₄ complexing
├── Kidney distal: ↑ Ca²⁺ reabsorption
└── Intestine (via Vitamin D): ↑ Ca²⁺ absorption (calbindin D-28K)
↓
↑ Plasma Ca²⁺ → normal → inhibits PTH (negative feedback)
8. Clinical Disorders of Calcium Homeostasis
| Disorder | Key Mechanism |
|---|---|
| Hypercalcemia | Most commonly: ↑ osteoclastic bone resorption (primary hyperparathyroidism, malignancy via PTHrP) |
| Hypocalcemia | Hypoparathyroidism, vitamin D deficiency, hypomagnesemia, CKD |
| Rickets (children) | Vitamin D deficiency → insufficient Ca²⁺/PO₄ for growing bone mineralization |
| Osteomalacia (adults) | Vitamin D deficiency → softening of weight-bearing bones |
| Secondary hyperparathyroidism | Chronic hypocalcemia/renal disease → parathyroid hyperplasia, ↑↑ PTH |
| Cell injury (intracellular Ca²⁺) | Ischemia/toxins → excessive cytosolic Ca²⁺ → activates phospholipases, proteases, endonucleases, ATPases → cell death |
- Costanzo Physiology 7e; Brenner and Rector's The Kidney; Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.