Leukemoid reaction ,hemoblastosis, leukemia and DD between them
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
Now I have comprehensive data. Let me compile a thorough, well-structured answer.
Leukemoid Reaction, Hemoblastosis, Leukemia, and Differential Diagnosis
1. Leukemoid Reaction
Definition
A leukemoid reaction is an excessive leukocytic response in the peripheral blood - leukocytosis of ≥50 × 10⁹/L (i.e., >50,000/µL) with a pronounced left shift (immature granulocytes in blood), occurring as a reactive, non-neoplastic response to an underlying stimulus.
It mimics the appearance of leukemia on a peripheral smear, hence the name.
(Henry's Clinical Diagnosis and Management by Laboratory Methods)
Peripheral Blood Smear Appearance
The peripheral blood shows:
- Left shift: bands, metamyelocytes, myelocytes in circulation
- Toxic granulation of neutrophils (coarse dark granules)
- Döhle bodies (pale blue cytoplasmic inclusions)
- Cytoplasmic vacuoles
Below is a peripheral blood smear from a leukemoid reaction patient - morphologically indistinguishable from CML without molecular testing:
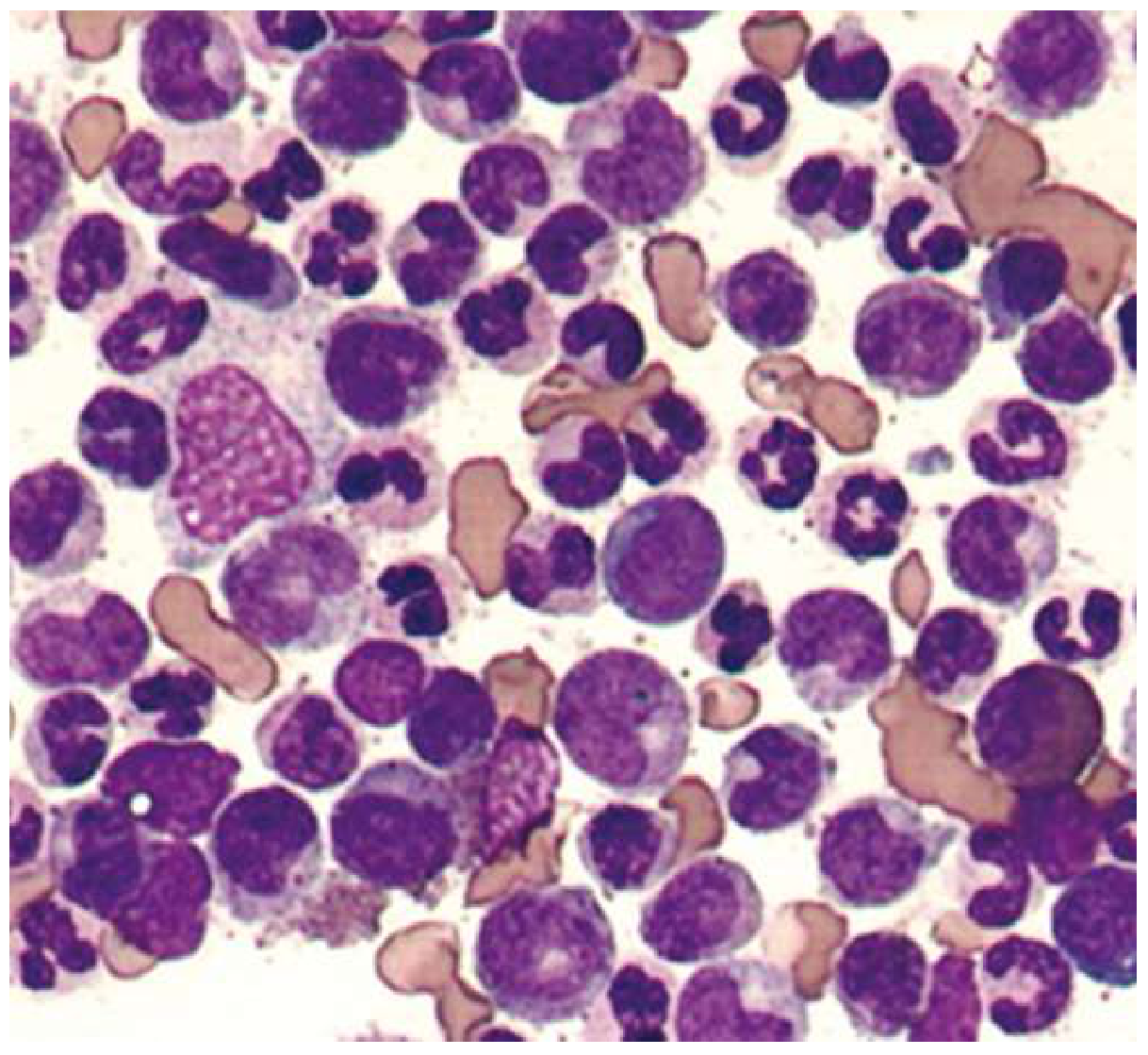
Figure: Peripheral blood from a patient with leukemoid reaction. Without BCR-ABL testing, it is morphologically identical to CML. - Goldman-Cecil Medicine
Types of Leukemoid Reaction
| Type | Key Features | Common Causes |
|---|---|---|
| Neutrophilic (most common) | Left shift, toxic changes | Bacterial infection (TB, diphtheria), malignancy (Hodgkin lymphoma), hemolysis, burns, eclampsia, toxins |
| Eosinophilic | Eosinophilic myelocytes in blood, WBC >50×10⁹/L | Parasitic infection (especially in children) |
| Lymphocytic | Very high counts of normal-appearing lymphocytes | Pertussis, infectious lymphocytosis, infectious mononucleosis (atypical lymphocytes) |
| Monocytic | Elevated monocytes | Rare; chronic infections |
Leukoerythroblastic Reaction (special variant)
When a neutrophilic leukemoid reaction is accompanied by circulating normoblasts (nucleated RBCs), it is called a leukoerythroblastic reaction. This occurs in:
- Metastatic carcinoma infiltrating bone marrow
- Marrow fibrosis
- Marrow infection
- Benign conditions: GI bleeding, hemolytic anemia
2. Hemoblastosis
Definition and Concept
"Hemoblastosis" is a broad term used primarily in Eastern European/Russian medical tradition (and historically in some pathology texts) to describe the entire group of tumors (neoplasms) arising from hematopoietic and lymphoid tissue. It is essentially synonymous with the modern WHO category of hematolymphoid neoplasms.
The term encompasses:
- Leukemias - systemic diseases with bone marrow involvement and peripheral blood tumor cells
- Hematosarcomas / lymphomas - solid tumor masses of hematopoietic origin (e.g., lymphoma), where cells do not necessarily circulate freely in peripheral blood
- Myeloproliferative neoplasms - clonal proliferations of bone marrow precursors (CML, polycythemia vera, essential thrombocythemia, myelofibrosis)
- Myelodysplastic syndromes (MDS) - clonal hematopoietic disorders with dysplasia and cytopenias
So: Hemoblastosis = Leukemias + Lymphomas + MPN + MDS (all primary hematologic malignancies).
Classification of Hemoblastosis
Hemoblastosis
├── Leukemias (marrow/blood-based)
│ ├── Acute: AML, ALL
│ └── Chronic: CML, CLL, hairy cell, etc.
├── Lymphomas (lymphoid tissue-based)
│ ├── Hodgkin lymphoma
│ └── Non-Hodgkin lymphoma (B-cell, T-cell, NK-cell)
├── Myeloproliferative Neoplasms (MPN)
│ ├── CML (BCR-ABL+)
│ ├── Polycythemia vera (JAK2+)
│ ├── Essential thrombocythemia (JAK2/CALR/MPL+)
│ └── Primary myelofibrosis
└── Myelodysplastic Syndromes (MDS)
3. Leukemia
Definition
Leukemia is a clonal neoplastic proliferation of hematopoietic stem/progenitor cells that infiltrates the bone marrow, circulates in peripheral blood, and may infiltrate other organs. Unlike lymphomas, leukemias are defined by their systemic/blood involvement.
WHO Classification (Modern)
A. By acuity:
- Acute leukemia: >20% blasts in bone marrow; rapidly fatal without treatment; cells are arrested in early differentiation
- Chronic leukemia: Mature-appearing cells predominate; more indolent course; blast crisis may occur later
B. By lineage:
- Myeloid: originates from myeloid progenitors (AML, CML, CMML)
- Lymphoid: originates from lymphoid progenitors (ALL, CLL, T-cell leukemia)
Major Leukemia Types
| Leukemia | Typical Age | WBC | Key Cells | Hallmark |
|---|---|---|---|---|
| AML | Adults (median 68) | Variable | Myeloblasts (Auer rods) | >20% blasts; t(15;17) in APL |
| ALL | Children (peak 2-5y) | Variable | Lymphoblasts | TdT+; t(9;22) in Ph+ ALL |
| CML | 40-60y | Very high (>100×10⁹/L) | All granulocytic stages | Philadelphia chromosome t(9;22); BCR-ABL |
| CLL | Elderly (>60y) | Elevated | Small mature lymphocytes, smudge cells | CD5+CD19+; indolent |
CML in Detail (most relevant to DD)
- Affects 95% of patients with the Philadelphia chromosome (t(9;22), BCR-ABL1 fusion)
- Characterized by "panmyelosis": increased ALL stages of granulocytic series, plus concomitant basophilia, eosinophilia, anemia, thrombocytosis
- Classic smear shows myelocyte "peak" (myelocytes > metamyelocytes)
- Treated with tyrosine kinase inhibitors (imatinib/Gleevec)
4. Differential Diagnosis: Leukemoid Reaction vs. CML (Leukemia)
This is the single most clinically important DD - both can present with WBC >50,000/µL and immature granulocytes in blood.
Comparison Table
| Feature | Leukemoid Reaction | CML (Chronic Leukemia) |
|---|---|---|
| WBC | Usually 50-100 ×10⁹/L | Often >100 ×10⁹/L |
| Cause | Reactive (infection, malignancy, toxin) | Clonal neoplasm |
| Immature cells | Left shift with toxic changes | Myelocyte "peak" (more myelocytes than metamyelocytes), no toxic changes |
| Basophilia | Absent | Present (characteristic) |
| Eosinophilia | Absent (unless eosinophilic type) | Often present |
| Toxic granulation | Present | Absent |
| Döhle bodies | Present | Absent |
| Thrombocytosis | Absent | Often present |
| Anemia | Absent (unless underlying) | Often present |
| Splenomegaly | Mild or absent | Prominent |
| NAP/LAP score | Normal or HIGH (≥80) | Low or zero (<20) |
| Philadelphia chromosome | Absent | Present in 95% |
| BCR-ABL1 fusion | Absent | Present |
| Bone marrow | Reactive hyperplasia; normal cytogenetics | Hypercellular; Ph+ chromosome on cytogenetics |
| CRP/ESR | Often elevated | Usually normal |
| Resolution | Resolves when cause treated | Persists and progresses |
NAP (Neutrophil Alkaline Phosphatase) / LAP (Leukocyte Alkaline Phosphatase) score is a historically important bedside test:
- Leukemoid reaction: NAP normal or elevated (>80 units)
- CML: NAP markedly decreased (<20 units, often 0)
Lymphocytic Leukemoid Reaction vs. CLL
| Feature | Lymphocytic Leukemoid Reaction | CLL |
|---|---|---|
| Patient age | Any age; children (pertussis) | Elderly (>60 years) |
| Lymphocyte morphology | Normal-appearing or atypical (reactive) | Small, uniform mature lymphocytes; smudge cells |
| CD5 expression | Absent | CD5+ (characteristic) |
| Monoclonality | Polyclonal | Monoclonal |
| Course | Self-limited | Chronic/progressive |
Key Diagnostic Algorithm
High WBC (>50,000/µL) + left shift
↓
Is there an obvious reactive cause?
(infection, burns, malignancy, eclampsia)
↓ ↓
YES NO
↓ ↓
Check NAP score Suspect primary hematologic disease
↓ ↓
HIGH LOW → BCR-ABL testing → CML
(Leukemoid) ↑
Also check: basophilia, eosinophilia,
panmyelosis, splenomegaly, cytogenetics
Summary Table: Leukemoid Reaction vs. Hemoblastosis vs. Leukemia
| Leukemoid Reaction | Hemoblastosis (broad) | Leukemia | |
|---|---|---|---|
| Nature | Reactive, non-neoplastic | Umbrella term for all hematologic neoplasms | Neoplastic, clonal |
| Clonality | Polyclonal | Monoclonal/neoplastic | Monoclonal |
| Reversibility | Reverses with cause treatment | Progressive; requires treatment | Progressive without therapy |
| Includes | - | Leukemias + Lymphomas + MPN + MDS | Subset of hemoblastosis |
| Bone marrow | Reactive hyperplasia | Neoplastic infiltration | Neoplastic infiltration/blast expansion |
| Cytogenetics | Normal | Often abnormal | Often abnormal (AML: t(15;17); CML: Ph+) |
| NAP score | Normal/high | Low (in CML) / variable | Low (CML); variable (others) |
| Peripheral blood | Left shift, toxic granules, Döhle bodies | Blasts, abnormal cells | Blasts or very high mature clonal cells |
Sources:
- Henry's Clinical Diagnosis and Management by Laboratory Methods, pp. 734-735 (Leukemoid Reactions section)
- Goldman-Cecil Medicine, pp. 1763-1764 (Leukemoid reaction, CML differential)
- Henry's Clinical Diagnosis and Management by Laboratory Methods, p. 132 (Elevated WBC, NAP score, CML vs leukemoid)
This is a shared conversation. Sign in to Orris to start your own chat.