Furuncle on armpit
Reading File
Finding Sources
Finding Sources
Searching PubMed
furuncle abscess management treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Here is the full clinical answer:
Furuncle (Boil) of the Axilla
Definition
A furuncle (boil) is a focal suppurative (pus-forming) inflammation of a hair follicle and the surrounding subcutaneous tissue caused by Staphylococcus aureus. When it occurs in the axilla, the rich density of hair follicles and apocrine sweat glands in that area makes it a particularly common and troublesome site.
- Robbins Pathologic Basis of Disease, p. 343
- S Das Manual on Clinical Surgery 13th Edition, p. 51
Why the Axilla is a Common Site
The axilla is predisposed because:
- High density of hair follicles
- Apocrine sweat glands are concentrated here (infection of these glands is called hidradenitis)
- Warm, moist, occluded environment promotes bacterial growth
- Friction from movement and clothing
- Shaving creates micro-abrasions that allow S. aureus entry
Other common friction sites include the inframammary fold, buttocks, and inner thigh.
- Textbook of Family Medicine 9e, p. 937
Pathophysiology
The infection begins in a single hair follicle. S. aureus uses several virulence factors to evade host immunity:
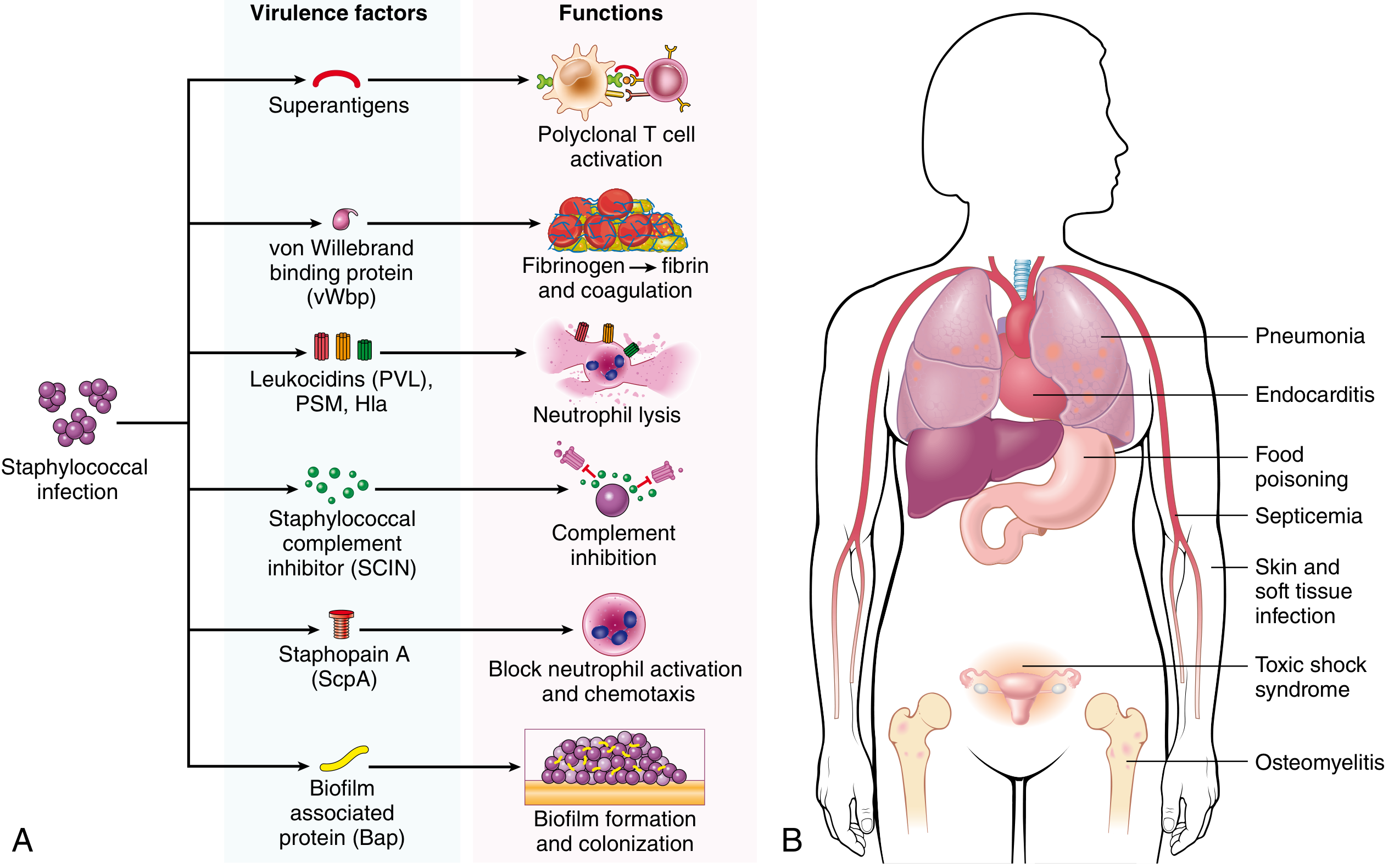
Key virulence mechanisms include:
- Leukocidins (PVL) - lyse neutrophils, impairing early defense
- Staphopain A (ScpA) - blocks neutrophil activation and chemotaxis
- Staphylococcal complement inhibitor (SCIN) - inhibits complement
- Biofilm-associated protein (Bap) - promotes biofilm colonization
This allows a growing, deepening abscess to develop that "comes to a head" by thinning and rupturing the overlying skin.
Clinical Features
Progression:
- Starts as a painful, indurated, tender swelling with surrounding oedema
- After a few days, central softening occurs - a small pustule appears at the summit
- May rupture spontaneously, discharging greenish slough
- A deep cavity lined by granulation tissue develops, which heals on its own
Complications specific to axillary furuncles:
-
Hidradenitis suppurativa - recurrent furuncles in the axilla can progress to this chronic, relapsing inflammatory condition affecting apocrine glands
-
Cellulitis - especially in immunocompromised patients
-
Lymphadenitis - regional lymph node infection
-
Infection spreading to neighboring hair follicles, leading to carbuncle formation
-
S Das Manual on Clinical Surgery, p. 51
Furuncle vs Carbuncle - Key Distinction
| Feature | Furuncle | Carbuncle |
|---|---|---|
| Follicles involved | Single | Multiple (collection) |
| Depth | Skin + subcutaneous tissue | Deeper, spreads under fascia |
| Sinuses | None initially | Multiple sinuses (cribriform/"sieve-like" appearance) |
| Typical patient | Any age | Men >40, often diabetic |
| Common site | Axilla, face, neck | Nape of neck, upper back |
| Systemic symptoms | Usually mild | More prominent toxaemia |
Management
Conservative (early/non-fluctuant)
- Warm compresses - promotes localization and spontaneous pointing
- Antibiotics are indicated when:
- Lesion is not yet fluctuant
- Surrounding cellulitis or lymphadenitis is present
- Lesion is on the face (danger triangle)
- Immunocompromised patient (diabetes, HIV, steroids)
Definitive - Incision and Drainage (I&D)
- Treatment of choice once fluctuance is established
- When done properly, antibiotics are usually unnecessary post-procedure
- Procedure: linear incision over the pointing area, break up loculations with a hemostat, irrigate the cavity, pack with gauze
Antibiotic Choice
-
Community-acquired S. aureus: clindamycin, trimethoprim/sulfamethoxazole, or doxycycline
-
If MRSA is suspected (recurrent abscess, treatment failure): obtain culture and sensitivity; empirical coverage with TMP-SMX or doxycycline
-
MRSA is now the most common pathogen for skin/soft tissue infections presenting to the emergency department
-
Pfenninger and Fowler's Procedures for Primary Care, p. 1039-1051
-
Textbook of Family Medicine 9e, p. 937
Special Considerations in the Axilla
- Recurrent axillary furuncles should raise suspicion for hidradenitis suppurativa (HS) - a distinct chronic condition requiring a different management approach (dermatology referral, biologics like adalimumab may be needed).
- Rule out cold abscess (tuberculous origin) - non-tender, non-inflammatory, fluctuant swelling, more common in immunocompromised individuals; the axilla is one of its common sites.
- Check for predisposing systemic conditions: diabetes mellitus, obesity, HIV, or chronic steroid use in any patient with recurrent boils.
- Decolonization with mupirocin nasal ointment and chlorhexidine body washes may reduce recurrence if the patient is a nasal carrier of S. aureus.
Bottom line: An axillary furuncle is a S. aureus hair follicle abscess managed with warm compresses if pre-fluctuant, or incision and drainage once fluctuant. Antibiotics covering MRSA (TMP-SMX, doxycycline) are added for cellulitis, systemic signs, or immunocompromised patients. Recurrent axillary furuncles should prompt evaluation for hidradenitis suppurativa and underlying systemic predisposition.
Furuncle on toe
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information. Here is the full clinical answer:
Furuncle (Boil) on the Toe
Important Anatomical Note
A "furuncle on the toe" is an uncommon but clinically important presentation. True furuncles require hair follicles - and while the dorsum of the toes has sparse hair, the toe is mostly glabrous (hairless) skin. This means what presents as a "furuncle on the toe" often overlaps with or mimics other distinct infections. Understanding these distinctions is essential for correct management.
Can a True Furuncle Occur on the Toe?
Yes, but only on the dorsal surface where sparse hair follicles exist. The pathophysiology is identical to furuncles elsewhere:
- Causative organism: Staphylococcus aureus (including CA-MRSA)
- Mechanism: Hair follicle blockage → perifolliculitis → deep suppurative abscess
- Natural history: Hard, tender, red folliculocentric nodule → enlarges → fluctuant → ruptures with discharge of pus and necrotic core → heals by granulation
Furuncles typically arise in hair-bearing sites subject to friction, occlusion, and perspiration - the toe (particularly with tight footwear and sweating) can satisfy these conditions.
- Fitzpatrick's Dermatology, p. 2754
Key Differential Diagnoses on the Toe
Toe swellings that resemble furuncles must be carefully distinguished:
1. Paronychia (most common mimic)
Infection of the nail fold, not the hair follicle.

| Feature | Paronychia | True Furuncle |
|---|---|---|
| Location | Nail fold (lateral/posterior) | Hair-bearing dorsal skin |
| Causative organisms | S. aureus, Streptococci, anaerobes, Candida | S. aureus (primarily) |
| Associated with | Nail trauma, ingrown toenail, water exposure | Friction, folliculitis, occlusion |
| Spread | Can track under nail (subungual) | Spreads into subcutaneous tissue |
Paronychia stages (per Roberts & Hedges' Clinical Procedures in Emergency):
-
Early: Collection limited to the lateral nail fold
-
Advanced: Abscess spreads around nail base, lifts the eponychium
-
Severe: Subungual extension + cellulitis up the digit - requires nail removal and IV antibiotics
-
Roberts and Hedges' Clinical Procedures in Emergency Medicine, p. 889
2. Felon
An abscess in the pulp space of the distal phalanx (plantar/volar side of the toe tip). Caused by S. aureus or streptococci. Extremely painful because the fibrous septa of the pulp space create a closed compartment with no room for swelling. Requires urgent I&D to prevent compartment syndrome and osteomyelitis.
3. Diabetic Foot Abscess
In diabetic patients with sensory neuropathy, a foreign body (e.g., a sewing needle, thorn, splinter) may penetrate the sole unnoticed and cause a deep abscess masquerading as a furuncle. Always radiograph the foot in diabetics with a toe/foot abscess.
A large painful abscess on the heel of a diabetic patient improved clinically but pain persisted - X-ray revealed a broken-off sewing needle. The patient had sensory neuropathy and was unaware of having stepped on it. - Fitzpatrick's Dermatology, p. 2754
Predisposing Factors (Systemic)
Recurrent or poorly healing toe furuncles/abscesses should prompt evaluation for:
-
Diabetes mellitus (impaired neutrophil function, poor vascularity)
-
Obesity (increased friction, sweating in web spaces)
-
Immunosuppression (HIV, steroids, chemotherapy)
-
Blood dyscrasias or defects in neutrophil function
-
S. aureus nasal carriage (self-inoculation)
-
Fitzpatrick's Dermatology, p. 2754; Sherris & Ryan's Medical Microbiology, p. 979
Management
Step 1: Assess Fluctuance
- Non-fluctuant (early): Warm soaks, elevation, oral antistaphylococcal antibiotics
- Fluctuant (pus-filled cavity): Incision and Drainage (I&D) is the definitive treatment
Step 2: Incision and Drainage
- Digital/toe block with local anaesthetic first
- Linear incision over the pointing area
- Break up loculations
- Irrigate with saline
- Pack with gauze; remove packing at 24-48 hours
- When done correctly, systemic antibiotics are often unnecessary post-procedure
Step 3: Antibiotic Selection
| Scenario | Antibiotic |
|---|---|
| Surrounding cellulitis present | Add oral antistaphylococcal antibiotic |
| MRSA suspected (recurrence, treatment failure) | TMP-SMX or doxycycline; confirm with culture |
| Immunocompromised / diabetic | Broader cover; consider IV antibiotics |
| Paronychia with oral flora (anaerobes likely) | Amoxicillin-clavulanate or clindamycin |
- Roberts and Hedges' Clinical Procedures in Emergency Medicine (Table 57.1)
Step 4: Culture
Send a swab of pus in all toe abscesses, immunocompromised patients, and any recurrent case - given the rising prevalence of CA-MRSA.
Red Flags - When to Escalate
- Rapidly spreading cellulitis or lymphangitis (red streaking up the foot/leg)
- Systemic fever, rigors, or sepsis signs
- Osteomyelitis risk (deep infection, bone tenderness, diabetic patient, sinus tract)
- No improvement after 48 hours of antibiotics + drainage
- Abscess tracking under the nail requiring nail avulsion
- Suspected necrotizing fasciitis (disproportionate pain, skin discolouration, crepitus)
In diabetic patients, a toe abscess that does not respond promptly warrants urgent surgical review - what looks like a simple boil can be the tip of a deep-space infection threatening limb loss.
Bottom line: A toe furuncle is a S. aureus hair-follicle abscess on the dorsum of the toe, managed with warm soaks if pre-fluctuant or I&D once fluctuant. On the toe specifically, always rule out paronychia (nail fold), felon (pulp space), and - in diabetics - a foreign body abscess. MRSA should be suspected in recurrent or treatment-resistant cases, and any diabetic patient with a toe abscess deserves extra vigilance for deep-space infection or osteomyelitis.
This is a shared conversation. Sign in to Orris to start your own chat.