Congestive heart failure
Reading File
search_medical_text
congestive heart failure pathophysiology etiology classification
search_medical_text
heart failure diagnosis management treatment guidelines
search_medical_image
congestive heart failure chest X-ray pulmonary edema cardiomegaly
GradeResponse
GradeResponse
GradeResponse
Congestive Heart Failure (CHF)
Definition
Congestive heart failure (CHF) is a clinical syndrome — not a single disease — characterized by current or prior symptoms and/or signs caused by a structural and/or functional cardiac abnormality. It is corroborated by elevated natriuretic peptides (BNP/NT-proBNP) and/or objective evidence of cardiogenic pulmonary or systemic congestion on imaging or invasive hemodynamic measurements. (ESC Guidelines – Diagnosis and Treatment of Acute and Chronic Heart Failure, p. 5)
Classification by Ejection Fraction
| Category | EF | Key Feature |
|---|---|---|
| HFrEF (Heart failure with reduced EF) | < 40% | Systolic dysfunction; LV dilated and weak |
| HFmrEF (mildly reduced EF) | 40–49% | Borderline; often ischemic etiology |
| HFpEF (preserved EF) | ≥ 50% | Diastolic dysfunction; stiff LV |
NYHA Functional Classification:
- Class I — No symptoms with ordinary activity
- Class II — Mild symptoms; slight limitation with ordinary activity
- Class III — Marked limitation; comfortable only at rest
- Class IV — Symptoms at rest; unable to perform any activity without discomfort
Etiology
Most common causes:
- Coronary artery disease / ischemic cardiomyopathy (most frequent in the West)
- Hypertension → hypertensive cardiomyopathy
- Dilated cardiomyopathy (idiopathic, viral, alcoholic, peripartum)
- Valvular heart disease (mitral/aortic stenosis or regurgitation)
- Diabetes mellitus (diabetic cardiomyopathy)
- Arrhythmias (e.g., atrial fibrillation-induced tachycardiomyopathy)
Less common:
- Infiltrative diseases (amyloidosis, sarcoidosis, hemochromatosis)
- Thyroid disease, high-output states (severe anemia, AV fistula, beriberi)
- Cardiotoxins (anthracyclines, trastuzumab, alcohol, cocaine)
Pathophysiology
- Primary insult (e.g., MI, pressure overload) → reduced cardiac output
- Compensatory mechanisms activated:
- Neurohormonal: RAAS activation → Na/water retention, vasoconstriction
- Sympathetic nervous system activation → tachycardia, increased contractility
- Ventricular remodeling → hypertrophy or dilation
- Decompensation: Chronic neurohormonal activation becomes maladaptive → progressive myocyte loss, fibrosis, further chamber dilation
- Congestion: Elevated filling pressures → pulmonary congestion (left-sided) and/or systemic venous congestion (right-sided)
Clinical Presentation
Left-sided HF (pulmonary congestion):
- Dyspnea on exertion → orthopnea → paroxysmal nocturnal dyspnea (PND)
- Pulmonary crackles (rales), S3 gallop
- Frothy or pink-tinged sputum in acute pulmonary edema
Right-sided HF (systemic congestion):
- Peripheral pitting edema (bilateral, dependent)
- Jugular venous distension (JVD)
- Hepatomegaly, ascites
- Anorexia/nausea (gut edema)
General:
- Fatigue, exercise intolerance
- Cardiac cachexia (late stage)
- Cheyne-Stokes respirations (severe HF)
Diagnosis
Key Investigations
| Test | Finding |
|---|---|
| BNP / NT-proBNP | Elevated; primary biomarker for HF diagnosis |
| ECG | LVH, Q waves (prior MI), bundle branch block, arrhythmia |
| Echocardiography | Gold standard: measures EF, wall motion, valve function, filling pressures |
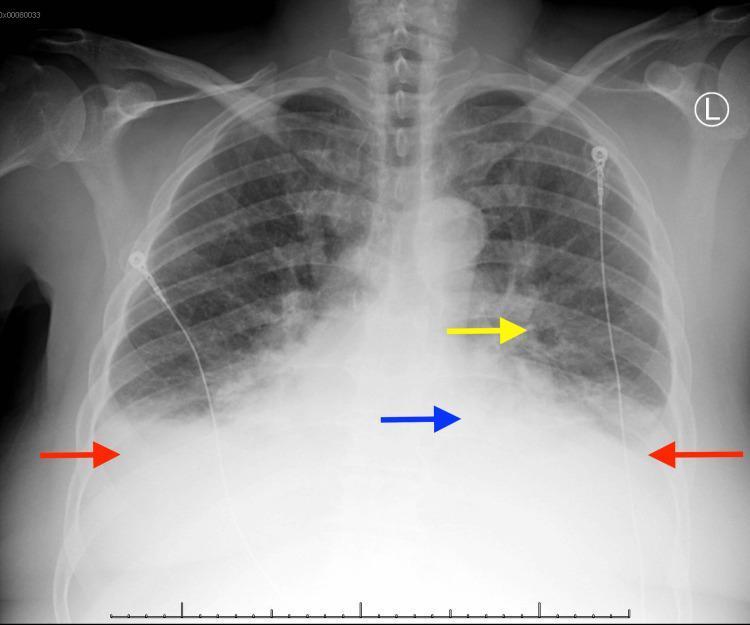
| Chest X-ray | Cardiomegaly, pulmonary vascular congestion, Kerley B lines, pleural effusions |
| Labs | CBC, BMP (renal function, electrolytes), LFTs, TFTs, ferritin, iron studies |
| Coronary angiography | If ischemic etiology suspected |
Chest X-ray Findings in CHF
Classic radiographic findings include cardiomegaly, bilateral pleural effusions, pulmonary vascular congestion, and alveolar (bat-wing) pulmonary edema:
Management
Acute Decompensated HF
| Intervention | Details |
|---|---|
| Positioning | Sit upright; legs dependent |
| Oxygen/NIV | Supplemental O₂; CPAP/BiPAP for pulmonary edema |
| IV Diuretics | Furosemide (loop diuretic) — cornerstone of decongestion |
| Vasodilators | IV nitroglycerin or nitroprusside if BP allows |
| Inotropes | Dobutamine, milrinone for cardiogenic shock |
| Vasopressors | Norepinephrine if hypotensive shock |
Chronic HFrEF — Guideline-Directed Medical Therapy (GDMT)
The 2023 ESC Focused Update reinforces a "four pillars" approach for HFrEF (all with mortality benefit):
| Pillar | Drug Class | Example Agent |
|---|---|---|
| 1 | ACE inhibitor / ARB / ARNi | Sacubitril/valsartan (preferred over ACEi) |
| 2 | Beta-blocker | Carvedilol, bisoprolol, metoprolol succinate |
| 3 | MRA (mineralocorticoid receptor antagonist) | Spironolactone, eplerenone |
| 4 | SGLT2 inhibitor | Dapagliflozin, empagliflozin |
Additional therapies:
- Loop diuretics (furosemide) for symptom relief and decongestion
- Ivabradine (if HR ≥ 70 bpm on max beta-blocker, sinus rhythm)
- Hydralazine + isosorbide dinitrate (if ACEi/ARB/ARNi not tolerated, particularly in Black patients)
- Iron replacement (IV ferric carboxymaltose) if iron-deficient
HFpEF
- SGLT2 inhibitors (dapagliflozin, empagliflozin) — now recommended; reduce HF hospitalizations
- Diuretics for volume/symptom control
- Aggressive management of underlying comorbidities (HTN, DM, AF, obesity)
Device Therapy
| Device | Indication |
|---|---|
| ICD (implantable cardioverter-defibrillator) | EF ≤ 35% despite GDMT ≥ 3 months; NYHA II–III; ≥ 1 year survival expected |
| CRT (cardiac resynchronization therapy) | EF ≤ 35% + LBBB + QRS ≥ 150 ms; NYHA II–IV |
| CRT-D | Combines CRT + ICD |
| LVAD | Bridge to transplant or destination therapy in advanced HF |
| Heart transplantation | End-stage HF; NYHA III–IV refractory to all therapy |
Complications
- Sudden cardiac death (ventricular arrhythmias)
- Cardiogenic shock
- Renal failure (cardiorenal syndrome)
- Hepatic congestion / cardiac cirrhosis
- Pulmonary hypertension
- Thromboembolic events (stroke, DVT/PE) — especially in AF
- Malnutrition / cardiac cachexia
Prognosis
- 5-year mortality ~50% overall; worse than many cancers
- HFrEF mortality has improved substantially with GDMT (especially the addition of SGLT2i and ARNi)
- Poor prognostic markers: low EF, elevated BNP, renal dysfunction, hyponatremia, NYHA Class IV, recurrent hospitalizations
- HFpEF prognosis approaches HFrEF in severity but fewer proven therapies exist
Sources: ESC 2023 Focused Update – Diagnosis and Treatment of Acute and Chronic Heart Failure (p. 5); ESC Guidelines – Management of Cardiovascular Disease in Patients with Diabetes (p. 44); clinical imaging from PMC Clinical VQA dataset.
This is a shared conversation. Sign in to Orris to start your own chat.