Acute inflammation of the middle ear. Mastoiditis. Chronic inflammation of the middle ear (mesotympanitis, epitympanitis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Here is the full structured summary:
Inflammatory Diseases of the Middle Ear
I. Acute Otitis Media (AOM)
Definition & Epidemiology
Acute otitis media is characterized by the presence of a middle ear effusion combined with signs and symptoms of acute infection. It is one of the most common diseases of childhood — the acute bacterial infection of the middle ear occurs in 80% of children between ages 1 and 6 years, and is the primary driver of pediatric antibiotic use in the outpatient setting. Peak incidence is 6–15 months of age. AOM is less common in adults, though the diagnostic and treatment approach is similar. — Cummings Otolaryngology, p. 2682; Rosen's Emergency Medicine
Pathophysiology
The eustachian tube lies between the middle ear cavity and nasopharynx, serving three functions: ventilating the middle ear to equalize pressure, allowing drainage, and protecting against nasopharyngeal secretion reflux. Mechanical or functional obstruction — most commonly from upper respiratory inflammation — leads to negative middle ear pressure, fluid accumulation, and bacterial colonization from the nasopharynx, causing inflammation and the signs/symptoms of AOM. AOM is commonly a co-infection of viral and bacterial pathogens; viruses are isolated in middle ear aspirates in 70% of cases. — Rosen's Emergency Medicine
Risk factors: Male sex, non-Hispanic white race, daycare attendance, family history, parental smoking, pacifier/bottle use. Breastfeeding is protective. Children with cleft palate or Down syndrome have higher rates due to eustachian tube abnormalities.
Microbiology
- Most common: Streptococcus pneumoniae, Haemophilus influenzae (primarily non-typeable), Moraxella catarrhalis
- Widespread pneumococcal vaccination has increased the relative frequency of H. influenzae, especially in persistent AOM and treatment failures
- Less common: S. pyogenes, S. aureus, Mycobacterium tuberculosis, Chlamydia trachomatis, gram-negative species
Clinical Features
- Ear pain (otalgia), fever, tympanic membrane (TM) erythema, bulging, and decreased mobility
- Bullae on the TM = bullous myringitis — treatment does not differ from non-bullous AOM
- Otorrhea from an acute perforation: treat identically to AOM without perforation; perforations are typically small and resolve spontaneously
- Diagnosis is clinical: middle ear effusion + signs of acute infection
Management
Observation vs. antibiotics:
Most cases of AOM resolve spontaneously. A 2–3 day observation period may be offered in appropriately selected pediatric patients. Observation is not validated in adults — antibiotics are first-line for adults.
| Age | Scenario | Recommendation |
|---|---|---|
| 6 months – 2 years | Any presentation | Antibiotics |
| ≥ 2 years | Severe symptoms or bilateral AOM | Antibiotics |
| ≥ 2 years | Unilateral AOM, no otorrhea | Antibiotics or observation |
Antibiotic therapy:
- First-line: Amoxicillin 80–90 mg/kg/day in two divided doses (effective against susceptible and intermediately resistant S. pneumoniae)
- Penicillin allergy (non-severe): Cefdinir, cefuroxime, cefpodoxime, or ceftriaxone IM/IV for 3 days
- Tympanostomy tubes with acute otorrhea: Ototopical fluoroquinolone drops
- Antibiotics do not improve pain in the first 24 hours — acetaminophen or ibuprofen should be used for analgesia
- Recurrent episodes or treatment failures warrant alternate antibiotic selection
— Rosen's Emergency Medicine; Cummings Otolaryngology
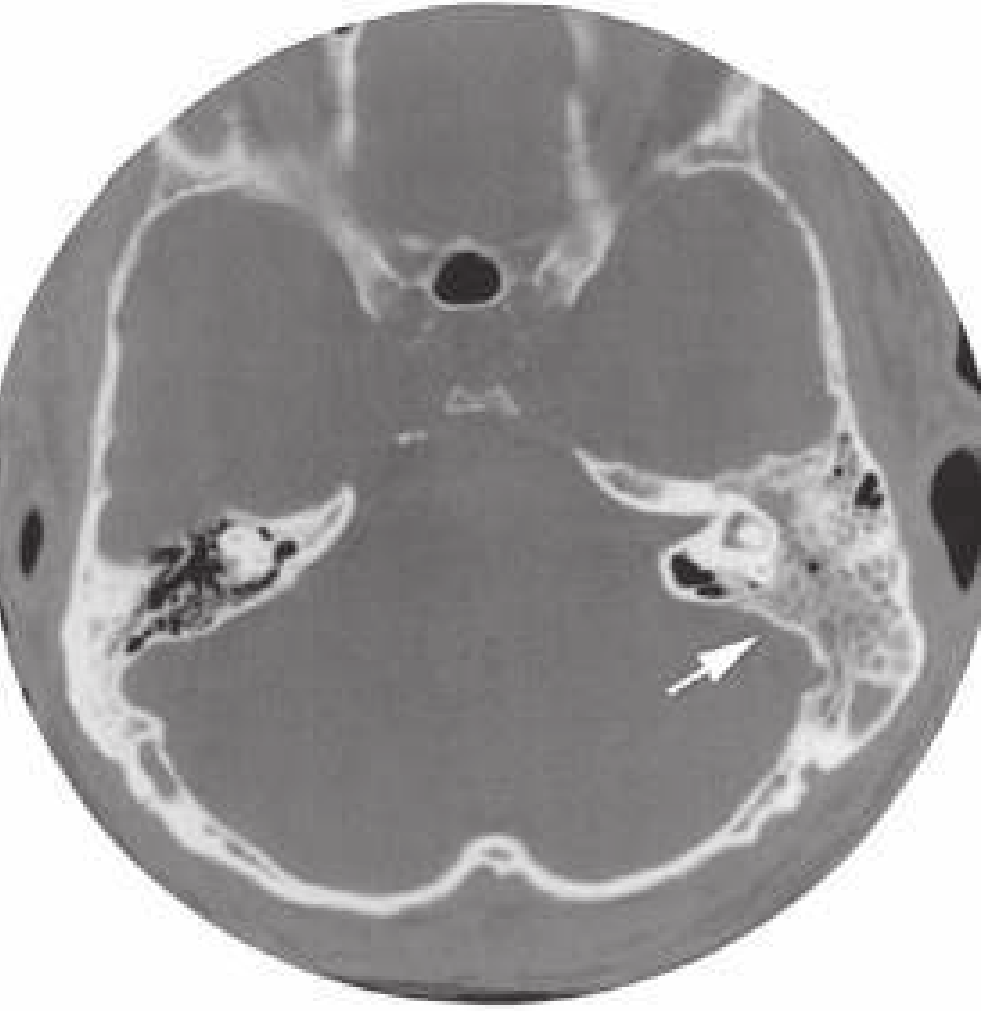
II. Mastoiditis
Pathophysiology
Mastoiditis is the most common suppurative complication of otitis media, though it is rare in the modern era. The middle ear and mastoid air cells are connected by the aditus ad antrum. When this narrow connection becomes obstructed, a closed space forms with potential for abscess development and bone destruction. Infection may spread from the mastoid air cells via venous channels, inflaming the overlying periosteum. Progression leads to destruction of the mastoid bone trabeculae and coalescence of cells → acute mastoid osteitis (coalescent mastoiditis). — Rosen's Emergency Medicine
Acute mastoiditis may also occur as a complication of leukemia, mononucleosis, sarcoma of the temporal bone, Kawasaki disease, and cochlear implant placement.
Microbiology
- S. pneumoniae — remains the leading cause
- Group A streptococcus — common
- Emerging pathogens (particularly post-antibiotic therapy): P. aeruginosa, S. aureus, Fusobacterium necrophorum
Clinical Features
- Fever, headache, otalgia, postauricular erythema and tenderness
- Protrusion of the auricle (forward and downward displacement) — classic sign
- Abnormal TM (erythema, bulging, decreased mobility); TM may be normal in ~10% of cases
- Suspicion should be heightened if AOM symptoms have lasted > 2 weeks
Differential Diagnosis
Severe otitis media, otitis externa, skull fracture, posterior auricular lymphadenopathy/lymphadenitis, deep space neck infections.
Imaging
CT scan is indicated when:
- Neurologic symptoms suggest intracranial extension
- There is failure to improve with conservative therapy
Management
- Parenteral antibiotics are the cornerstone of treatment; initiated promptly on clinical diagnosis
- Mastoidectomy may be required for coalescent mastoiditis, abscess formation, or failure to respond to antibiotics
- Intracranial complications (epidural abscess, subdural empyema, meningitis, sigmoid sinus thrombosis) require urgent surgical drainage
— Rosen's Emergency Medicine; Cummings Otolaryngology
III. Chronic Otitis Media
Chronic otitis media refers to prolonged discharge from the ear through a perforation of the tympanic membrane. It is divided clinically into two major forms based on the location of the pathology.
A. Mesotympanitis (Tubotympanic / Safe Chronic Otitis Media)
Definition: Chronic inflammation of the mesotympanum (central portion of the middle ear), associated with a central perforation of the pars tensa. Eustachian tube dysfunction plays a central role.
Features:
- Central TM perforation — the rim of the perforation remains attached to the annulus; the tympanic membrane does not extend into the attic
- Mucoid or mucopurulent discharge
- Conductive hearing loss due to TM perforation ± ossicular involvement
- Generally considered "safe" — less risk of serious complications
- No cholesteatoma formation (in uncomplicated cases)
- Underlying pathology: persistent mucosal inflammation, tympanosclerosis (hyalinization of middle ear structures from chronic inflammation or trauma), and ossicular erosion or fixation
Management:
- Topical antibiotic drops (fluoroquinolone-containing preferred, especially if TM is perforated — aminoglycosides are contraindicated due to ototoxicity)
- Systemic antibiotics for exacerbations
- Tympanoplasty (surgical repair of the perforation) for definitive treatment and hearing restoration
B. Epitympanitis (Atticoantral / Dangerous Chronic Otitis Media)
Definition: Chronic inflammation of the epitympanum (attic) and mastoid, associated with a marginal or attic perforation of the pars flaccida. This form is associated with cholesteatoma.
Features:
- Marginal perforation in the posterior-superior TM or attic (pars flaccida)
- Often foul-smelling discharge (due to keratin debris and chronic infection)
- Conductive hearing loss, which may progress to sensorineural loss if the labyrinth is eroded
- Formation of cholesteatoma — an epidermal inclusion cyst of the middle ear or mastoid in which keratinizing squamous epithelium accumulates; it can only be eradicated by surgical resection
- Bone erosion is the hallmark: osteoclastic bone resorption is stimulated by inflammatory cytokines, localized pressure, keratin, and bacterial toxins — Cummings Otolaryngology, p. 2683
- Considered "dangerous" due to high risk of complications
Complications of epitympanitis/cholesteatoma:
- Labyrinthine fistula (horizontal canal fistula is most common)
- Facial nerve palsy
- Petrous apicitis (extension into the pneumatized anterior/posterior petrous apex)
- Intracranial infections: meningitis, epidural/subdural abscess, brain abscess
- Sigmoid sinus thrombosis
Cholesteatoma types:
- Primary acquired — arising from retraction pocket of pars flaccida (no prior perforation)
- Secondary acquired — keratinizing epithelium migrates through a pre-existing TM perforation into the middle ear
- Congenital — behind an intact TM, without prior infection or surgery
Management:
- Surgical: tympanomastoidectomy (canal wall up or canal wall down mastoidectomy)
- Objective: complete eradication of cholesteatoma and reconstruction of the sound-conduction mechanism
- Topical therapy alone is insufficient and potentially dangerous if it masks ongoing bone erosion
— Cummings Otolaryngology, pp. 2682–2689
Summary Comparison
| Feature | AOM | Mastoiditis | Mesotympanitis | Epitympanitis |
|---|---|---|---|---|
| Onset | Acute | Acute (complication) | Chronic | Chronic |
| TM finding | Bulging, erythema | Abnormal (as AOM) | Central perforation | Marginal/attic perforation |
| Discharge | ± otorrhea | ± otorrhea | Mucoid/mucopurulent | Foul-smelling, purulent |
| Cholesteatoma | No | No | No | Yes |
| Bone destruction | No | Mastoid trabecular lysis | Rare | Characteristic |
| Danger level | Moderate | High if untreated | "Safe" | "Dangerous" |
| Primary treatment | Antibiotics ± observation | IV antibiotics ± mastoidectomy | Topical antibiotics + tympanoplasty | Tympanomastoidectomy |
This is a shared conversation. Sign in to Orris to start your own chat.