Acute inflammation of the middle ear. Mastoiditis. Chronic inflammation of the middle ear (mesotympanitis. epitympanitis). Explain in detail
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from the textbooks. Let me compile this into a thorough, well-structured answer covering all four topics: AOM, mastoiditis, mesotympanitis, and epitympanitis.
Middle Ear Inflammation: A Detailed Overview
1. Acute Otitis Media (AOM)
Definition
Acute otitis media is acute bacterial or viral infection of the middle ear cleft, characterized by the presence of a middle ear effusion combined with signs and symptoms of acute infection (otalgia, fever, tympanic membrane changes).
Epidemiology
AOM is one of the most common childhood diseases — 80% of children experience at least one episode between ages 1 and 6. It is the most frequent diagnosis driving outpatient antibiotic prescriptions in the United States. Peak incidence is at 6–15 months. Risk factors include male sex, non-Hispanic white race, daycare attendance, family history, parental smoking, pacifier use, and anatomic anomalies (cleft palate, Down syndrome). Breastfeeding is protective. Pneumococcal vaccination has significantly reduced incidence.
Pathophysiology
The eustachian tube (ET) connects the middle ear to the nasopharynx and serves three functions: ventilation, drainage, and protection from refluxed secretions. In AOM, ET dysfunction — from viral URI-induced mucosal edema or anatomic reasons — causes negative pressure and fluid accumulation in the middle ear. Bacteria and viruses from the nasopharynx colonize this fluid, triggering an inflammatory cascade with increased pressure, edema, and purulent exudate.
AOM is frequently a co-infection: viruses are isolated from middle ear aspirates in ~70% of cases. Key bacterial pathogens:
- Streptococcus pneumoniae — most common, most virulent
- Haemophilus influenzae (non-typeable) — increased frequency since PCV vaccine
- Moraxella catarrhalis — common but often self-limiting
- In neonates: Group B Streptococcus, S. aureus, gram-negatives also possible
Clinical Features
- Otalgia (most important symptom) — may present as ear-pulling in infants
- Fever, irritability, poor feeding, vomiting
- Otoscopy: erythema and bulging of the tympanic membrane (TM), reduced or absent mobility on pneumatic otoscopy, possible perforation with purulent discharge
- Bullous myringitis — hemorrhagic bullae on TM surface, seen in some cases; treatment is the same as non-bullous AOM
- Hearing loss (conductive) due to effusion
Diagnosis requires both a middle ear effusion and signs of acute inflammation — erythema alone is insufficient.
Management
Watchful waiting (observation): Appropriate for:
- Children ≥2 years with mild, unilateral AOM
- Children 6–24 months with mild bilateral AOM
- Observation for 48–72 hours; prescribe antibiotics if no improvement
Antibiotic therapy:
- Amoxicillin (high-dose: 80–90 mg/kg/day) — first-line for most patients
- Amoxicillin-clavulanate — treatment failure after 48–72 h, or if H. influenzae suspected
- Cephalosporins (cefdinir, cefuroxime) — penicillin allergy (non-anaphylactic)
- Azithromycin — severe penicillin allergy; course 1–5 days
- Ceftriaxone IM — vomiting or non-compliance
Pain management: Antibiotics do not relieve pain in first 24 hours — use paracetamol or ibuprofen. Topical benzocaine drops provide short-term relief.
Myringotomy + tympanostomy tubes: Indicated for recurrent AOM (≥3 episodes in 6 months or ≥4 in 1 year) or persistent OME with hearing loss.
Complications: Persistent otitis media with effusion (OME), TM perforation, acute mastoiditis, facial nerve palsy, labyrinthitis, intracranial extension.
2. Mastoiditis
Definition & Pathophysiology
Mastoiditis is the most common suppurative complication of AOM, though its incidence has fallen dramatically in the antibiotic era. It is fundamentally an extension of middle ear infection into the mastoid air cells, which communicate with the middle ear via the aditus ad antrum.
The pathological progression:
- Acute mastoiditis with periostitis — mucosal inflammation of mastoid air cells with accumulation of pus; the bony trabeculae remain intact
- Coalescent (acute mastoid osteitis) — sustained pressure and inflammatory enzymes destroy bony trabeculae separating air cells; cells coalesce into an abscess cavity
- Masked mastoiditis — partially treated AOM where symptoms are suppressed but low-grade infection persists
Obstruction of the aditus creates a closed-space infection. Spread occurs via:
- Erosion of the mastoid cortex → subperiosteal abscess (most common)
- Medial spread → petrous apicitis
- Posterior spread → sigmoid sinus thrombosis
- Superior spread → epidural abscess, meningitis, brain abscess
Microbiology
- S. pneumoniae — most common
- Group A Streptococcus — significant cause
- Pseudomonas aeruginosa, S. aureus, Fusobacterium necrophorum — emerging pathogens, particularly post-antibiotic treatment
- Mixed infections possible in chronic cases
Clinical Features
- Postauricular pain, erythema, and tenderness — cardinal findings
- Protrusion (anterior displacement) of the auricle — ear pushed forward and downward by subperiosteal abscess
- Effacement of the postauricular crease
- Fever, headache, otalgia
- TM similar to AOM (erythematous, bulging, reduced mobility) — but may be normal in ~10%
- Suspicion should heighten if AOM symptoms persist beyond 2 weeks
Diagnosis
Clinical diagnosis in typical cases. CT scan is indicated when:
- Neurologic symptoms suggest intracranial extension
- Failure to improve after 24–48 h of IV antibiotics
- To assess extent of bone destruction and subperiosteal abscess
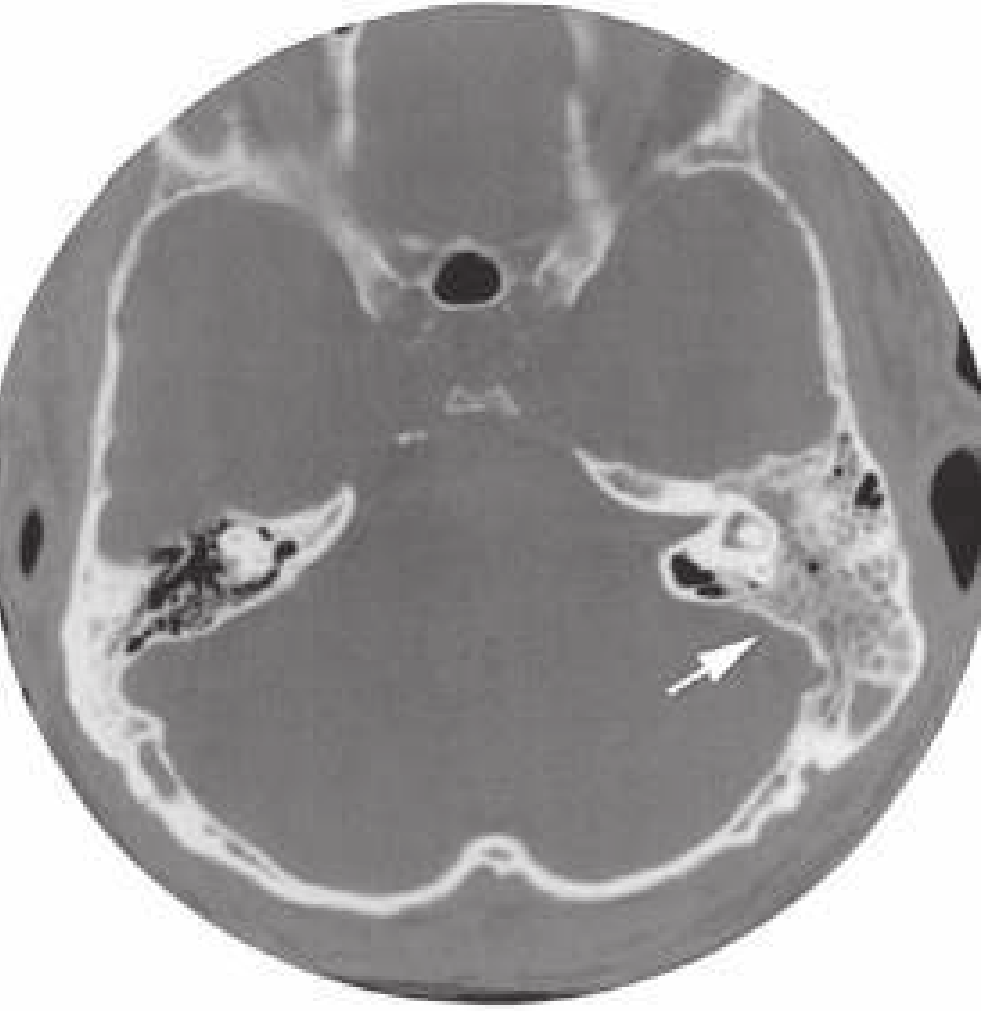
CT findings: soft-tissue density filling air cells, destruction of mastoid trabeculae, subperiosteal fluid collection.
Differential diagnosis: severe AOM, external otitis, auricular cellulitis, posterior auricular lymphadenitis, parotitis, skull fracture.
Management
Hospitalization is generally required for IV antibiotics and otolaryngologic consultation.
Antibiotics (parenteral):
- No recent antibiotic use: vancomycin 15 mg/kg IV (covers S. pneumoniae, S. pyogenes, MRSA)
- Recent antibiotic use or recurrent AOM: add cefepime 50 mg/kg IV (peds) / 2 g IV (adults) for Pseudomonas coverage
Surgical options (range by severity):
- Myringotomy ± tympanostomy tube placement — drainage, culture, pressure relief
- Cortical mastoidectomy — indicated for coalescent mastoiditis, subperiosteal abscess, or failure of medical therapy; removes diseased air cells while preserving ear canal wall
- Radical mastoidectomy — for extensive disease or intracranial complications
Complications of mastoiditis (if untreated):
- Subperiosteal abscess
- Bezold's abscess — pus tracks under sternocleidomastoid along the tip of mastoid
- Luc's abscess — pus in temporal/zygomatic region
- Petrous apicitis (Gradenigo's syndrome: otorrhea, abducens palsy, retro-orbital pain)
- Sigmoid sinus thrombosis
- Meningitis, epidural/subdural abscess, brain abscess
- Labyrinthitis, facial nerve paralysis
3. Chronic Otitis Media — Mesotympanitis (Tubotympanic / Safe Type)
Definition
Mesotympanitis (also called chronic tubotympanic otitis media or "safe" chronic otitis media) is a chronic inflammatory condition of the middle ear characterized by a permanent central perforation of the tympanic membrane with recurrent or persistent mucopurulent otorrhea, involving primarily the mesotympanum (the part of the middle ear medial to the pars tensa). It is considered "safe" because it does not typically erode the ossicles aggressively or invade the mastoid.
Pathogenesis
- Follows recurrent AOM, acute perforations that fail to heal, or pressure-related TM necrosis
- The perforation disrupts the barrier between the external canal and middle ear
- Repeated infections from external contamination (water entry) perpetuate mucosal inflammation
- Long-standing disease → mucosal hypertrophy, granulation tissue, polypoid change, tympanosclerosis
- Eustachian tube dysfunction contributes to inadequate ventilation and drainage
The perforation is central (pars tensa) — the remnant of the annulus is intact. This distinguishes it from marginal perforations (associated with epitympanitis/cholesteatoma).
Clinical Features
- Chronic, recurrent, non-foul-smelling mucoid/mucopurulent otorrhea
- Conductive hearing loss (due to TM perforation and ossicular chain compromise)
- Usually painless between acute exacerbations
- Otoscopy: central TM perforation, often with pale, wet, or granulating margins
- Hearing tests: mild-to-moderate conductive loss (typically 20–40 dB)
- Tuning fork: Rinne negative (BC > AC), Weber lateralizes to affected ear
Complications
- Ossicular erosion (especially incus long process) → greater conductive loss
- Tympanosclerosis — hyalinization/calcification of middle ear structures causing ossicular fixation
- Adhesive otitis media
- Sensorineural hearing loss (toxins, labyrinthine window involvement)
- Progression to cholesteatoma (less common in mesotympanitis than epitympanitis)
Management
Medical (conservative):
- Aural toilet — suction/dry mopping of discharge
- Topical antibiotic drops: fluoroquinolone drops (ciprofloxacin/ofloxacin) are preferred — effective and safe if TM is perforated (aminoglycosides are ototoxic and contraindicated with TM perforation)
- Systemic antibiotics for acute exacerbations — guided by culture
- Avoidance of water contamination (earplugs during bathing/swimming)
Surgical:
- Myringoplasty / Tympanoplasty — closure of TM perforation using temporalis fascia or perichondrium graft; performed when infection is quiescent
- Ossiculoplasty — if ossicular chain erosion is present
- Aim: dry ear, hearing restoration, prevention of further complications
4. Chronic Otitis Media — Epitympanitis (Atticoantral / Unsafe Type)
Definition
Epitympanitis (also called chronic atticoantral otitis media or "unsafe" chronic otitis media) is a chronic middle ear infection involving the epitympanum (attic/Prussak's space) and often the posterior mesotympanum and mastoid antrum. It is called "unsafe" because it is almost always associated with a cholesteatoma — an epidermal inclusion cyst filled with desquamating keratin — which actively erodes bone and can lead to serious intracranial complications.
Pathogenesis & Cholesteatoma Formation
A cholesteatoma is not a true tumor but an accumulation of desquamating keratinizing squamous epithelium within the middle ear or mastoid.
Theories of formation:
- Invagination theory (most accepted) — Chronic ET dysfunction → sustained negative middle ear pressure → retraction of the pars flaccida (or pars tensa) into the attic → retraction pocket accumulates keratin → cholesteatoma develops
- Epithelial migration theory — Squamous epithelium migrates through a marginal perforation into the middle ear
- Squamous metaplasia theory — Middle ear mucosa undergoes metaplastic transformation to keratinizing epithelium
- Basal cell hyperplasia theory — Hyperproliferation of basal layer cells of the pars flaccida with invasion
Bone erosion mechanism: Cholesteatoma matrix stimulates multinucleate osteoclasts via inflammatory cytokines (IL-1, TNF-α), localized pressure, and bacterial toxins → progressive bony destruction of ossicles, tegmen, semicircular canals, and facial nerve canal.
The perforation in epitympanitis is marginal or attic (pars flaccida), not central.
Clinical Features
- Foul-smelling (fetid), scanty otorrhea — keratin debris and anaerobic infection produce characteristic offensive odor
- Conductive hearing loss — from ossicular chain erosion
- Attic/marginal perforation on otoscopy — often with a retraction pocket
- Whitish pearly mass visible in the attic or posterosuperior quadrant (cholesteatoma)
- Deep otalgia, sense of aural fullness
- The ear may appear "dry" between episodes but discharge recurs
Complications (why it is "unsafe")
Bone erosion is relentless and can affect:
- Ossicular chain — incus most frequently; severe conductive loss (40–60 dB)
- Facial nerve canal — facial nerve palsy (House-Brackmann grading)
- Semicircular canals / labyrinth — fistula → vertigo, sensorineural hearing loss
- Tegmen tympani — spread to epidural space → epidural abscess
- Sigmoid sinus — thrombophlebitis, septic emboli
- Meningitis, brain abscess — life-threatening
- Petrous apex → Gradenigo's syndrome (otorrhea + 6th nerve palsy + retro-orbital pain)
Diagnosis
- Otoscopy/otomicroscopy — the primary tool; identify marginal/attic perforation, cholesteatoma
- CT temporal bone — gold standard for surgical planning: shows extent of bone erosion, mastoid involvement, facial nerve canal integrity, tegmen erosion
- MRI with DWI (diffusion-weighted imaging) — distinguishes cholesteatoma (restricted diffusion) from other soft tissue and detects residual/recurrent disease post-op
Management
Cholesteatoma requires surgical eradication — it cannot be sterilized medically.
Goals: eradicate disease, prevent complications, reconstruct hearing when possible.
Conservative (temporizing only):
- Aural toilet and topical antibiotics to control infection before surgery
- Saline irrigation or removal of keratin debris in clinic to delay progression
Surgical approaches:
| Procedure | Description | When Used |
|---|---|---|
| Canal wall-up (closed) mastoidectomy | Removes mastoid disease, preserves posterior ear canal wall | Localized disease; good ET function; reliable patient for follow-up |
| Canal wall-down (open/radical) mastoidectomy | Removes canal wall — creates open mastoid cavity | Extensive disease; lateral canal fistula; poor ET function |
| Modified radical mastoidectomy | Exteriorizes mastoid while preserving middle ear remnants | Preserves some hearing |
| Attic cholesteatoma resection | Endaural approach for limited attic disease | Early/limited epitympanic cholesteatoma |
Canal wall-up: residual/recurrent disease rate 11–27%; requires second-look procedure or DWI MRI.
Canal wall-down: recurrent disease 2–10%; requires lifelong mastoid cavity cleanings.
Summary Comparison Table
| Feature | Mesotympanitis | Epitympanitis |
|---|---|---|
| Synonyms | Tubotympanic, "safe" COM | Atticoantral, "unsafe" COM |
| Perforation | Central (pars tensa) | Marginal / attic (pars flaccida) |
| Discharge | Mucoid/mucopurulent, odorless | Scanty, foul-smelling (fetid) |
| Cholesteatoma | Absent | Present (hallmark) |
| Bone erosion | Minimal | Extensive |
| Complications | Less severe | Life-threatening possible |
| Treatment | Medical ± tympanoplasty | Surgery (mastoidectomy) mandatory |
Sources:
- Cummings Otolaryngology Head and Neck Surgery (Chapter 140 — Complications and Sequelae of Otitis Media)
- Rosen's Emergency Medicine: Concepts and Clinical Practice (Chapter 58 — Otitis Media, Mastoiditis)
This is a shared conversation. Sign in to Orris to start your own chat.