11 year girl with short stature, xray wrist showed wrist widening
Reading File
Searching the Web
rickets short stature wrist widening xray child differential diagnosis
Finding Sources
Searching PubMed
rickets children diagnosis wrist widening
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
Finding Sources
I now have excellent content to give a comprehensive answer. Let me compile everything.
Rickets - 11-Year-Old Girl with Short Stature and Wrist Widening on X-ray
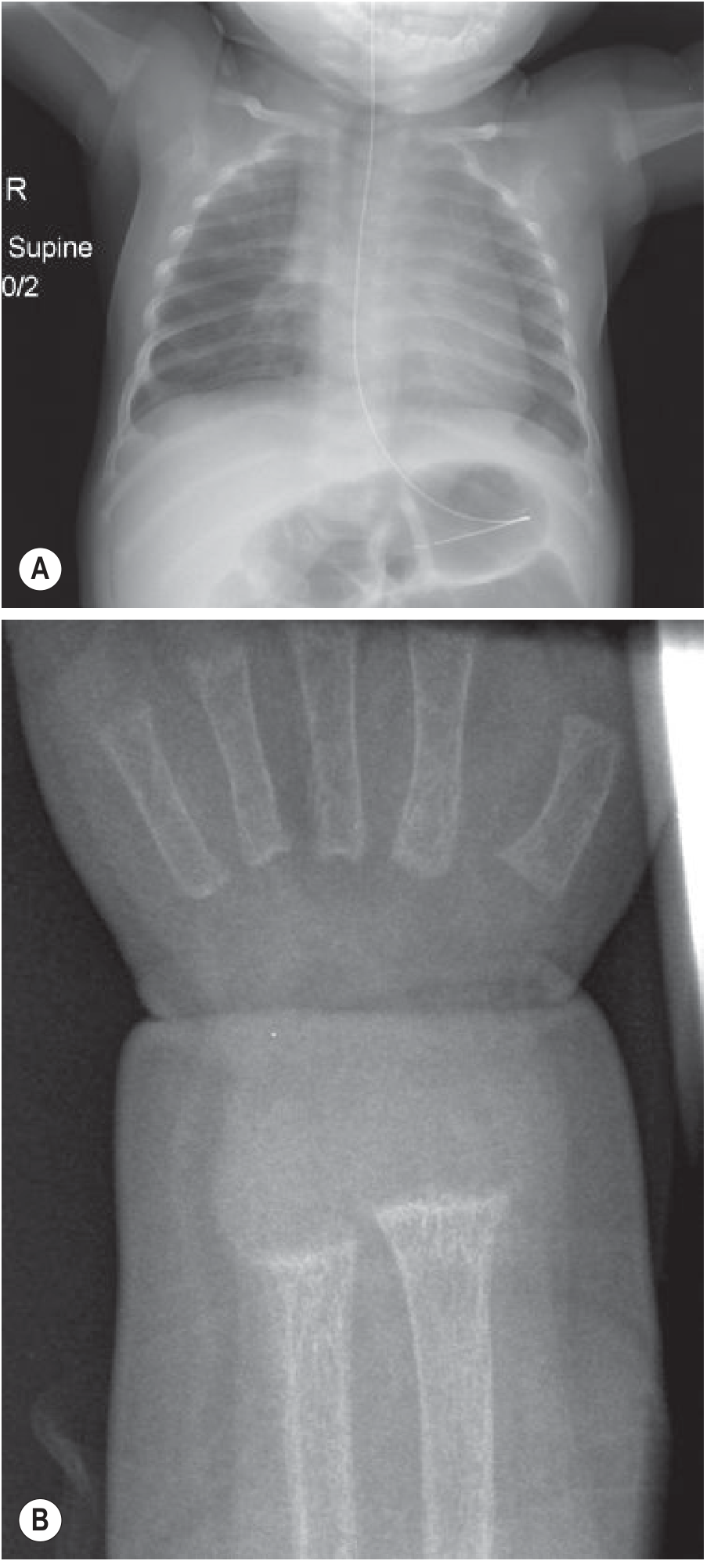
This is the classic presentation of rickets. The X-ray finding of wrist widening (metaphyseal flaring, cupping, and fraying at the distal radius and ulna) is pathognomonic.
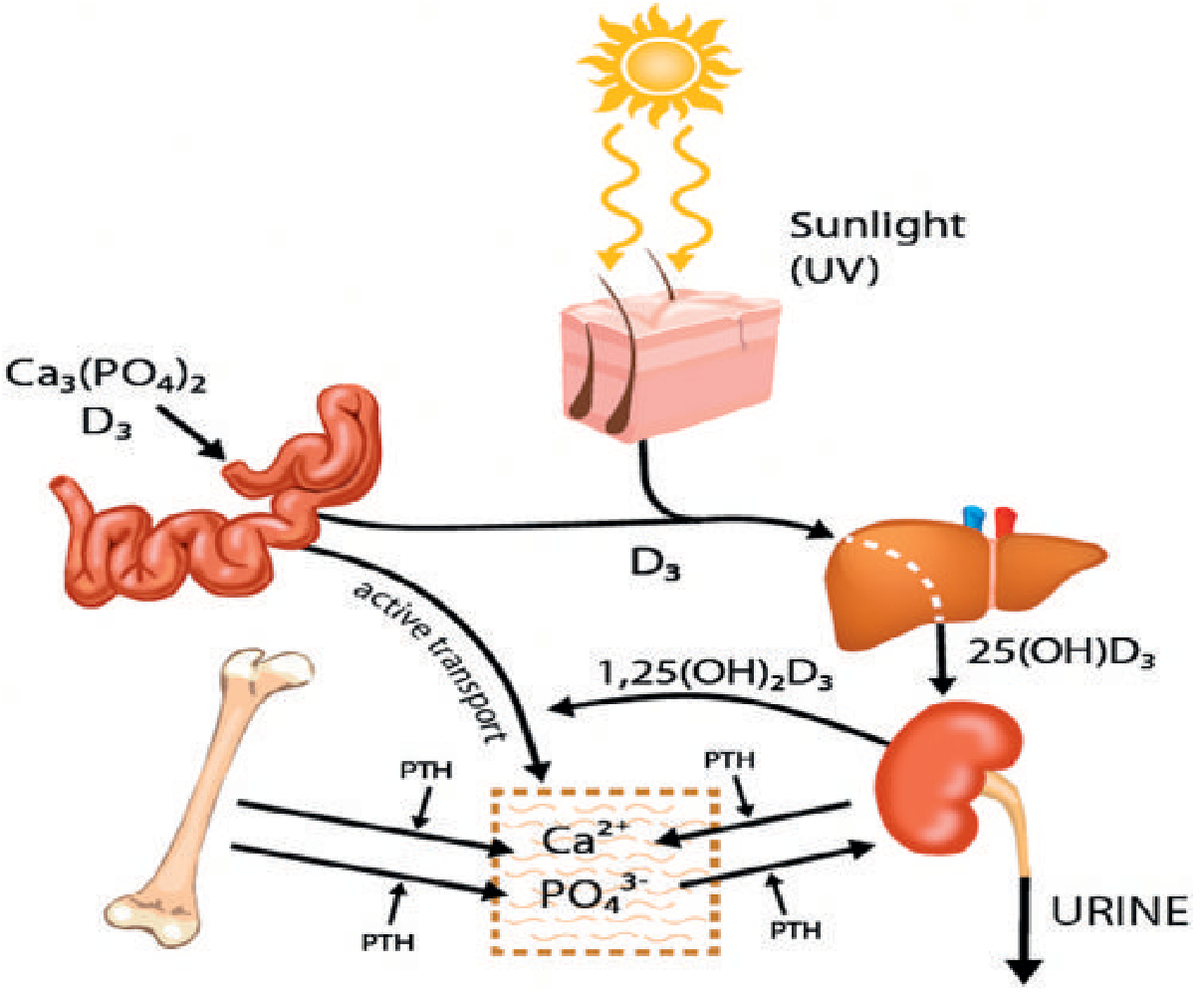
Pathophysiology
Rickets occurs when the calcium-phosphate product in the extracellular fluid is too low around developing growth plates. This disrupts the normal chondrocyte scaffold: instead of hypertrophied chondrocytes undergoing orderly apoptosis and mineralization, they accumulate in a disorganized, expanded, hypomineralized growth plate - producing the classic radiological findings.
X-ray Findings
The wrist and knee are the most commonly affected sites because they are the most rapidly growing physes in the body.
Classic radiological features:
- Widening of the growth plate (epiphysis-diaphysis distance increased)
- Metaphyseal fraying (loss of the zone of provisional calcification, giving a "paintbrush" or "frayed" appearance)
- Cupping of the metaphyses
- Generalized osteopenia (epiphyses appear indistinct)
- Looser zones (pseudofractures) - particularly at pubic rami, medial proximal femora, posterior proximal ulnae
- Bowing of long bones in advanced cases
- Rachitic rosary (expansion of costochondral junctions on chest X-ray)
Differential Diagnosis by Cause
| Type | Mechanism | Key Features |
|---|---|---|
| Nutritional Vit D deficiency | Inadequate dietary intake or sun exposure | Most common; low 25-OH Vit D; responds rapidly to supplementation; bowing less prominent |
| Vit D-dependent type 1 (VDDR1) | Deficient renal 1α-hydroxylase; AR | Presents <2 years; severe bony changes; hypocalcemic tetany/seizures; normal 25-OH Vit D but low 1,25-OH Vit D |
| Vit D-dependent type 2 (VDDR2) | Defective VDR; AR | <1 year presentation; alopecia; poor dentition |
| X-linked hypophosphatemic (XLH) | PHEX gene mutation; XLD; impaired renal PO4 reabsorption | Normal/elevated Vit D; isolated hypophosphatemia; severe bowing; short stature; dental abscesses; family history |
| Renal osteodystrophy | Chronic kidney disease; impaired 1α-hydroxylation | Signs of CKD; mixed picture |
| Fanconi syndrome | Proximal tubular defect; phosphate + glucose + amino acid wasting | Polyuria, polydipsia, growth failure |
| Dietary calcium deficiency | Low calcium intake despite normal Vit D | Common in some regions; high ALP, low Ca |
Clinical Features (in this case)
- Short stature (hallmark - growth plate disruption impairs longitudinal bone growth)
- Wrist/ankle widening
- Leg bowing (genu varum/valgum)
- Bone pain and tenderness
- Muscle weakness and hypotonia
- Rachitic rosary (beading at costochondral junctions)
- Dental abnormalities/delayed eruption
- Craniotabes (in infants)
Investigations to Order
First-line blood tests:
| Test | Nutritional Vit D deficiency | XLH (hypophosphatemic) |
|---|---|---|
| Serum calcium | Low or normal | Normal |
| Serum phosphate | Low (secondary) | Low (primary, isolated) |
| Alkaline phosphatase (ALP) | Markedly elevated | Elevated |
| PTH | Elevated (2° hyperparathyroidism) | Normal |
| 25-OH Vitamin D | Low (<20 ng/mL) | Normal |
| 1,25-OH Vitamin D | Low | Normal or elevated |
| Urinary calcium | Low | Low |
| Urinary phosphate | Elevated | Elevated (phosphate wasting) |
Radiology:
- Wrist X-ray (already done - shows widening)
- Knee X-ray
- Chest X-ray (rachitic rosary)
- Bone age (typically delayed)
Treatment (based on cause)
Nutritional Vit D deficiency:
- Cholecalciferol (Vit D3): 2,000-5,000 IU/day x 6-12 weeks in children with normal GI absorption, then maintenance
- Calcium supplementation if dietary intake is low
- Radiological findings improve rapidly with treatment
X-linked hypophosphatemic rickets:
- Oral phosphate supplementation + calcitriol (active Vit D)
- Burosumab (anti-FGF23 monoclonal antibody) - now approved for children, highly effective
- Dose for Vit D-resistant rickets: 40,000-80,000 IU/day initially, titrated up
Renal causes:
- Treat underlying CKD; calcitriol supplementation; phosphate binders
Key Point for This Case
At age 11, the most likely cause is either:
- Nutritional Vit D deficiency (especially if poor diet, limited sunlight, darker skin tone, or veiled/indoor lifestyle) - check 25-OH Vit D and ALP first
- X-linked hypophosphatemic rickets - if phosphate is low but Vit D is normal and there is a family history, or if it has been refractory to standard Vit D therapy
The short stature results from impaired growth plate mineralization rather than a primary GH/IGF-1 problem, and will improve with correction of the underlying metabolic defect.
- Grainger & Allison's Diagnostic Radiology, pp. 1909-1911
- Miller's Review of Orthopaedics 9th Ed., p. 322
This is a shared conversation. Sign in to Orris to start your own chat.