DIAGNOSTIC CRITERIA FOR pediatric anaphylactic
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have all the key content. Here is a comprehensive answer:
Diagnostic Criteria for Pediatric Anaphylaxis
Anaphylaxis is primarily a clinical diagnosis. The NIAID/FAAN and WAO (World Allergy Organization) guidelines provide consensus criteria that apply to all ages, including children, with specific pediatric blood pressure thresholds. Sensitivity is ~95–97% and specificity ~71–82%.
WAO/NIAID-FAAN Clinical Criteria
Anaphylaxis is highly likely when ANY ONE of the following three criteria is met:
Criterion 1 — Skin/Mucosal Involvement + At Least One More System
Sudden onset (minutes to several hours) with:
- Skin or mucosal involvement (e.g., generalized urticaria, pruritus, flushing, swollen lips/tongue/uvula)
PLUS at least one of:
- (a) Respiratory compromise — dyspnea, wheeze, cough, stridor, hypoxemia
- (b) Reduced BP or end-organ dysfunction — hypotonia (collapse), syncope, incontinence
Criterion 2 — Two or More Systems Rapidly Involved (No Prior Known Allergen Required)
Two or more of the following occurring rapidly after exposure to a likely allergen or trigger:
| Feature | |
|---|---|
| (a) | Skin/mucosal involvement — hives, itch/flush, swollen lips/tongue/uvula |
| (b) | Sudden respiratory compromise — dyspnea, wheeze, cough, stridor, hypoxemia |
| (c) | Sudden reduced BP or end-organ dysfunction — hypotonia, syncope, incontinence |
| (d) | Sudden gastrointestinal symptoms — crampy abdominal pain, vomiting |
Criterion 3 — Hypotension After Exposure to a Known Allergen
Reduced BP occurring minutes to several hours after exposure to a known allergen for that patient:
Pediatric-specific BP thresholds:
| Age | Low Systolic BP |
|---|---|
| 1 month – 1 year | < 70 mmHg |
| 1 – 10 years | < 70 mmHg + (2 × age in years) |
| 11 – 17 years | < 90 mmHg |
OR: > 30% decrease in systolic BP from baseline at any pediatric age.
Key Pediatric Considerations
- Hypotension and shock are rare presenting features in infants and children — unlike adults where they are more common. Skin and respiratory manifestations dominate in the pediatric population.
- Under-recognition is a major risk factor for increased anaphylaxis severity in very young children.
- Idiopathic anaphylaxis accounts for up to 10% of pediatric cases (vs. 30–60% in adults).
- Food (especially peanut, tree nuts, milk, egg) is the most common trigger in children.
- Teenagers are at increased incidence risk, particularly for food-triggered reactions.
Clinical Manifestations by Frequency
| System | Frequency |
|---|---|
| Skin (urticaria, angioedema, flushing) | 80–90% |
| Respiratory (wheeze, stridor, dyspnea) | 70–80% |
| Cardiovascular (hypotension, dysrhythmia) | 30–50% |
| GI (vomiting, abdominal cramps) | 25–30% |
| CNS (seizure, altered mentation) | 20–30% |
Common Mimics to Exclude
- Vasovagal syncope (bradycardia, no urticaria)
- Acute asthma exacerbation (no skin findings)
- Panic attack
- Flush syndromes (scrombroidosis, sulfites — lack hypotension and airway involvement)
— ROSEN's Emergency Medicine: Concepts and Clinical Practice, Box 106.5 & Table 106.2
INITIAL ASSESSMENT
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of the initial assessment of pediatric anaphylaxis:
Initial Assessment of Pediatric Anaphylaxis
1. Rapid Recognition
Anaphylaxis is primarily a clinical diagnosis — lab tests are not needed before acting. The goal is immediate recognition using the WAO/NIAID-FAAN criteria (skin/mucosal involvement + respiratory or cardiovascular compromise; or ≥2 organ systems; or hypotension after known allergen).
Key clinical presentations in children:
| System | Manifestation | Frequency |
|---|---|---|
| Cutaneous | Urticaria, angioedema, flushing, pruritus | 80–90% |
| Respiratory | Wheeze, stridor, dyspnea, cough | 70–80% |
| Cardiovascular | Hypotension, syncope, tachycardia | 30–50% |
| GI | Vomiting, cramping, diarrhea | 25–30% |
| CNS | Altered consciousness, seizure | 20–30% |
Critical pediatric note: Hypotension and shock are rare initial features in children — skin and respiratory signs dominate. Under-recognition in infants is a leading cause of increased severity.
2. Immediate Assessment Steps (ABC-Based)
A — Airway
- Assess for stridor, voice changes, throat tightness, uvular/tongue swelling
- Signs of upper airway edema demand urgent airway management
- Allow child to assume a position of comfort if distressed
B — Breathing
- Assess for wheeze, tachypnea, use of accessory muscles, hypoxemia
- Attach pulse oximetry immediately
- Administer supplemental oxygen
C — Circulation
- Assess heart rate, capillary refill, BP (using pediatric-specific thresholds)
- Establish IV access
- Attach continuous cardiac monitoring
D — Disability / Neurological
- Level of consciousness (AVPU or GCS)
- Hypotonia or collapse in infants = sign of cardiovascular compromise
E — Exposure
- Identify and remove the trigger (e.g., remove insect stinger, stop infusing medication)
- Look for rash, angioedema across the full body
3. Positioning
- Hypotensive child: Supine with lower extremities elevated
- Airway compromise or vomiting: Allow position of comfort; attempt leg elevation if possible
- Never leave child sitting upright or standing — upright posture at anaphylaxis onset is associated with increased mortality
4. Immediate Intervention — Epinephrine First
Prompt recognition must be immediately followed by epinephrine — do not delay for observation or antihistamines.
"Prompt recognition and initiation of appropriate interventions remain key in avoiding adverse outcomes. Treatment delays, even by a few minutes, could potentially lead to hypoxia, circulatory collapse, and even death."
| Parameter | Pediatric Dose |
|---|---|
| Epinephrine IM | 0.01 mg/kg of 1:1000 (1 mg/mL) concentration |
| Route | IM into the lateral thigh (vastus lateralis) |
| Max single dose | 0.5 mg |
| Repeat | Every 5–10 minutes as needed (up to 30% require >1 dose) |
- IM lateral thigh achieves peak plasma concentration in ~8 minutes vs. subcutaneous route (~34 minutes)
- Subcutaneous and inhaled epinephrine are no longer recommended
5. Concurrent Monitoring Setup
- Continuous cardiac monitoring
- Pulse oximetry
- IV access (x2 if possible)
- Supplemental O₂ — target SpO₂ ≥95%
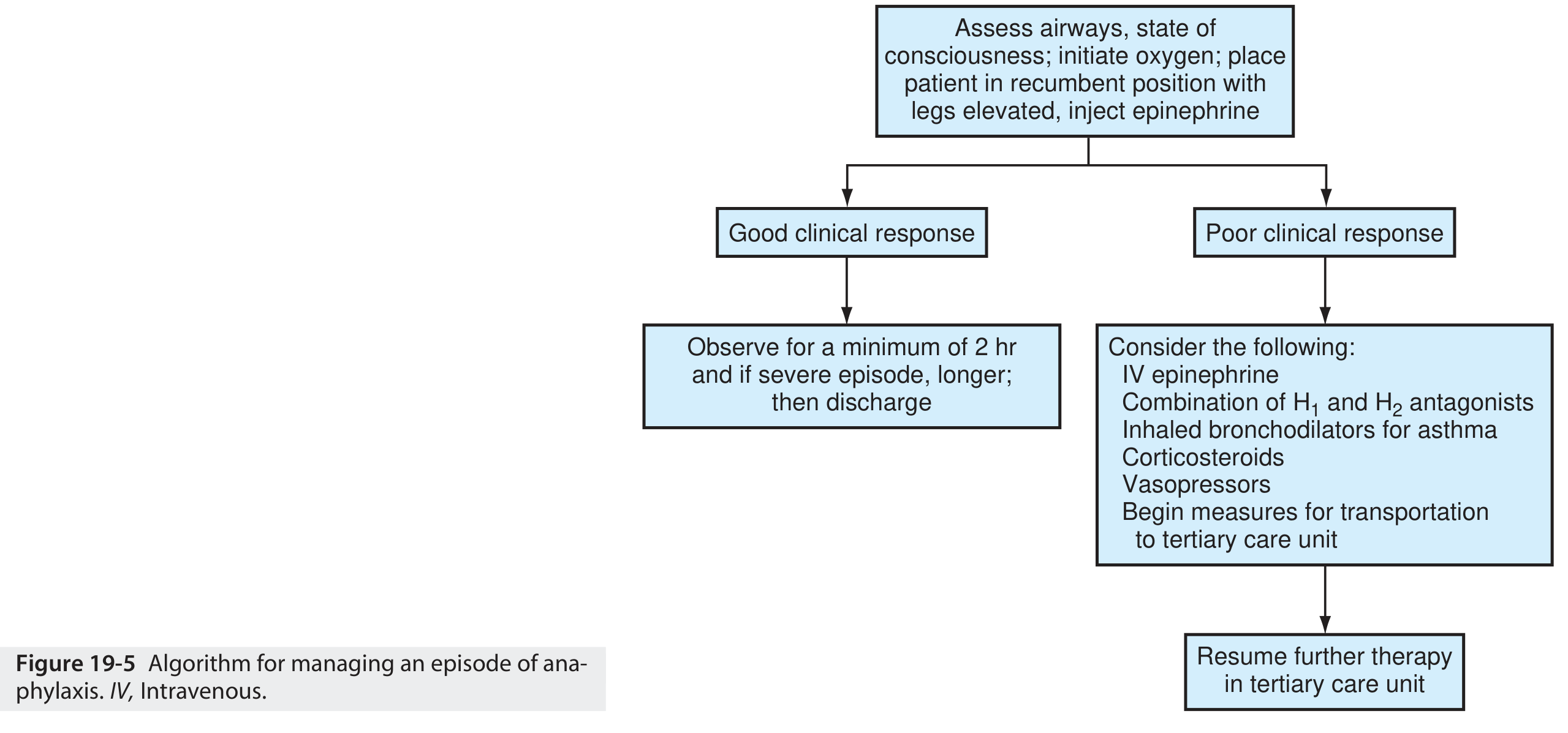
6. Clinical Algorithm
7. Biphasic Reaction Awareness
After initial stabilization, observe for a biphasic reaction — a second wave of anaphylaxis occurring hours after apparent resolution. This influences the decision for observation vs. discharge.
Key Takeaway
The initial assessment follows a rapid ABCDE framework with simultaneous trigger removal and epinephrine IM as the first and only first-line drug. Antihistamines and corticosteroids are adjuncts only and must never delay or replace epinephrine.
— ROSEN's Emergency Medicine: Concepts and Clinical Practice, Chapter 106; Textbook of Family Medicine 9e, Chapter 19
FIRST LINE MANAGEMENT AND SUPPORTIVE MANAGEMENT
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
All content retrieved. Here is the comprehensive structured response:
First-Line & Supportive Management of Pediatric Anaphylaxis
FIRST-LINE MANAGEMENT
1. Epinephrine — The Only First-Line Drug
"Epinephrine is the sole first-line medication and should be given immediately whenever anaphylaxis is suspected."
Delay in administration is directly associated with hypoxic encephalopathy, increased hospitalization, and death. Despite established guidelines, only ~30% of patients receive epinephrine prehospital and 50–70% receive it in the ED.
| Parameter | Pediatric Details |
|---|---|
| Drug | Aqueous epinephrine 1:1000 (1 mg/mL) |
| Dose | 0.01 mg/kg IM |
| Max single dose | 0.5 mg |
| Route | IM into anterolateral thigh (vastus lateralis) |
| Repeat | Every 5–10 minutes as needed (up to 30% require >1 dose) |
| Auto-injector | EpiPen Jr (0.15 mL) for children <25 kg |
Why the lateral thigh? Peak plasma concentration achieved in ~8 minutes vs. ~34 minutes with subcutaneous route. Subcutaneous and inhaled routes are no longer recommended.
Mechanism of Epinephrine:
| Receptor | Effect |
|---|---|
| α₁ | Vasoconstriction, ↑ peripheral vascular resistance, ↓ mucosal edema |
| β₁ | ↑ Inotropy & chronotropy (reverses cardiovascular collapse) |
| β₂ | Bronchodilation, mast cell/basophil stabilization → ↓ mediator release |
There is no absolute contraindication to epinephrine in anaphylaxis — benefits always outweigh risks, including in children with cardiovascular disease.
2. Simultaneous Emergency Measures (Taken Concurrently with Epinephrine)
| Action | Pediatric Detail |
|---|---|
| Remove trigger | Stop infusing drug, remove insect stinger |
| Positioning | Supine + legs elevated (if hypotensive); position of comfort if airway distress |
| Oxygen | Supplemental O₂ via mask; target SpO₂ ≥95% |
| Monitoring | Continuous cardiac + pulse oximetry + BP |
| IV access | Establish promptly; intraosseous if IV fails |
| Airway preparation | Be ready for endotracheal intubation ± RSI; awake fiberoptic or surgical airway if needed |
3. Fluid Resuscitation
Distributive shock from anaphylaxis causes massive fluid extravasation into the extravascular space.
| Agent | Pediatric Dose |
|---|---|
| Isotonic crystalloid (Normal Saline) | 20–30 mL/kg IV boluses, repeated as needed |
| Alternative access | Intraosseous (IO) if IV unavailable |
Large volumes may be required. Monitor closely in children with cardiac or renal disease.
SUPPORTIVE (SECOND-LINE) MANAGEMENT
These agents must never precede or replace epinephrine.
4. Antihistamines
- Useful for cutaneous symptoms (urticaria, pruritus, flushing) only
- No effect on hypotension or airway obstruction
- Never used as sole or initial treatment
| Drug | Pediatric Dose |
|---|---|
| Diphenhydramine (H₁ blocker) | 1 mg/kg IV or oral |
| Famotidine (H₂ blocker) | 0.5 mg/kg IV or oral |
5. Aerosolized Beta-Agonists (Bronchospasm)
Used adjunctively when bronchospasm persists after epinephrine — does not replace epinephrine.
| Drug | Pediatric Dose |
|---|---|
| Albuterol | 2.5 mg diluted in 3 mL NS; repeat or continuous as needed |
| Ipratropium | 0.25 mg in 3 mL NS; repeat as needed |
6. Glucocorticoids
- No acute benefit — onset of action takes several hours
- Theoretically may prevent protracted symptoms or biphasic reaction, but no strong evidence supports this
- Optional adjunct only — never precede epinephrine
| Drug | Pediatric Dose |
|---|---|
| Methylprednisolone | 1–2 mg/kg IV |
| Prednisolone/prednisone | 1–2 mg/kg oral |
7. Refractory Hypotension — Escalation
For children who fail to respond to repeated IM epinephrine + volume expansion:
| Agent | Pediatric Dose |
|---|---|
| IV Epinephrine infusion | Start 0.1 μg/kg/min, titrate by 0.1 μg/kg/min increments → max 1.5 μg/kg/min |
| Dopamine | 5–20 μg/kg/min continuous IV |
| Norepinephrine | 0.05–0.5 μg/kg/min titrated |
| Vasopressin | 0.01–0.4 units/min |
Central venous access is strongly recommended for IV epinephrine infusion due to risk of tissue necrosis from extravasation.
8. Beta-Blocker Patients — Glucagon
Children on beta-blockers may not respond to epinephrine (β-adrenergic blockade). Glucagon works independently of adrenergic receptors.
| Drug | Pediatric Dose |
|---|---|
| Glucagon | 20–30 μg/kg IV over 5 min (max 1 mg), then 5–15 μg/min infusion |
Nausea/vomiting are common — have antiemetic available.
Summary Hierarchy
ANAPHYLAXIS IDENTIFIED
↓
1. EPINEPHRINE IM (0.01 mg/kg lateral thigh) ← ONLY first-line drug
↓
2. O₂ + Monitoring + IV Access + Fluid Bolus (20–30 mL/kg NS)
↓
3. Repeat Epinephrine q5–10 min if no response
↓
4. Antihistamines + Bronchodilators + Steroids (adjuncts only)
↓
5. IV Epinephrine infusion / Vasopressors (refractory cases)
↓
6. Glucagon (if on beta-blockers)
Disposition
| Scenario | Observation Period |
|---|---|
| Complete symptom resolution after treatment | Minimum 1–4 hours |
| High biphasic risk (hypotension, >1 epi dose, unknown trigger) | 6 hours or longer |
| Protracted anaphylaxis, airway involvement, >2 IM epi doses | Hospitalize |
Biphasic reaction occurs in up to 20% of cases — typically within 8 hours but reported up to 72 hours. Clinically important biphasic reactions are rarer than historically reported.
At discharge: prescribe epinephrine auto-injector, provide written action plan, arrange allergist follow-up.
— ROSEN's Emergency Medicine: Concepts and Clinical Practice, Box 106.7 & Chapter 106
This is a shared conversation. Sign in to Orris to start your own chat.