Old MI ecg changes
Reading File
Finding Sources
Finding Sources
Searching Images
old myocardial infarction ECG changes Q waves ST T wave
Reading File
Loading Image
Loading Image
Loading Image
Here is a comprehensive overview of ECG changes in old (healed) myocardial infarction.
ECG Changes in Old (Healed) MI
Evolution Over Time
The ECG changes after an MI evolve through distinct phases. This diagram from Guyton & Hall shows the progression in a V3 lead after anterior wall infarction:
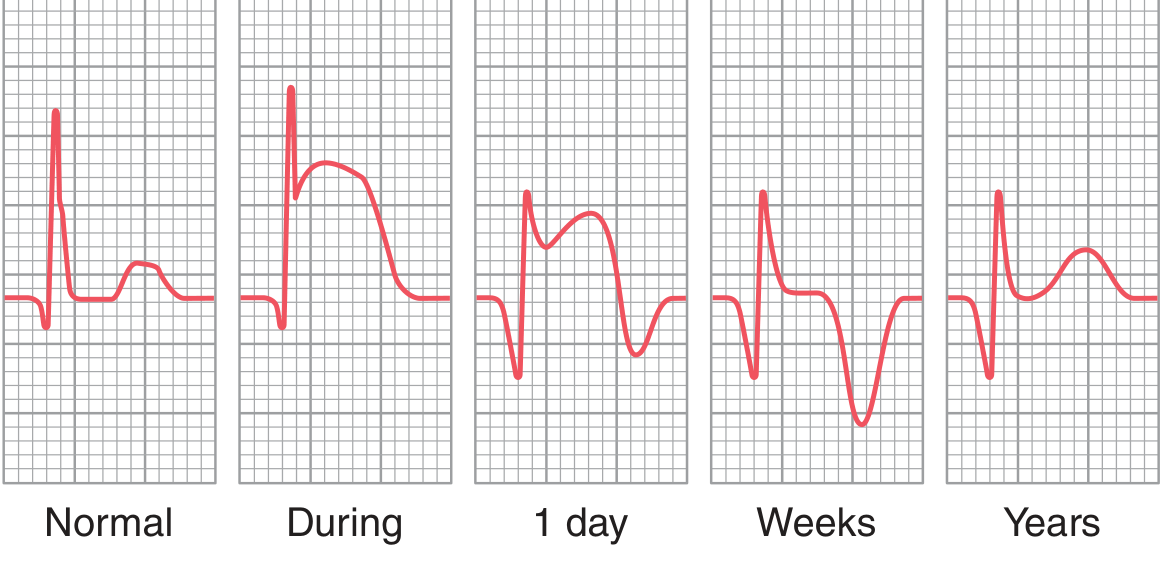
| Phase | Timeframe | Key Changes |
|---|---|---|
| Acute (hyperacute) | Minutes–hours | Tall, peaked T waves; ST elevation (injury current) |
| Acute | Hours–days | ST elevation maximal; Q waves begin to form |
| Subacute | Days–weeks | ST elevation resolves; T-wave inversion deepens |
| Old/healed | Weeks–years | ST returns to baseline; T may normalize; Q waves persist |
The Hallmark of Old MI: Pathological Q Waves
The defining feature of old MI on ECG is the persistent pathological Q wave. Once the injury current resolves (by ~3 weeks), Q waves remain as the signature of irreversible myocardial death.
Criteria for a pathological Q wave:
- Width ≥ 0.04 seconds (1 small square)
- Depth ≥ 25% of the following R wave height
- Present in ≥ 2 contiguous leads
Mechanism: Necrotic myocardium is electrically silent. During ventricular activation, the vector points away from the infarcted zone, creating a negative deflection (Q wave) in leads overlying the infarct.
Localisation by Lead Distribution
| Territory | Culprit artery | Leads with Q waves |
|---|---|---|
| Anterior | LAD | V1–V4 |
| Anterolateral | LAD / LCx | V1–V6, I, aVL |
| Inferior | RCA (or LCx) | II, III, aVF |
| Lateral | LCx | I, aVL, V5–V6 |
| Posterior | RCA / LCx | Tall R in V1–V2 (reciprocal Q) |
- Anterior infarction: Q wave in lead I at the beginning of QRS (loss of anterior LV muscle mass)
- Inferior/posterior infarction: Q wave in lead III (loss of inferior/apical LV muscle)
Other ECG Features of Old MI
- Loss of R-wave progression — R waves fail to grow in V1–V4; may have rS or QS pattern in anterior leads
- T-wave inversion — may persist chronically, especially in anterolateral leads; can indicate ventricular aneurysm if ST remains persistently elevated with deep T inversions
- Persistent ST elevation — if present >3 months after acute event, suggests left ventricular aneurysm (dyskinetic scar)
- Reduced QRS voltage — due to replacement of myocardium by scar
- QRS prolongation — due to conduction block in infarcted tissue; may also see fascicular blocks (e.g., LAFB with inferior MI)
- Bizarre QRS patterns — local conduction block from scar can distort morphology
Example ECGs
Old inferoanterior MI — deep Q waves in II, III, aVF (inferior) and V1–V4 (anterior); loss of R-wave progression precordially; mild ST/T changes:

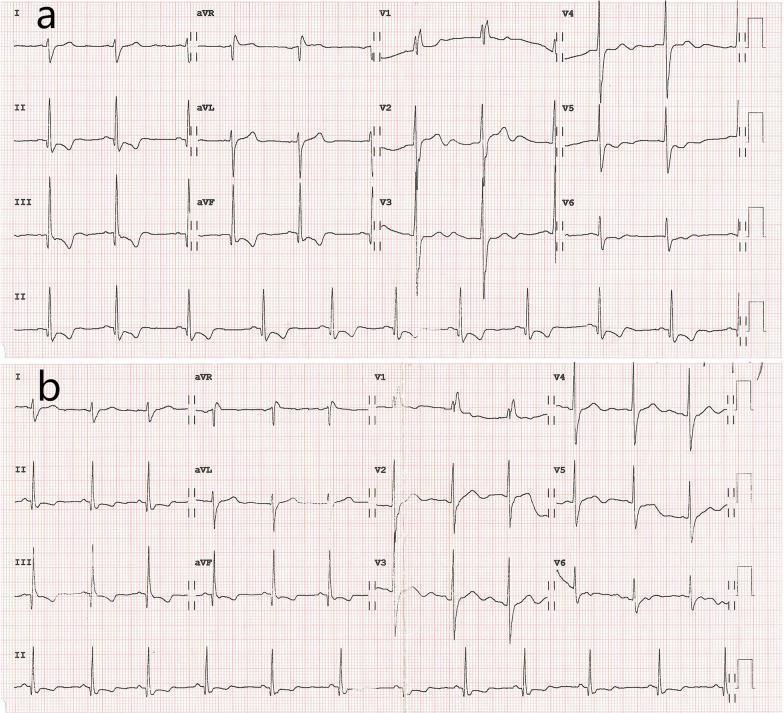
Before/after revascularisation — Panel (a) shows old inferior MI with pathological Q waves in II, III, aVF plus RBBB; Panel (b) shows ST improvement after stenting, but Q waves and RBBB persist (permanent scar):
Key Points
- Q waves are permanent in most cases — they do not resolve with reperfusion (unlike ST changes)
- Not all old MIs show Q waves ("non-Q wave MI" or NSTEMI may heal without Q waves)
- Q waves alone do not distinguish old from very recent MI — clinical context and serial ECGs are essential
- ICD coding: Old MI (healed, past MI diagnosed on ECG but currently asymptomatic) = ICD-9 412
— Guyton and Hall Textbook of Medical Physiology; Tintinalli's Emergency Medicine
This is a shared conversation. Sign in to Orris to start your own chat.