Rheumatic heart disease
Reading File
Finding Sources
Searching PubMed
"rheumatic heart disease"[MeSH Terms]
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive data from multiple authoritative textbooks. Let me compile the full answer.
Rheumatic Heart Disease (RHD)
The famous French aphorism by Lasegue (1884) perfectly captures the essence: "Rheumatic fever licks the joints but bites the heart." RHD is the chronic cardiac sequela of acute rheumatic fever (ARF), caused by an abnormal immune response to Group A beta-hemolytic streptococcal (GAS) pharyngitis, resulting in progressive valvular damage.
Epidemiology
- Global burden: RHD affects over 40.5 million people worldwide and caused approximately 305,651 deaths in 2019, resulting in 10.7 million DALYs lost annually - almost entirely in endemic countries.
- Incidence of ARF: ~19/100,000 globally; lowest in North America/Western Europe (<10/100,000), highest in Eastern Europe, Middle East, Asia, Africa, and Oceania.
- Age: Most common between ages 5-30; peak onset of ARF is 5-15 years.
- Sex: Women are ~1.8 times more susceptible to developing RHD, and disease is more severe in females than males.
- High-burden regions: Central sub-Saharan Africa, South Asia, and Oceania (particularly indigenous populations).
- India: Prevalence of 5-7 per 1000 in the 5-15 age group; RHD constitutes 20-30% of hospital admissions for cardiovascular disease.
- Declining in affluent nations: But persists in pockets of poverty even in high-income countries.
(Fuster and Hurst's The Heart, 15th Edition; Park's Textbook of Preventive and Social Medicine)
Pathophysiology
Molecular Mimicry - The Core Mechanism
RHD is an autoimmune disease triggered by molecular mimicry between streptococcal antigens and cardiac proteins:
- GAS pharyngitis triggers antibody production against streptococcal M-protein and N-acetyl-glucosamine (streptococcal carbohydrate).
- These antibodies cross-react with cardiac myosin, tropomyosin, and laminin in valve tissue - a phenomenon called molecular mimicry.
- Cross-reactive antibodies bind to valvular endothelium and basement membrane, upregulating adhesion molecules including VCAM-1 (vascular cell adhesion molecule-1).
- VCAM-1 interacts with VLA-4 (very late activation antigen-4) on CD4+ T lymphocytes, facilitating their infiltration into heart tissue.
- Chemokines including CCL1/I-309 and CXCL9/Mig are highly expressed in valvular tissue, mediating both CD4+ and CD8+ T cell infiltration.
- Cardiac myosin is the major autoantigen; ~63% of intralesional T cell clones in valve tissue recognize light meromyosin (LMM) peptides.
Pathological Hallmark: The Aschoff Body
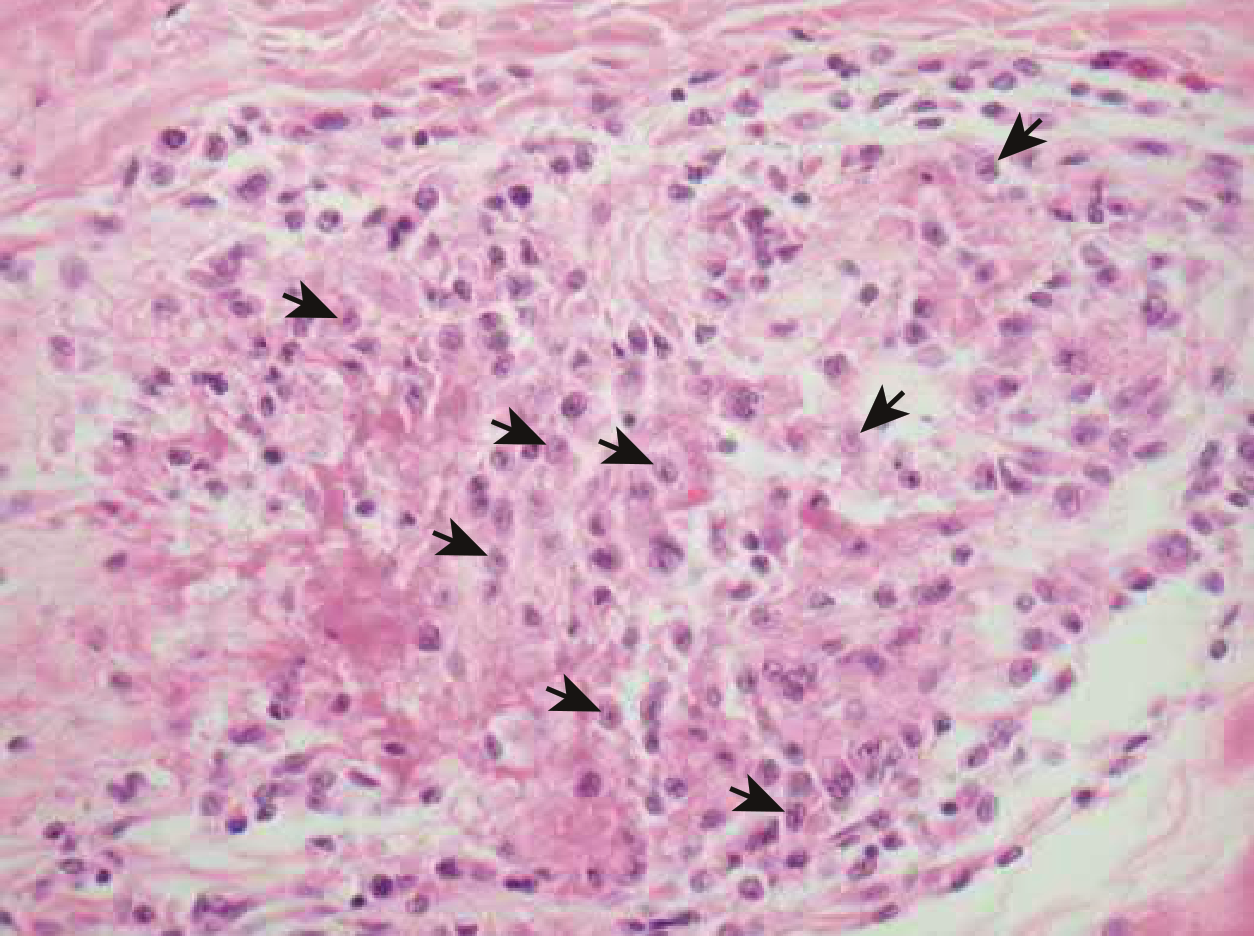
Aschoff nodule (arrows): Composed of Anitschkow cells with clear nuclei and a central chromatin bar resembling a caterpillar. Central fibrinoid necrosis is surrounded by mononuclear cell infiltrate. Myocardial fibers adjacent to the nodule undergo destruction. - Braunwald's Heart Disease
The Aschoff body is the pathognomonic granulomatous lesion of rheumatic carditis, found in the myocardium. It consists of:
- A central zone of fibrinoid necrosis
- Anitschkow (caterpillar) cells - modified macrophages with characteristic nuclei
- Surrounding mononuclear infiltrate (lymphocytes, plasma cells)
Valve Involvement
| Valve | Frequency |
|---|---|
| Mitral | ~100% |
| Aortic | 20-30% |
| Tricuspid | 15-40% (histologic only, rarely clinical) |
| Pulmonic | Rare |
- Mitral regurgitation is the most common early lesion.
- Mitral stenosis develops from progressive scarring - RHD is the most common cause of MS worldwide.
- Aortic involvement: regurgitation more common than stenosis.
(Firestein & Kelley's Textbook of Rheumatology; Goldman-Cecil Medicine)
Acute Rheumatic Fever (ARF) - Clinical Features
ARF precedes RHD. It occurs 2-4 weeks after GAS pharyngitis. The major manifestations (in order of frequency):
1. Arthritis (Most Common - 65-75%)
- Migratory polyarthritis - large joints (ankles, knees, elbows, wrists)
- Begins asymmetrically in lower limbs before spreading to upper limbs
- Pain is disproportionate to physical signs (opposite to Lyme arthritis)
- Resolves completely within 4 weeks; if persistent, consider JIA or SLE
- In high-risk populations (India, Australia, Fiji): monoarthritis occurs in 17-25%
- Jaccoud arthropathy: rare chronic post-RF arthropathy with swan neck deformity, ulnar deviation - no erosions on X-ray
2. Carditis (35-72% clinical; 18% subclinical on echo)
- Pancarditis: affects endocardium, myocardium, and pericardium
- Presents as: new murmur, tachycardia out of proportion to fever, pericardial friction rub, cardiomegaly, or heart failure
- Subclinical carditis detectable by echocardiography (important addition in 2015 Jones Criteria revision)
- Most likely to resolve in the first year after acute episode
3. Sydenham's Chorea (10-30%)
- Involuntary, purposeless movements of face, trunk, and extremities
- Emotional lability, muscle weakness
- Appears late (up to 6 months after GAS infection - "pure chorea")
- Can occur in isolation without other manifestations
4. Erythema Marginatum (<5%)
- Fleeting, non-pruritic, macular rash with pale centers and red margins
- Spreads centrifugally on trunk and proximal limbs (not face)
- Evanescent - may come and go within hours
5. Subcutaneous Nodules (<5%)
- Firm, painless nodules over bony prominences (elbows, wrists, knees, ankles, spinous processes)
- Associated with severe carditis
- Resolve spontaneously within weeks
Diagnosis: Revised Jones Criteria (2015 AHA)
Requirement: Evidence of preceding GAS infection (positive throat culture, rapid strep test, elevated/rising ASO or anti-DNase B titers) PLUS:
| Initial ARF | Recurrent ARF | |
|---|---|---|
| Criteria needed | 2 major OR 1 major + 2 minor | 2 major OR 1 major + 2 minor OR 3 minor |
Major Criteria
| Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|
| Carditis (clinical and/or subclinical echo) | Carditis (clinical and/or subclinical echo) |
| Polyarthritis only | Monoarthritis or polyarthritis; polyarthralgia (added) |
| Chorea | Chorea |
| Erythema marginatum | Erythema marginatum |
| Subcutaneous nodules | Subcutaneous nodules |
Minor Criteria
| Low-Risk | Moderate/High-Risk |
|---|---|
| Polyarthralgia | Monoarthralgia |
| Fever ≥38.5°C | Fever ≥38°C |
| ESR ≥60 mm/hr and/or CRP ≥3.0 mg/dL | ESR ≥30 mm/hr and/or CRP ≥3.0 mg/dL |
| Prolonged PR interval | Prolonged PR interval |
Low-risk populations: ARF incidence <2/100,000 school-aged children/year OR all-age RHD prevalence ≤1/1000/year.
(Adapted from 2015 AHA Scientific Statement; Braunwald's Heart Disease; Goldman-Cecil Medicine)
Echocardiographic Criteria for Rheumatic Valvulitis (WHO/WHF)
Pathologic mitral regurgitation requires all four:
- Seen in at least 2 views
- Jet length ≥2 cm in at least one view
- Peak velocity >3 m/sec
- Pansystolic jet in at least one envelope
Acute mitral valve changes: annular dilatation, chordal elongation/rupture, anterior leaflet tip prolapse, beading/nodularity.
Management
Acute Phase
| Intervention | Details |
|---|---|
| Hospitalization | All ARF patients |
| Eradication of GAS | Benzathine penicillin G 1.2 million units IM (single dose) OR oral penicillin V 10 days |
| Arthritis | Aspirin 80-100 mg/kg/day (max 4-8 g/day) OR naproxen 10-20 mg/kg/day; continue 1-2 weeks after all symptoms resolve |
| Carditis/Heart failure | Diuretics, ACE inhibitors/ARBs, fluid restriction, bed rest; severe cases: corticosteroids (limited evidence) |
| Chorea | Usually self-limiting; carbamazepine or sodium valproate if severe |
| Valve surgery | Rarely needed acutely; indicated for acute leaflet rupture |
Secondary Prophylaxis (Critical for preventing RHD progression)
| Drug | Dose | Route |
|---|---|---|
| Benzathine penicillin G (preferred) | 1.2 million units every 4 weeks (every 3 weeks in high-risk) | IM |
| Oral penicillin V | 250 mg twice daily | Oral |
| Oral amoxicillin | 250 mg twice daily | Oral |
| Azithromycin (penicillin allergy) | 250 mg daily | Oral |
Duration of secondary prophylaxis (AHA guidelines):
| Condition | Duration |
|---|---|
| ARF without carditis | 5 years or until age 21 |
| ARF with mild carditis (resolved) | 10 years or until age 21 |
| ARF with persistent valvular disease | 10 years or until age 40, sometimes lifelong |
2024 Cochrane Review (PMID: 39312290): Confirmed that long-term benzathine penicillin G prophylaxis reduces ARF recurrence and prevents progression to RHD. Adherence remains a major challenge globally (meta-analysis PMID: 39542478 found suboptimal adherence in many settings). A 2025 meta-analysis (PMID: 40333929) found severe adverse reactions to benzathine penicillin G are rare (0.2-2.1/1000 injections), supporting its continued use.
Chronic RHD - Natural History and Complications
- Progressive valvular scarring leads to severe disease in the 3rd-4th decade of life in untreated patients
- Premature death by age 35 or earlier without treatment
- Major complications:
- Mitral stenosis - breathlessness, hemoptysis, pulmonary hypertension, right heart failure
- Atrial fibrillation - from left atrial enlargement (major cause of stroke)
- Infective endocarditis - RHD is a leading risk factor in developing countries
- Heart failure - systolic and/or diastolic
- Pulmonary hypertension
- Thromboembolism/stroke - especially with AF and MS
- Variables predicting severity: number of previous ARF attacks, delay before starting therapy, female sex
- 60-80% of mitral insufficiency resolves with adherent prophylaxis
Surgical/Interventional Options for Chronic RHD
| Lesion | Intervention |
|---|---|
| Mitral stenosis | Percutaneous balloon mitral commissurotomy (PBMC) - preferred if anatomy suitable; Closed/open mitral commissurotomy; Mitral valve replacement |
| Mitral regurgitation | Mitral valve repair (preferred) or replacement |
| Aortic valve disease | Aortic valve repair or replacement |
Prevention
- Primordial: Address social determinants - overcrowding, poverty, poor sanitation
- Primary: Treat GAS pharyngitis with antibiotics within 9 days of onset (prevents first episode of ARF)
- Secondary: Long-term benzathine penicillin G after established ARF/RHD
- Echocardiographic screening: Population-based screening in endemic regions detects subclinical RHD and guides prophylaxis to reduce disease progression (prevalence 0.3-5.7 per 1000 by echo vs. lower by auscultation alone)
Key Points Summary
- RHD = autoimmune sequela of GAS pharyngitis via molecular mimicry
- Pathognomonic lesion = Aschoff body (Anitschkow cells)
- Mitral valve affected in virtually 100%; MR most common early, MS most common late
- Diagnosis by 2015 revised Jones Criteria (requires preceding GAS evidence + major/minor manifestations)
- Treatment: eradicate GAS + anti-inflammatory (aspirin) + manage carditis
- Secondary prophylaxis with benzathine penicillin G is the most important intervention to prevent progression
- RHD remains a leading preventable cause of cardiovascular mortality in low-income countries, affecting >40 million people globally
Sources: Braunwald's Heart Disease (15th ed.); Goldman-Cecil Medicine; Firestein & Kelley's Textbook of Rheumatology; Fuster and Hurst's The Heart (15th ed.); Park's Textbook of Preventive and Social Medicine; Sabiston Textbook of Surgery; Cochrane Database 2024 (PMID: 39312290); BMJ Open 2024 (PMID: 39542478); PLoS One 2025 (PMID: 40333929)
This is a shared conversation. Sign in to Orris to start your own chat.