- Fecal calprotectin (FC) and procalcitonin (PCT) test uses, indications,sensitivity, specificity
Reading File
Checking Date & Time
Finding Sources
Finding Sources
Searching PubMed
fecal calprotectin inflammatory bowel disease sensitivity specificity
Searching PubMed
procalcitonin sepsis bacterial infection sensitivity specificity
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have enough information to write a comprehensive answer. Let me compile everything.
Fecal Calprotectin (FC) and Procalcitonin (PCT): Uses, Indications, Sensitivity & Specificity
🔬 FECAL CALPROTECTIN (FC)
What is it?
Calprotectin is a member of the S100 family of zinc- and calcium-binding proteins (heterodimer of S100A8/9). It accounts for ~60% of cytosolic protein in neutrophils, with lower concentrations in monocytes and macrophages. When GI mucosal architecture is disrupted, neutrophils accumulate at sites of inflammation, are shed into the lumen, and FC concentrations rise — directly proportional to the extent of inflammation. It correlates well with the gold-standard indium-111-labeled granulocyte test. — Tietz Textbook of Laboratory Medicine, 7th Ed.
Indications / Uses
| Use | Detail |
|---|---|
| Distinguishing IBS from IBD | Primary clinical application — non-invasive triage to select patients for colonoscopy referral |
| Monitoring IBD disease activity | Differentiates active vs. inactive disease; correlates with mucosal healing |
| Predicting relapse in IBD | Elevated FC during clinical remission identifies patients at risk of relapse |
| Treatment response monitoring | A fall in FC concentration precedes clinical response and indicates response to therapy |
| Guiding therapy escalation | FC recommended before initiating or changing IBD therapy (e.g., biologics) |
| Post-op recurrence in Crohn's | Surrogate for endoscopic lesions; used for monitoring after surgery |
| Colorectal cancer screening | Elevated in colorectal carcinoma (but not specific) |
Sensitivity & Specificity
IBD vs. IBS distinction (the main diagnostic use):
| Study / Setting | Sensitivity | Specificity | Cut-off |
|---|---|---|---|
| King's College Hospital (n=602 primary care referrals) | 89% | 79% | — |
| Meta-analyses range (2019 review of multiple meta-analyses) | 83–99% | 53–96% | 50–60 µg/g |
| Primary care retrospective (n=946 from 48 practices) | 82% | 77% | — |
| Combining FC + Rome questionnaire | Predictive value approaching 100% | — | — |
Optimal cut-off: 50–60 µg/g — recommended by most commercial methods and NICE guidelines.
— Tietz Textbook of Laboratory Medicine, 7th Ed.
Diagnostic Algorithm
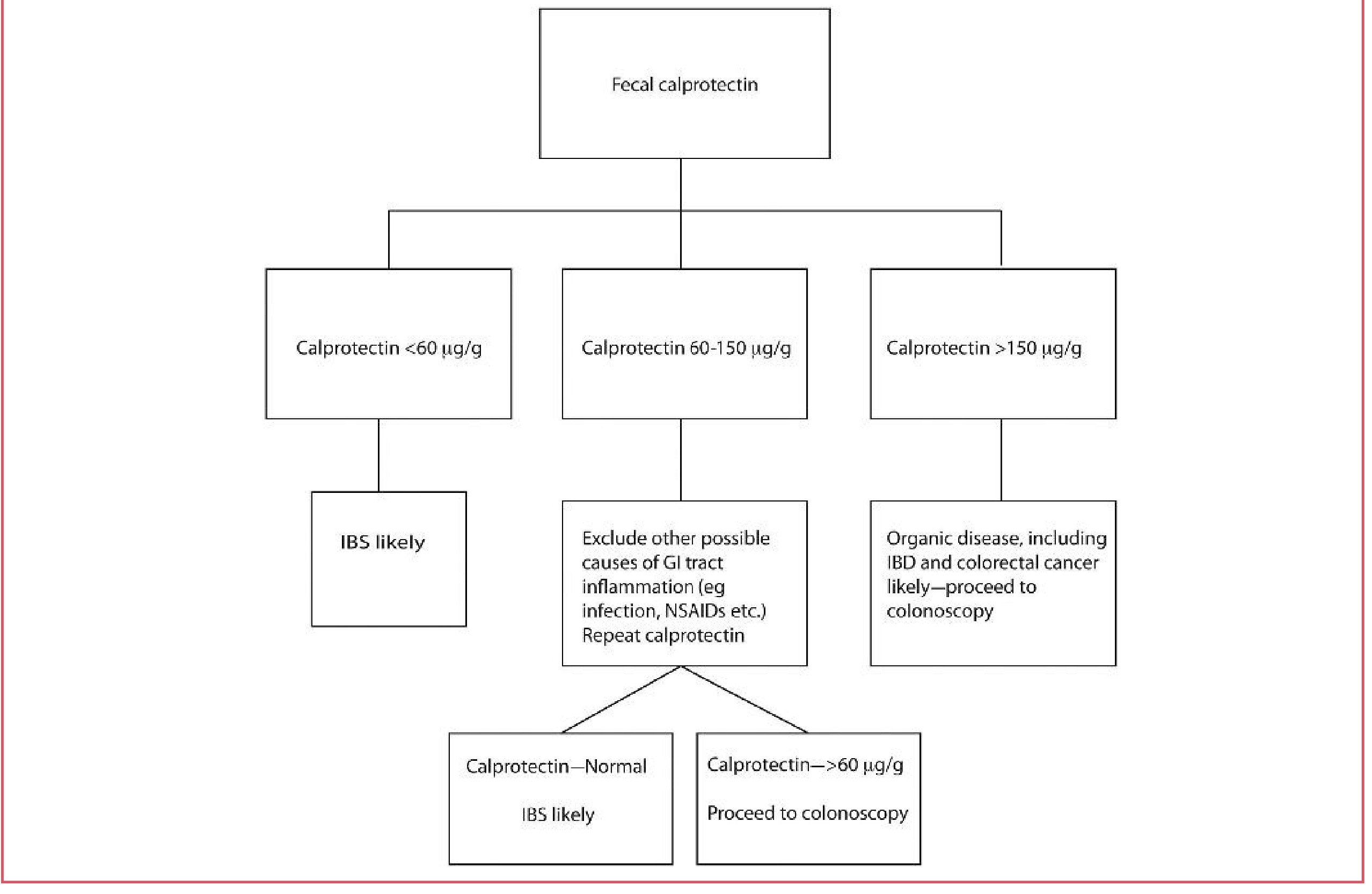
GI = gastrointestinal; IBD = inflammatory bowel disease; IBS = irritable bowel syndrome
Limitations of FC
- Not specific to IBD — also elevated in:
- Colorectal carcinoma
- Chronic NSAID use
- GI infections
- Diverticular disease
- ~38% of microscopic (collagenous) colitis patients have normal FC, limiting its utility there
- Higher in children than adults (age-adjusted reference ranges required)
- NICE (UK) recommends widespread use in general practice to triage referrals to gastroenterology, with significant cost savings
Recent Evidence (PubMed 2023–2025)
- Meta-analysis (Dajti et al., Aliment Pharmacol Ther 2023, PMID: 37823411): FC for IBD vs. IBS distinction in adults — confirmed diagnostic performance
- Systematic review (Samnani et al., Clin Gastroenterol Hepatol 2025, PMID: 40467019): FC useful for detecting postoperative Crohn's recurrence
🩸 PROCALCITONIN (PCT)
What is it?
PCT is a precursor peptide of calcitonin. It is released into the bloodstream when systemic inflammation is mediated by bacterial infection — triggered by bacterial toxins and cytokines (TNF-α, IL-1β, IL-6). Critically, viral infections do not stimulate PCT release, making it potentially useful for differentiating bacterial from viral/non-infectious inflammation. — Fishman's Pulmonary Diseases and Disorders
Indications / Uses
| Use | Detail |
|---|---|
| Bacterial vs. viral infection discrimination | Early detection of bacterial infections; distinguishes from viral pneumonia, non-infectious SIRS |
| Sepsis diagnosis and risk stratification | Elevated in sepsis; utility in predicting mortality |
| Antibiotic stewardship (serial monitoring) | Best-supported clinical use — guides when to stop antibiotics; Cochrane Review: PCT-guided protocols reduced antibiotic use, side effects, and mortality |
| Community-acquired pneumonia (CAP) | Aids decision on antibiotic initiation; threshold <0.25 ng/mL used by some institutions to stop antibiotics in stable patients |
| Bacterial vs. viral meningitis | Adjunct when clinical picture is unclear |
| ICU/critical care | Serial PCT trending more useful than a single value |
| Duration of antibiotic therapy | Used with source control to guide 3–7 day regimens in IAI/sepsis |
Sensitivity & Specificity
| Clinical Context | Sensitivity | Specificity | Notes |
|---|---|---|---|
| Bacterial meningitis (vs. viral) | ~90% | ~98% | Useful adjunct, not definitive to rule out |
| Bacterial infection / sepsis (general) | Moderate–high | Moderate | Varies widely by cut-off and population |
| CAP — bacterial vs. viral | Moderate | Moderate | Mycoplasma & Chlamydia may NOT elevate PCT |
Key cut-off values (clinical practice):
| PCT Level | Interpretation |
|---|---|
| < 0.1 ng/mL | Bacterial infection very unlikely |
| 0.1–0.25 ng/mL | Low likelihood; monitor |
| 0.25–0.5 ng/mL | Possible bacterial infection; consider antibiotics |
| > 0.5 ng/mL | High likelihood of bacterial infection / sepsis |
| > 2 ng/mL | Severe sepsis / septic shock likely |
| > 10 ng/mL | Septic shock / high mortality risk |
Limitations of PCT
- Mycoplasma and Chlamydia pneumonia do NOT reliably elevate PCT
- Single values have limited utility — serial measurements are more informative
- Cannot clearly determine bacterial vs. viral in all pneumonia cases
- Cannot discriminate infectious from non-infectious shock alone
- Requires rapid lab turnaround to be clinically useful
- IDSA/ATS guidelines make a strong recommendation against withholding antibiotics in radiographically proven pneumonia regardless of PCT level
- "PCT should supplement, rather than supplant, clinical judgment" — Fishman's Pulmonary Diseases and Disorders
Recent Evidence (PubMed 2023–2025)
- Systematic review (Julián-Jiménez et al., Rev Clin Esp 2024, PMID: 38815753): PCT diagnostic accuracy for bacterial infection in the ED
- Meta-analysis (Julián-Jiménez et al., Emergencias 2024, PMID: 38318742): Models to predict bacteremia including PCT in the ED
Quick Comparison Table
| Feature | Fecal Calprotectin (FC) | Procalcitonin (PCT) |
|---|---|---|
| Specimen | Stool | Serum |
| Primary use | GI mucosal inflammation (IBD vs. IBS) | Systemic bacterial infection, sepsis |
| Key clinical role | IBD triage, disease monitoring, relapse prediction | Antibiotic stewardship, sepsis risk |
| Optimal cut-off | 50–60 µg/g | 0.25–0.5 ng/mL (context-dependent) |
| Sensitivity | 82–99% (IBD vs. IBS) | ~90% (bacterial meningitis) |
| Specificity | 53–96% (IBD vs. IBS) | ~98% (bacterial meningitis) |
| Not elevated by | IBS, microscopic colitis (often) | Viral infections, Mycoplasma/Chlamydia |
| Best use | Avoid unnecessary endoscopy; monitor IBD therapy | Serial monitoring to guide antibiotic duration |
Sources: Tietz Textbook of Laboratory Medicine 7th Ed. · Fishman's Pulmonary Diseases and Disorders · Rosen's Emergency Medicine · Yamada's Textbook of Gastroenterology · Current Surgical Therapy 14th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.