Ebstein anomoly radiology
Reading File
Finding Sources
Searching Images
Ebstein anomaly radiology chest X-ray echocardiogram
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of the radiology of Ebstein anomaly:
Ebstein Anomaly — Radiology
Anatomy & Pathology
Ebstein anomaly is a congenital tricuspid valve and right ventricular malformation with six key components:
- Failure of delamination — leaflets adhere to underlying myocardium
- Apical displacement of the functional tricuspid annulus into the RV (septal leaflet displaced >8 mm/m², or >20 mm in adults)
- "Atrialised" RV — the basal portion of the RV functions as part of the right atrium, with variable wall thinning
- Redundant, "sail-like" anterior leaflet — may be fenestrated or tethered
- Right AV junction dilatation
- Variable RV myocardial dysfunction
Associated anomalies include ASD/PFO, accessory pathways (Wolff-Parkinson-White), pulmonary stenosis, VSD, and LV non-compaction.
Chest Radiograph

Classic CXR features:
- Massive cardiomegaly with a "box-shaped" or globular heart — a hallmark sign
- Prominent, curved right heart border — due to severe right atrial enlargement
- Decreased pulmonary vascularity (oligaemic lung fields) — from reduced pulmonary blood flow and/or right-to-left shunting through ASD
- Small aortic knob and pulmonary trunk shadow
- Cardiothoracic ratio ≥0.65 is a marker of poor prognosis in unoperated patients
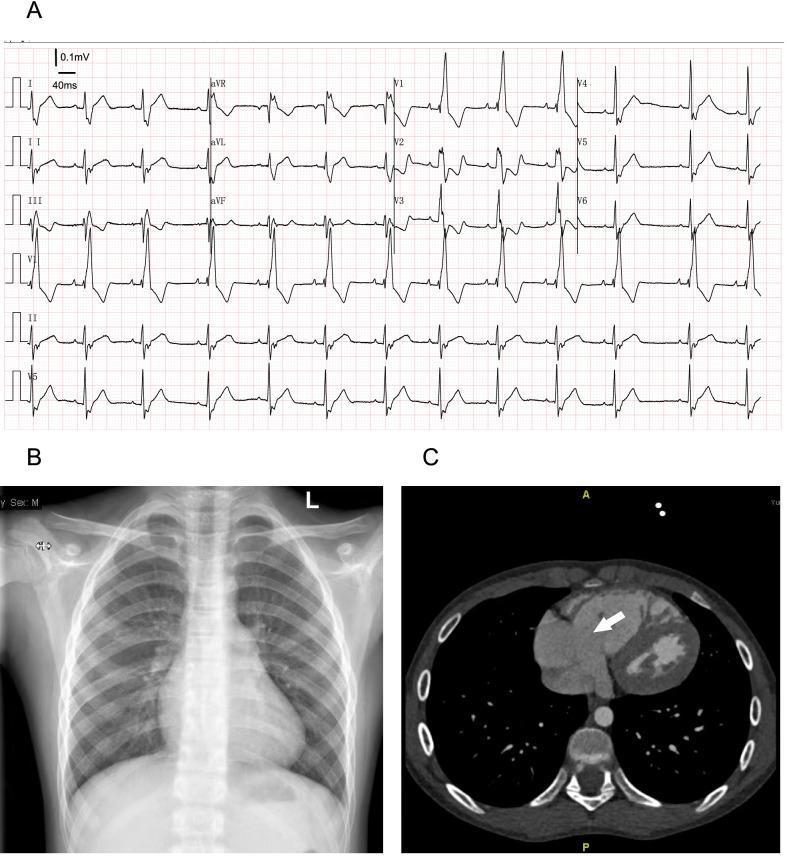
Panel B shows the prominent right heart border on PA CXR; Panel C (axial CT) demonstrates the enlarged tricuspid annulus (arrow).
Echocardiography (Primary Diagnostic Modality)
Key imaging goals:
- Apical displacement of the septal tricuspid leaflet — diagnostic criterion
- Assess leaflet mobility of the anterosuperior and inferior leaflets
- Note eccentric valve coaptation
- Quantify tricuspid regurgitation (severity)
- Size the atrialised RV and right atrium
- Assess RV and LV volumes and systolic function
- Evaluate ASD/PFO with shunt direction (right-to-left = cyanosis)
- Exclude RVOT obstruction
TTE + TEE may both be necessary — the anterior leaflet and distal tethering points can be far from the TEE probe.
Cardiac MRI (CMR)
CMR is increasingly used and provides:
- Degree of tricuspid valve displacement and rotation
- Quantification of tricuspid regurgitation
- RV and LV volumes (LV may be small due to septal shift)
- RV systolic function — CMR-derived RV and LV dysfunction predict mortality and sustained VT
- Cardiac output and Qp:Qs ratio (shunt quantification)
CT
Axial contrast-enhanced CT shows:
- Enlargement of the tricuspid annulus (see image above, white arrow)
- Right atrial and atrialised RV dilation
- Useful when CMR is contraindicated or for surgical planning
Key Imaging Summary Table
| Modality | Key Finding |
|---|---|
| CXR | Box-shaped cardiomegaly, oligaemic lungs, prominent right heart border |
| Echo | Apical septal leaflet displacement >8 mm/m², TR severity, atrialised RV |
| CMR | RV/LV volumes & function, TR quantification, Qp:Qs |
| CT | Tricuspid annulus enlargement, right heart dimensions |
Sources:
- Grainger & Allison's Diagnostic Radiology
- Braunwald's Heart Disease, 2-Vol Set
This is a shared conversation. Sign in to Orris to start your own chat.