Stable Angina
Reading File
Finding Sources
Searching PubMed
"stable angina" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a thorough clinical overview of Stable Angina Pectoris, drawn primarily from Harrison's Principles of Internal Medicine 22nd Edition (2025), Goldman-Cecil Medicine, and Lippincott Illustrated Reviews: Pharmacology.
Stable Angina Pectoris
Definition
Stable angina is an episodic clinical syndrome resulting from transient myocardial ischemia - an imbalance between myocardial oxygen demand and supply. The ischemia arises from a fixed atherosclerotic obstruction in one or more coronary arteries. It is called "stable" because the pattern of chest pain (threshold, frequency, duration) does not vary substantially over time.
- Males constitute ~70% of all patients; women tend to present at a later age (>60 years) and with more atypical symptoms.
Pathophysiology
Coronary blood flow is reduced by atherosclerotic plaque causing a fixed luminal obstruction. When myocardial oxygen demand rises (e.g., exertion, emotion), supply cannot increase adequately, causing ischemia. Vascular tone also modulates the effective degree of stenosis:
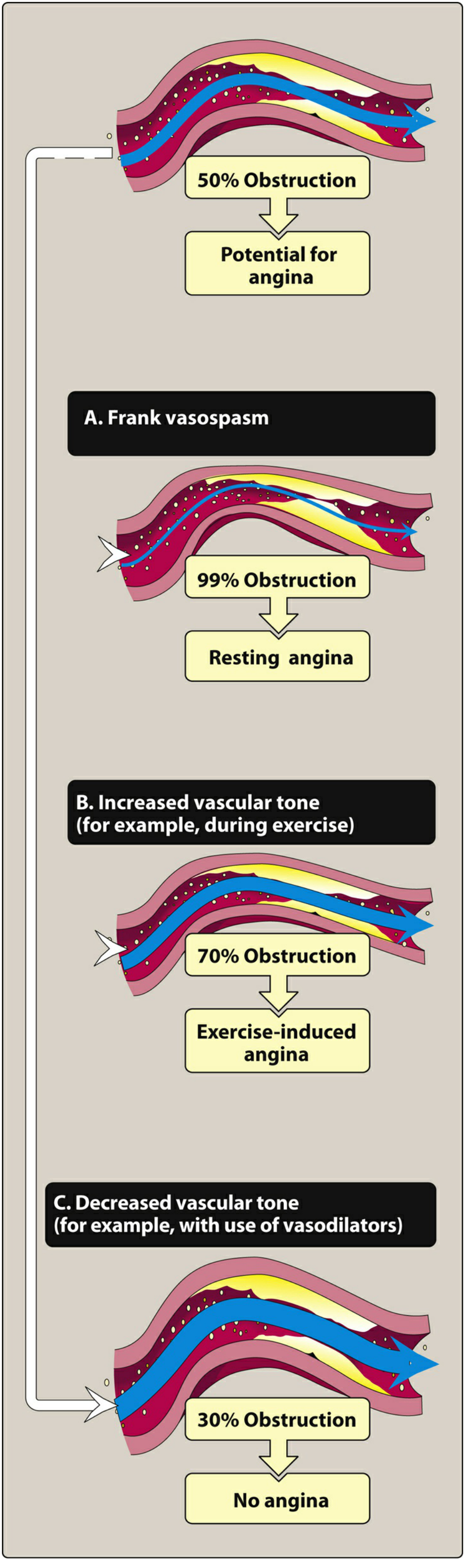
Lippincott Illustrated Reviews: Pharmacology - Figure 12.2
Key determinants of myocardial oxygen demand:
- Heart rate
- Systolic wall tension (preload + afterload)
- Myocardial contractility
Clinical Features
Symptoms
- Character: Heaviness, pressure, squeezing, smothering, or choking - rarely described as sharp pain
- Location: Central, substernal; patient typically places a clenched fist over the sternum (Levine's sign)
- Radiation: To either shoulder, ulnar aspect of forearm/hand, jaw, teeth, neck, back, interscapular region, or epigastrium. Notably, does not radiate to the trapezius muscles (that pattern suggests pericarditis)
- Duration: Typically 2-5 minutes
- Trigger: Exertion (exercise, hurrying, sexual activity), emotional stress, cold exposure, heavy meals
- Relief: Rest and/or sublingual nitroglycerin within 1-5 minutes
If angina does not respond to rest + sublingual nitroglycerin, the diagnosis should be reconsidered or unstable angina/ACS suspected.
Atypical Presentations
Women, diabetics, and the elderly may present with fatigue, nausea, or diaphoresis rather than chest pain ("silent angina").
Comparison with Other Angina Types
| Feature | Stable Angina | Unstable Angina | Prinzmetal (Vasospastic) |
|---|---|---|---|
| Trigger | Exertion/emotion | Minimal effort or rest | Rest (often nocturnal) |
| Fixed threshold | Yes | No (worsening) | No |
| Relief with rest/NTG | Yes | Partial/No | Yes (vasodilators) |
| Mechanism | Fixed obstruction | Plaque rupture/thrombus | Coronary vasospasm |
| Biomarkers | Normal | +/- elevated | Normal |
Canadian Cardiovascular Society (CCS) Classification
| Class | Description |
|---|---|
| I | Ordinary activity does not cause angina; angina with strenuous/rapid/prolonged exertion |
| II | Slight limitation of ordinary activity; angina walking >2 blocks or climbing >1 flight of stairs |
| III | Marked limitation; angina walking 1-2 blocks on the level or climbing 1 flight of stairs |
| IV | Inability to carry on any physical activity without discomfort; may occur at rest |
Investigations
Electrocardiography
- Resting ECG may be normal in ~50% of patients
- Exercise stress ECG: ST-segment depression (horizontal or downsloping ≥1 mm) is the classic ischemic finding
- ST depression does not localize the site of ischemia; ST elevation during stress does
Imaging
- Echocardiography: Assess LV function, wall motion abnormalities, rule out valvular disease
- Stress echocardiography / Nuclear myocardial perfusion imaging: For risk stratification and assessing extent of ischemia
- Coronary CT angiography (CCTA): Excellent negative predictive value; identifies obstructive CAD non-invasively
- Coronary artery calcium (CAC) score: Adjunctive tool; should not be the sole basis for therapeutic decisions
- Invasive coronary angiography: Gold standard; defines anatomy and guides revascularization decisions
Risk Stratification Markers
- Extent of CAD and LV function are the most important prognostic determinants
- Worse prognosis: advanced age (>75 years), hypertension, dyslipidemia, diabetes, obesity, peripheral/cerebrovascular disease, prior MI
- Additional markers: elevated CRP, extensive coronary calcification on EBCT, increased carotid intimal thickness
Management
The management plan has six components (Harrison's):
- Explanation and reassurance
- Identification and treatment of aggravating conditions
- Adaptation of activity
- Risk factor reduction
- Drug therapy
- Consideration of revascularization
1. Risk Factor Modification
- Smoking cessation (reduces carboxyhemoglobin, improves oxygen delivery)
- Control of hypertension, dyslipidemia, diabetes, obesity
- Treat thyrotoxicosis, anemia, LVH - these increase oxygen demand or reduce supply
2. Pharmacotherapy
Nitrates
- Mechanism: Systemic venodilation → reduce LV end-diastolic volume/pressure → reduce wall tension and O2 demand; also dilate epicardial coronary arteries and collaterals (via NO release → guanylyl cyclase → cGMP → smooth muscle relaxation)
- Sublingual NTG (0.3-0.6 mg): For acute episodes; up to 3 doses, 5 min apart
- Long-acting nitrates: Isosorbide dinitrate (10-40 mg orally 2-3x/day), Isosorbide 5-mononitrate (30-240 mg SR once daily)
- Important: A 10-12 hour nitrate-free interval is required daily to prevent tolerance
Beta-Blockers (First-line)
- Mechanism: Reduce heart rate and contractility → decrease myocardial O2 demand; also increase diastolic perfusion time by slowing heart rate
- Cardioselective agents (β1): Atenolol (50-200 mg/d), Bisoprolol, Metoprolol
- Non-selective: Propranolol, Nadolol, Carvedilol
- Target resting HR: 55-60 bpm
- Contraindications: Severe bronchospasm, significant bradycardia, advanced AV block (without pacemaker), decompensated heart failure
Calcium Channel Blockers (CCBs)
- Mechanism: Reduce myocardial O2 demand by vasodilation (reducing afterload) and/or slowing heart rate
- Dihydropyridines (Amlodipine, Nifedipine): Primarily vasodilatory; minimal chronotropic effect; used especially in vasospastic angina
- Non-dihydropyridines (Verapamil, Diltiazem): Both vasodilatory and rate-limiting; useful when beta-blockers are contraindicated
- Caution: Combining non-DHP CCBs with beta-blockers can cause profound bradycardia
Antiplatelet Therapy
- Aspirin (75-100 mg/day): Reduces risk of MI and death; mainstay in all patients with IHD without contraindication
Statins (HMG-CoA reductase inhibitors)
- Reduce LDL-cholesterol; stabilize plaques; reduce cardiovascular events
- High-intensity statin therapy indicated for all patients with established IHD
ACE Inhibitors / ARBs
- Indicated in patients with concomitant LV dysfunction, hypertension, or diabetes
- Reduce cardiovascular mortality in IHD
Ranolazine
- Late sodium current inhibitor; reduces intracellular Ca2+ overload; anti-ischemic without affecting HR or BP
- Useful as add-on therapy when beta-blockers/CCBs are insufficient or not tolerated
3. Revascularization
Percutaneous Coronary Intervention (PCI)
- Effective for symptom relief in patients with significant obstructive CAD
- A 2026 meta-analysis (PMID: 41130952) comparing PCI vs. optimal medical therapy in stable angina suggests similar outcomes for mortality/MI; PCI may provide superior angina relief but does not consistently improve survival over optimal medical therapy
- Drug-eluting stents are preferred over bare-metal stents
Coronary Artery Bypass Grafting (CABG)
- Preferred when:
- Left main stenosis >50%
- Triple-vessel disease
- Double-vessel disease with proximal LAD involvement
- Reduced LV function
- Strongly abnormal exercise test
- Diabetes with multi-vessel disease
- CABG provides more consistent and durable angina relief than PCI in complex anatomy
Prognosis
- Prognosis is determined primarily by LV function and extent of CAD
- The more myocardium at risk, the worse the outlook
- Annual mortality in medically managed stable angina: ~1-3%, varying widely by risk profile
- Patients with left main or three-vessel disease have substantially improved survival with CABG vs. medical therapy alone
Key Points Summary
| Aspect | Key Fact |
|---|---|
| Mechanism | Fixed coronary obstruction → ischemia with increased demand |
| Classic symptom | Substernal pressure, 2-5 min, relieved by rest/NTG |
| Levine's sign | Clenched fist over sternum |
| Diagnostic gold standard | Invasive coronary angiography |
| First-line drug | Beta-blockers + aspirin + statin |
| Nitrate-free interval | 10-12 hours/day mandatory |
| CABG indications | Left main, 3-vessel, proximal LAD + LV dysfunction |
| PCI vs. medical therapy | Similar hard outcomes; PCI superior for symptom relief |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. (2025), Chapter 284 - Stable Ischemic Heart Disease
- Goldman-Cecil Medicine, International Edition - Chapter on CABG Indications
- Lippincott Illustrated Reviews: Pharmacology - Chapter 12 (Antianginal Drugs)
- PMID: 41130952 - Medical Management vs. PCI in Stable Angina (Meta-analysis, 2026)
This is a shared conversation. Sign in to Orris to start your own chat.