Ebstein anomoly radiology
Reading File
Finding Sources
Searching Images
Ebstein anomaly radiology chest X-ray echocardiography
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Here is a comprehensive radiology overview of Ebstein Anomaly:
Ebstein Anomaly — Radiology
Anatomy (Pathological Basis)
Ebstein anomaly is a congenital tricuspid valve and right ventricular (RV) malformation with six key components:
- Failure of delamination (adherence of tricuspid leaflets to underlying myocardium)
- Apical/anterior displacement of the functional tricuspid annulus
- Dilation of the "atrialized" RV with variable wall thinning
- Redundant, fenestrated, sail-like anterior leaflet
- Dilation of the true tricuspid annulus (right AV junction)
- Variable RV myocardial dysfunction
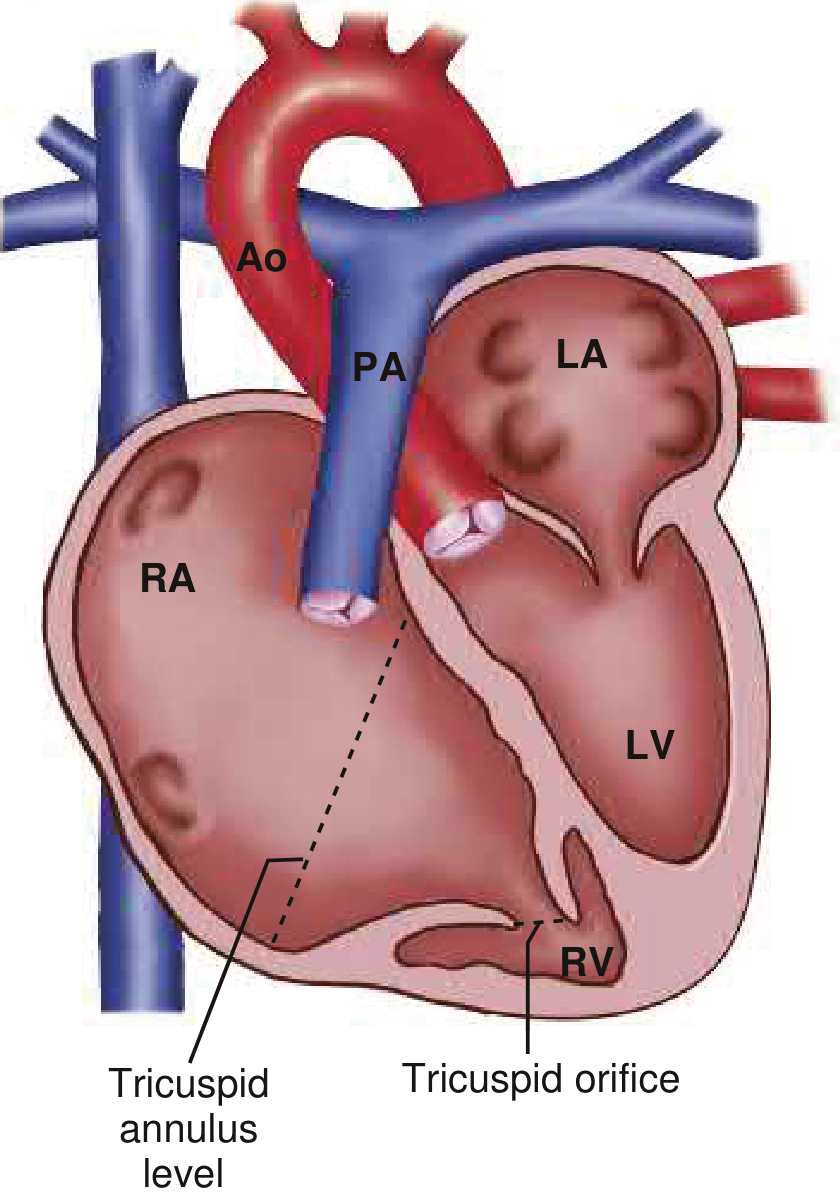
Diagram: The tricuspid orifice is displaced apically into the RV. The true annulus level is at the AV groove, leaving a large "atrialized" RV between them. — Braunwald's Heart Disease
Plain Chest Radiograph (CXR)
The CXR is often the first imaging modality and has classic findings:
| Feature | Description |
|---|---|
| Massive cardiomegaly | Markedly elevated cardiothoracic ratio (often ≥0.65) |
| "Box-shaped" / globular heart | Characteristic silhouette; smooth, rounded borders |
| Prominent right heart border | Due to massive right atrial (RA) enlargement |
| Decreased pulmonary vascularity | Oligemic lung fields (reduced pulmonary blood flow) |
| Small aortic knob | Low cardiac output, reduced systemic flow |
| Small pulmonary trunk shadow | Compared to the giant cardiac silhouette |

AP CXR: Massive cardiomegaly with rounded right heart border (RA enlargement), oligemic lungs, and small aortic knuckle — classic Ebstein.
A cardiothoracic ratio ≥0.65 is a prognostic marker for decreased survival in unrepaired cases.
Echocardiography (Primary Diagnostic Tool)
Echocardiography is the cornerstone of diagnosis and assessment:
- Apical displacement of the septal tricuspid leaflet >8 mm/m² from the AV junction (or >20 mm absolute in adults) — diagnostic criterion
- The inferior and occasionally anterior leaflets may also be displaced
- The anterior leaflet is elongated, "sail-like," and may be fenestrated or tethered
- Atrialized RV: the basal portion of the RV between the true AV groove and the displaced valve orifice behaves hemodynamically as part of the RA
- Tricuspid regurgitation: typically severe and eccentric
- ASD/PFO: present in the majority; direction of shunting (right-to-left = cyanosis) must be assessed with color Doppler
- TEE may be needed to fully characterize anterior leaflet distal tethering
Key echocardiographic imaging goals (Grainger & Allison's Diagnostic Radiology):
- Describe apical displacement of septal leaflet
- Assess mobility of anterosuperior and inferior leaflets
- Note eccentric coaptation
- Quantify tricuspid regurgitation
- Quantify RA dilation and size of atrialized RV
- Assess RV and LV volume, function, and mass
- Exclude RVOT obstruction
Cardiac MRI (CMR)
CMR is increasingly used for comprehensive functional assessment, especially pre-operatively:
- Quantifies degree of tricuspid valve displacement and rotation
- Measures RV volumes and systolic function (RVEF) — RV dysfunction predicts mortality and sustained VT
- Quantifies tricuspid regurgitation severity
- Assesses LV volumes (may be small due to interventricular septal shift)
- Calculates Qp:Qs ratio for atrial-level shunt quantification
- Detects LV non-compaction (an associated finding)
CT
CT is less commonly used but can characterize:
- Enlargement of the tricuspid annulus (see axial CT below)
- Overall cardiac chamber dimensions
- Associated anomalies (RVOT, pulmonary arteries)
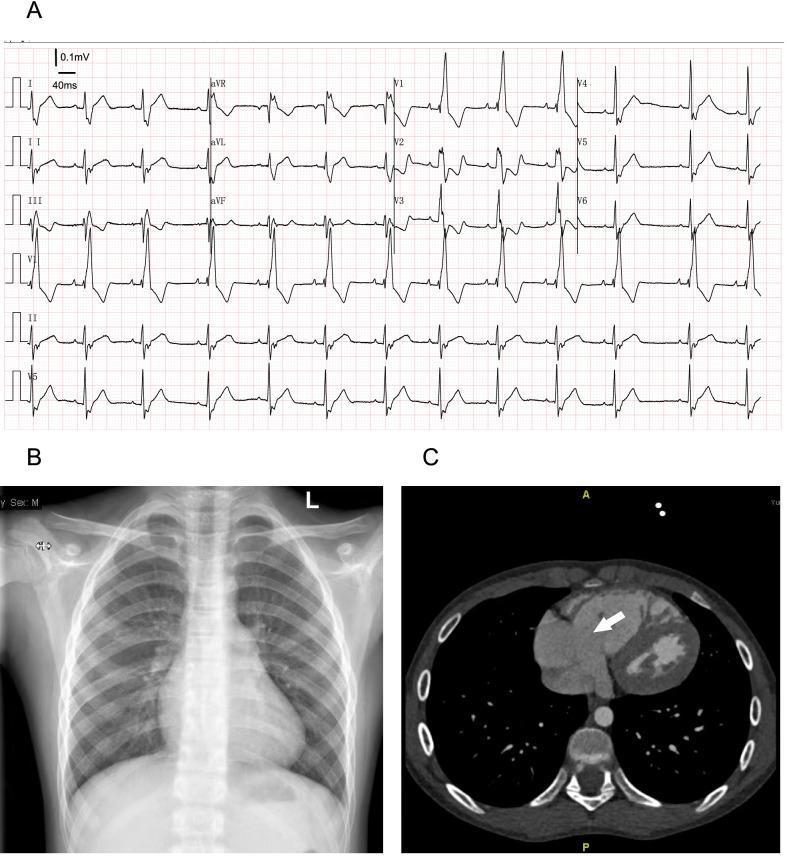
Panel B: CXR with right heart border enlargement (CTR ~0.5). Panel C: Axial CT — arrow points to enlarged tricuspid annulus. Panel A: ECG with RBBB pattern.
Associated Radiological/Imaging Findings
| Modality | Finding |
|---|---|
| ECG | Tall/peaked "Himalayan" P waves, prolonged PR, RBBB, delta waves (WPW), atrial flutter/fibrillation |
| CXR | Box-shaped cardiomegaly, oligemia, small aorta |
| Echo | Displaced septal leaflet, TR, atrialized RV, ASD |
| CMR | RV dysfunction, quantify TR, Qp:Qs |
| All | ASD/PFO, accessory pathways, pulmonary stenosis, VSD |
Key Numbers
- Diagnostic threshold: septal leaflet displacement >8 mm/m² (or >20 mm in adults)
- Incidence: 1 per 200,000 live births
- Poor prognosis markers on imaging: cardiothoracic ratio ≥0.65, RV/LV systolic dysfunction, severe TR
— Braunwald's Heart Disease, Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.