Diagnosis and management of hypertension
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertension"[MeSH Terms] AND "diagnosis" AND "management"
Finding Sources
Reading Article
PMID: 40815242
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
I now have comprehensive, well-sourced information from multiple authoritative textbooks plus the 2025 AHA/ACC guideline. Let me compile the full response.
Diagnosis and Management of Hypertension
Definition and Classification
Blood pressure (BP) in adults is classified using the 2017 ACC/AHA system, which the 2025 AHA/ACC guideline retires the 2017 document and updates:
| Category | Systolic (SBP) | Diastolic (DBP) | |
|---|---|---|---|
| Normal | <120 mmHg | and | <80 mmHg |
| Elevated | 120-129 mmHg | and | <80 mmHg |
| Stage 1 Hypertension | 130-139 mmHg | or | 80-89 mmHg |
| Stage 2 Hypertension | ≥140 mmHg | or | ≥90 mmHg |
CVD risk is directly related to BP in a continuous fashion with no true threshold - risk increases even below the hypertension cutoff. - Fuster and Hurst's The Heart, 15th Edition
Diagnosis
Accurate BP Measurement
- Measure with the patient at rest, sitting, legs uncrossed, bladder empty, in a comfortable temperature
- Average ≥2 readings on ≥2 separate occasions before diagnosing hypertension
- Exception: Hypertension may be diagnosed on a single reading if BP >180/120 mmHg or if target organ damage is present
- Exclude pseudohypertension in elderly patients with stiff, noncompressible vessels (Osler sign: palpable artery persisting after cuff inflation)
- Home and ambulatory BP monitoring correlate better with target organ damage than clinic readings - Washington Manual of Medical Therapeutics
Evaluation: Initial Workup
A thorough history, physical exam, and basic investigations are performed to:
- Confirm the diagnosis
- Identify secondary causes
- Assess cardiovascular risk and target organ damage
Investigations:
- Urinalysis and urine microalbumin/creatinine (renal damage)
- Serum creatinine/eGFR (renal function)
- Electrolytes (K+ low in hyperaldosteronism)
- Fasting glucose, HbA1c (metabolic syndrome, DM)
- Fasting lipid panel (cardiovascular risk)
- ECG (LVH, arrhythmias)
- Thyroid function (secondary cause)
Secondary Hypertension
Screen especially in young patients, resistant hypertension, or atypical presentations:
| Cause | Clues |
|---|---|
| Renal artery stenosis | Abdominal bruit, flash pulmonary edema, worsening renal function on ACEi |
| Primary aldosteronism | Hypokalemia, elevated aldosterone/renin ratio |
| Pheochromocytoma | Episodic headache, palpitations, diaphoresis |
| Obstructive sleep apnea | Obesity, daytime somnolence, resistant HTN |
| Coarctation of aorta | Radio-femoral delay, reduced BP in legs |
| Cushing's syndrome | Central obesity, striae, hyperglycemia |
| Thyroid disease | Tachycardia/bradycardia, weight changes |
Pathophysiology
Hypertension arises from increased cardiac output, increased peripheral vascular resistance, or both. Renal mechanisms are central:
- Salt-sensitive hypertension: Reduced nephron mass, decreased glomerular filtration coefficient, or increased distal tubule sodium reabsorption - all shift the pressure-natriuresis curve rightward
- Salt-insensitive hypertension: Increased preglomerular resistance (e.g., renal artery stenosis) causes a parallel shift in the pressure-natriuresis relationship - Brenner and Rector's The Kidney
Key contributing factors:
- Excess sodium intake - higher dietary sodium and sodium/potassium ratios are associated with higher BP (INTERMAP data)
- Physical inactivity - risk of hypertension is dose-dependently reduced ~6% per 10 METs-hr/week of leisure activity
- Obesity - visceral adipocytes generate pro-inflammatory cytokines promoting vascular disease
- Social determinants - income, education, access to care; hypertension is more prevalent and harder to control in Black Americans - Fuster and Hurst's The Heart, 15th Edition
Management
Treatment Goals
- Target BP <130/80 mmHg for most patients
- The primary driver of cardiovascular risk reduction is the amount of BP reduction, not the specific drug class chosen
Lifestyle Modifications (First-line for all patients)
| Modification | Approximate SBP Reduction |
|---|---|
| Weight reduction (per 10-kg loss) | 5-20 mmHg |
| DASH diet | 8-14 mmHg |
| Dietary sodium reduction (<2 g/day) | 2-8 mmHg |
| Physical activity (150 min/week) | 4-9 mmHg |
| Alcohol moderation (<2 drinks/day) | 2-4 mmHg |
- Washington Manual of Medical Therapeutics
Most patients with Stage 1 hypertension without high cardiovascular risk should have a trial of lifestyle changes (approx. 1 month) before starting pharmacotherapy. Stage 2 hypertension or high-risk patients should start drugs sooner.
Pharmacologic Therapy
Drug classes and key points:
1. Thiazide Diuretics (e.g., hydrochlorothiazide, chlorthalidone)
- First-line for most patients
- Especially effective in Black patients and elderly
- Side effects: hypokalemia, hyponatremia, hyperuricemia, hyperglycemia, hyperlipidemia
- Reduce urinary calcium excretion (protective against fractures in women)
2. ACE Inhibitors (e.g., ramipril, lisinopril)
- Preferred in: heart failure, CKD with proteinuria, post-MI, diabetes, high renin states
- Reduce complications beyond BP reduction (HOPE trial: reduced MI, stroke, death)
- Side effects: dry cough (up to 20%), angioedema, hyperkalemia, worsening renal function in bilateral renal artery stenosis
- Contraindicated in pregnancy (teratogenic)
- Do not combine with ARBs (increased vascular events and renal dysfunction)
3. Angiotensin Receptor Blockers (ARBs) (e.g., losartan, valsartan)
- Alternative to ACEi, especially in ACEi-intolerant patients (e.g., cough)
- Useful in heart failure, CKD
- Side effects: rare angioedema, rash
- Contraindicated in pregnancy
4. Calcium Channel Blockers (CCBs)
- Dihydropyridines (e.g., amlodipine, nifedipine): cause peripheral vasodilation; effective in Black patients; side effects: edema, flushing, headache
- Non-dihydropyridines (verapamil, diltiazem): negative chronotropes; useful in AF; side effects: constipation (verapamil), heart block; avoid in HF with reduced EF
- No adverse effects on glucose, lipids, or electrolytes
5. Beta-Blockers (e.g., metoprolol, carvedilol, atenolol)
- Preferred in: ischemic heart disease, post-MI, heart failure with reduced EF, AF rate control
- Not first-line for uncomplicated hypertension (less effective for stroke prevention)
- Side effects: bradycardia, fatigue, sexual dysfunction, masking hypoglycemia, bronchospasm
- Avoid in asthma/COPD; avoid atenolol in pregnancy (fetal growth restriction risk)
- Abrupt discontinuation can trigger rebound hypertension (withdrawal syndrome within 24-72 hours); serious complications include stroke, MI, encephalopathy
6. ARNI (Sacubitril-Valsartan)
- Particularly useful in heart failure; reduces all-cause mortality vs enalapril
- Do not administer within 36 hours of switching to/from ACEi
- Contraindicated with aliskiren in diabetics or eGFR <60
7. Direct Renin Inhibitor (aliskiren)
- Used solely for hypertension
- Contraindicated in combination with ACEi/ARBs in diabetic patients
8. Alpha-Blockers, Central Agents (e.g., clonidine, methyldopa)
- Clonidine: reserved for resistant hypertension; rebound hypertension on abrupt withdrawal
- Methyldopa: safe in pregnancy (first-line)
Special Populations
Compelling indications and preferred agents:
| Condition | Preferred Drug(s) |
|---|---|
| Heart failure (HFrEF) | ACEi/ARB, beta-blocker, diuretic, MRA |
| HFpEF with volume overload | Diuretics; ACEi/ARB for LVH regression |
| Post-MI | Beta-blocker, ACEi |
| CKD with proteinuria | ACEi or ARB |
| Diabetes | ACEi or ARB (reduce proteinuria) |
| Black patients | Thiazides and CCBs are especially effective |
| Pregnancy | Labetalol, nifedipine, or methyldopa |
| PAD | ACEi beneficial; beta-blockers safe (do not worsen claudication) |
Hypertension in Pregnancy:
- Preeclampsia: New-onset HTN after 20 weeks + proteinuria (or end-organ features)
- Eclampsia: Preeclampsia + generalized seizures
- Treat when SBP ≥160 or DBP ≥100 mmHg in pregnancy
- First-line: labetalol, nifedipine, methyldopa
- Avoid: ACEi, ARBs (teratogenic), atenolol
- Washington Manual of Medical Therapeutics
Hypertensive Urgency and Emergency
| Feature | Urgency | Emergency |
|---|---|---|
| BP threshold | ≥180/110 mmHg | ≥180/110 mmHg (may be higher) |
| End-organ damage | Absent | Present |
| Symptoms | Asymptomatic or vague | Headache, vision changes, dyspnea, chest pain, altered mentation, seizures |
| Setting | Outpatient | Emergency room / ICU |
| Route of treatment | Oral | IV |
| Rate of BP reduction | Gradual (hours to days) | Controlled reduction over minutes-hours; avoid overly rapid drops (risk of ischemia) |
Hypertensive urgency: Restart/intensify oral agents; schedule prompt follow-up. Rapid reductions risk precipitating target organ ischemia.
Hypertensive emergency - common presentations:
- Hypertensive encephalopathy (obtundation, visual disturbances, papilledema, seizures, posterior leukoencephalopathy on MRI - no focal neurologic signs)
- Acute left ventricular failure / pulmonary edema
- Acute coronary syndrome
- Aortic dissection
- Eclampsia
- Pheochromocytoma crisis
IV agents used in hypertensive emergencies: labetalol, nicardipine, clevidipine, nitroprusside, nitroglycerin, hydralazine (eclampsia), phentolamine (pheochromocytoma)
Note: Previously used sublingual nifedipine is no longer recommended - it was associated with acute coronary events and ischemic strokes. - Swanson's Family Medicine Review
Resistant Hypertension
Defined as BP above goal despite optimal doses of 3 antihypertensive agents of different classes (including a diuretic), or BP requiring ≥4 agents to be controlled.
- Screen for secondary causes
- Assess medication adherence and white coat effect
- 42% of treatment-resistant hypertensive adults are physically inactive
- Additional agents: mineralocorticoid receptor antagonists (spironolactone), alpha-blockers, direct vasodilators
Key 2025 Guideline Update
The 2025 AHA/ACC/AANP et al. Guideline (PMID: 40815242) represents the most current comprehensive update, replacing the 2017 guideline. It is described as a "living document" incorporating evidence through 2024. Key areas include updated BP classification, treatment thresholds, lifestyle intervention evidence, and special population guidance. Note: an erratum was published (PMID: 42300826).
The Hypertension Canada 2025 guideline for primary care (PMID: 40419299) was also published in May 2025, offering a complementary primary care-focused perspective.
Sources:
- Fuster and Hurst's The Heart, 15th Edition - Classification, epidemiology, CVD risk, pathophysiology, lifestyle therapy
- Washington Manual of Medical Therapeutics - Diagnosis, medications, special populations, pregnancy
- Harrison's Principles of Internal Medicine, 22E (2025) - Race/sex disparities, hypertensive urgencies/emergencies
- Goldman-Cecil Medicine - Hypertensive emergency/urgency definition, clinical features, treatment
- Brenner and Rector's The Kidney - Renal mechanisms of hypertension
Diagnosis and management of hypertension
Reading File
Finding Sources
Finding Sources
Searching PubMed
"hypertension"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Finding Sources
Searching PubMed
"hypertension"[MeSH Terms] AND "guideline"[pt]
Reading File
Reading Article
PMID: 39210715
Loading Image
Reading File
Reading File
Excellent content from Harrison's. I now have comprehensive material covering all major aspects. Let me compile the full, detailed answer.
Diagnosis and Management of Hypertension
1. Blood Pressure Measurement
Accurate measurement is the foundation of hypertension diagnosis. Errors are common in routine practice - SBP is overestimated by an average of ~7 mmHg in clinical settings, leading to a 15-20% overestimation of hypertension prevalence.
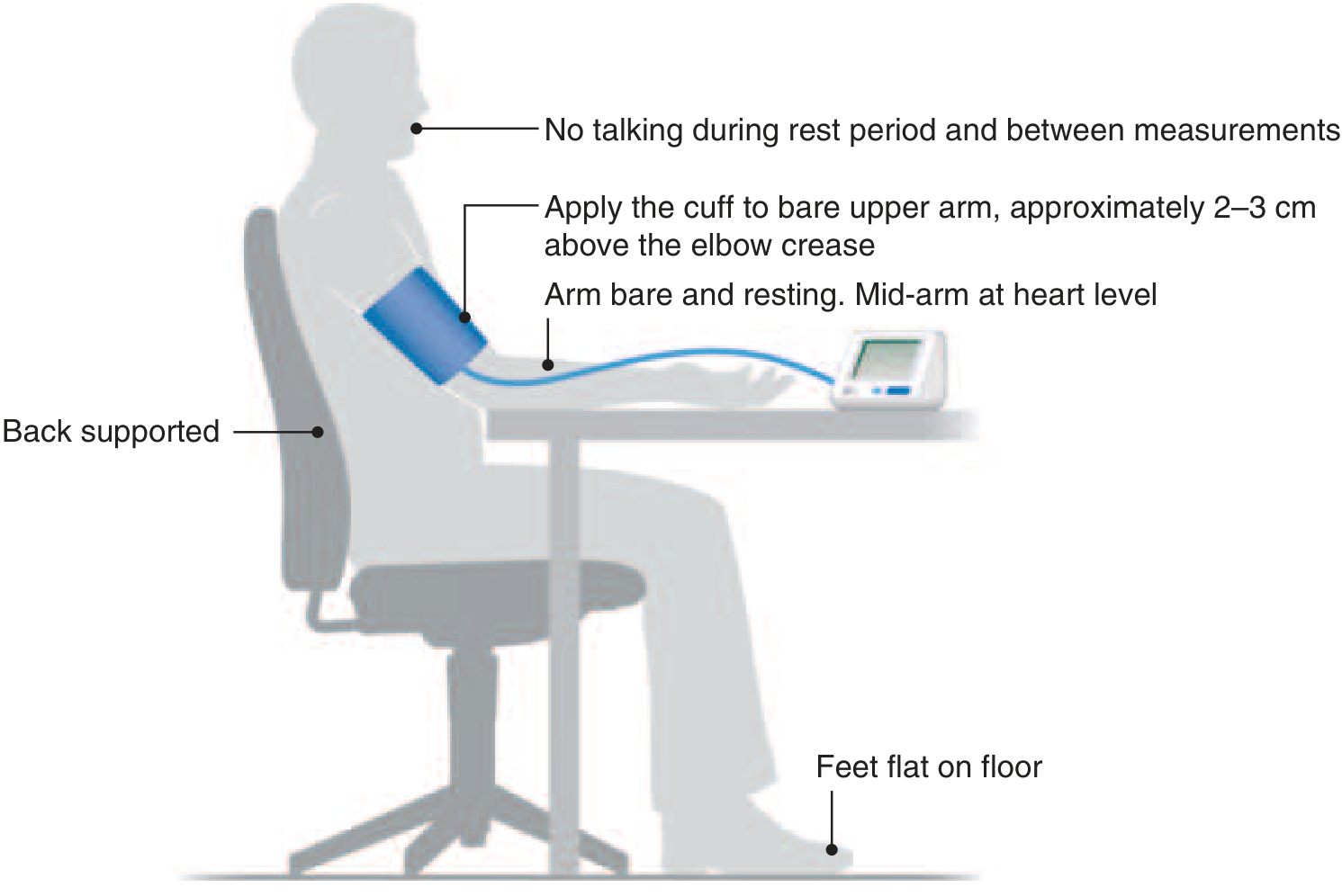
Key requirements for accurate measurement:
- Use a clinically validated oscillometric (automated) device
- Correct cuff size; apply to bare upper arm, 2-3 cm above the elbow crease
- Patient seated, back supported, feet flat, mid-arm at heart level
- No talking during rest period or between measurements
- Measure the arm with the highest reading at the first visit
- Average ≥2 readings at ≥2 separate visits before diagnosing hypertension
- When SBP and DBP fall in different categories, use the higher classification
2. Classification
The ACC/AHA classification system (the current standard, updated in the 2025 AHA/ACC guideline PMID 40811497 and the 2024 ESC guideline PMID 39210715):
| BP Category | Systolic (mmHg) | Diastolic (mmHg) | |
|---|---|---|---|
| Normal | <120 | and | <80 |
| Elevated | 120-129 | and | <80 |
| Stage 1 Hypertension | 130-139 | or | 80-89 |
| Stage 2 Hypertension | ≥140 | or | ≥90 |
When SBP and DBP fall in different categories, the higher category applies (e.g., 162/82 mmHg = Stage 2).
In children <13 years, classification is based on age-, sex-, and height-specific percentiles. Hypertension = average SBP/DBP at or above the 95th percentile, or ≥130/80 mmHg.
3. Out-of-Office BP Monitoring
Office readings alone can be misleading. Two important syndromes:
- White-coat hypertension: Office BP meets hypertension criteria, but out-of-office BP is normal (prevalence ~15-25%). CVD risk resembles those with normal BP. Manage with lifestyle changes and monitor carefully.
- Masked hypertension: Office BP appears controlled, but out-of-office BP is hypertensive (prevalence ~15-25%). CVD risk resembles sustained hypertension - treat with antihypertensives plus lifestyle changes.
Home BP targets (same thresholds as office): hypertension ≥130/80 mmHg, controlled <130/80 mmHg. Measure in morning and evening, 2-3 readings each, for 3 days before an office visit.
Ambulatory BP monitoring (ABPM) is the gold standard for out-of-office BP assessment.
- Harrison's Principles of Internal Medicine, 22nd Edition (2025)
4. Initial Evaluation
Purpose
- Confirm diagnosis and stage
- Identify secondary (reversible) causes
- Assess target organ damage (TOD)
- Quantify overall cardiovascular risk
History
- Duration of hypertension, prior BP levels, treatments
- Symptoms suggestive of secondary causes (episodic headache/palpitations/sweating = phaeochromocytoma; snoring/daytime somnolence = OSA)
- Family history of hypertension, CVD, renal disease
- Medications (NSAIDs, oral contraceptives, decongestants, stimulants, steroids, calcineurin inhibitors - all raise BP)
- Lifestyle: sodium intake, alcohol, exercise, weight, smoking
- Comorbidities: DM, CKD, sleep apnea, dyslipidemia
Physical Examination
- BP both arms (interarm difference >15 mmHg suggests coarctation or subclavian stenosis)
- Pulse, heart rate, BMI, waist circumference
- Fundoscopy (AV nicking, flame hemorrhages, papilledema = hypertensive retinopathy)
- Cardiovascular exam: S3/S4, displaced apex (LVH/HF)
- Abdomen: renal bruits (renovascular disease), palpable kidneys (polycystic kidney disease)
- Peripheral pulses, radio-femoral delay (coarctation)
- Signs of Cushing's, thyroid disease
Baseline Investigations
| Test | Purpose |
|---|---|
| Urinalysis + urine albumin/creatinine ratio | Proteinuria, hematuria (renal TOD) |
| Serum creatinine + eGFR | Renal function (TOD/secondary) |
| Serum electrolytes (K+, Na+) | Hypokalemia → hyperaldosteronism |
| Fasting glucose + HbA1c | Diabetes |
| Fasting lipid profile | Cardiovascular risk |
| ECG | LVH, arrhythmias, prior MI |
| Thyroid function (TSH) | Secondary cause |
| Full blood count | Polycythaemia |
Echocardiography is considered if LVH is suspected clinically.
5. Secondary Hypertension
Accounts for ~10% of all hypertension. Suspect in: young patients (<30 years), resistant hypertension, acute onset, hypokalaemia, asymmetric renal size, or abnormal urinalysis.
| Cause | Clues | Key Investigation |
|---|---|---|
| Renal parenchymal disease | Elevated creatinine, proteinuria, haematuria | eGFR, renal USS |
| Renovascular disease | Abdominal bruit, flash pulmonary oedema, worsening renal function on ACEi/ARB | Duplex USS, CT/MR angiography |
| Primary aldosteronism | Hypokalemia, adrenal incidentaloma | Aldosterone:renin ratio (ARR) |
| Phaeochromocytoma | Paroxysmal headache, palpitations, diaphoresis | 24h urinary metanephrines or plasma metanephrines |
| Obstructive sleep apnoea | Obesity, snoring, daytime somnolence | Polysomnography |
| Coarctation of aorta | Radio-femoral delay, lower BP in legs, rib notching on CXR | CT/MR aortography |
| Cushing's syndrome | Central obesity, moon face, striae, buffalo hump, hyperglycaemia | 24h urinary cortisol, overnight dexamethasone suppression test |
| Hypothyroidism/Hyperthyroidism | Bradycardia or tachycardia, weight changes | TSH |
| Primary hyperparathyroidism | Hypercalcaemia | Serum Ca2+, PTH |
6. Target Organ Damage (TOD)
Hypertension damages the heart, brain, kidneys, eyes, and peripheral vasculature:
| Organ | Manifestation |
|---|---|
| Heart | LVH, CAD, HF, AF |
| Brain | Stroke, TIA, vascular dementia, hypertensive encephalopathy |
| Kidneys | CKD, microalbuminuria, proteinuria |
| Eyes | Hypertensive retinopathy (AV nicking → flame haemorrhages → papilledema) |
| Vessels | Peripheral arterial disease, aortic aneurysm, aortic dissection |
7. Management
Treatment Goal
- <130/80 mmHg for most adults
- The magnitude of BP reduction, not the drug class chosen, is the primary driver of cardiovascular risk reduction
A. Lifestyle (Non-pharmacological) Modifications
First-line for ALL patients regardless of whether medication is needed. Can be sufficient to control Stage 1 hypertension in low-risk patients.
| Intervention | Expected SBP Reduction |
|---|---|
| Weight reduction (per 10 kg lost) | 5-20 mmHg |
| DASH diet | 8-14 mmHg |
| Dietary sodium reduction (<2 g/day) | 2-8 mmHg |
| Regular aerobic exercise (150 min/week) | 4-9 mmHg |
| Alcohol moderation (<2 drinks/day) | 2-4 mmHg |
| Potassium supplementation / salt substitution | ~4-5 mmHg |
The interventions show a linear dose-response, and combining multiple interventions (e.g., DASH + sodium restriction + weight loss) produces additive reductions. Non-pharmacological treatment also enhances the effect of antihypertensive medications. - Harrison's Principles of Internal Medicine, 22E (2025)
B. When to Start Pharmacotherapy
- Stage 1 (130-139/80-89 mmHg) with low CVD risk: lifestyle changes for 3-6 months first
- Stage 1 with established CVD, DM, CKD, or 10-year CVD risk ≥10%: start medication immediately alongside lifestyle
- Stage 2 (≥140/90 mmHg): initiate pharmacotherapy promptly, often with two drugs
- BP >180/120 mmHg with target organ damage: hypertensive emergency - IV treatment required
C. Drug Classes
Meta-analysis of 123 trials showed antihypertensive therapy reduces: major CVD by 20%, CHD by 17%, stroke by 27%, HF by 28%, and all-cause mortality by 13%. The five classes proven to prevent CVD are diuretics, beta-blockers, CCBs, ACEi, and ARBs - though in head-to-head RCTs, beta-blockers are inferior to the others (especially for stroke prevention).
1. Thiazide/Thiazide-like Diuretics
(e.g., chlorthalidone, hydrochlorothiazide, indapamide)
- Considered "best in class" for first-step antihypertensive therapy in meta-analyses
- Especially effective in Black patients and elderly
- Reduce urinary calcium excretion (fracture protection in women)
- Side effects: Hypokalemia, hyponatraemia, hyperuricaemia (gout), impaired glucose tolerance, hyperlipidaemia, erectile dysfunction
2. ACE Inhibitors (ACEi)
(e.g., ramipril, lisinopril, enalapril, perindopril)
- Preferred in: HF, post-MI, CKD with proteinuria, diabetes, renovascular hypertension (high-renin states), scleroderma renal crisis
- Reduce cardiovascular events beyond BP reduction (HOPE trial - ramipril reduced MI, stroke, death in high-risk patients without HF)
- Side effects: Dry cough (up to 20%), angioedema (<1%), hyperkalemia, worsening renal function in bilateral renal artery stenosis or severe renal insufficiency
- Contraindicated: Pregnancy (teratogenic), bilateral renal artery stenosis, hyperkalaemia
- Do NOT combine with ARBs (increased renal/vascular events)
3. Angiotensin Receptor Blockers (ARBs)
(e.g., losartan, valsartan, irbesartan, candesartan)
- Equivalent to ACEi in most indications; preferred in ACEi-intolerant patients (cough)
- Useful in HFrEF, CKD with proteinuria, post-MI
- Side effects: Rare angioedema, hyperkalaemia, worsening renal function
- Contraindicated: Pregnancy (teratogenic)
- Do NOT combine with ACEi
4. Calcium Channel Blockers (CCBs)
- Dihydropyridines (e.g., amlodipine, nifedipine, felodipine): peripheral vasodilators; good for stroke prevention; effective in Black patients and elderly
- Side effects: Peripheral oedema, flushing, headache, gingival hyperplasia
- Non-dihydropyridines (verapamil, diltiazem): also reduce heart rate; useful in AF/SVT rate control
- Side effects: Constipation (verapamil), bradycardia, heart block, nausea
- Avoid non-DHPs in HFrEF
- No adverse effect on glucose, lipids, or electrolytes
5. Beta-Blockers
(e.g., metoprolol succinate, carvedilol, bisoprolol, atenolol, labetalol)
- Not first-line for uncomplicated hypertension (inferior for stroke prevention in meta-analyses)
- Compelling indications: post-MI, HFrEF, stable angina, AF rate control, aortic aneurysm
- Side effects: Fatigue, bradycardia, bronchospasm, sexual dysfunction, cold extremities, masking of hypoglycaemia
- Avoid in: Asthma/reactive airway disease, heart block (>1st degree), cardiogenic shock
- Abrupt discontinuation causes rebound hypertension (worst with clonidine and beta-blockers) - taper when stopping; rebound can cause encephalopathy, stroke, MI
6. Mineralocorticoid Receptor Antagonists (MRAs)
(e.g., spironolactone, eplerenone)
- Especially useful in primary aldosteronism, resistant hypertension, HFrEF
- Spironolactone is most effective 4th-line agent in resistant hypertension (Pathway-2 trial)
- Side effects: Hyperkalaemia, gynaecomastia (spironolactone), menstrual irregularities
7. Other Classes
- Alpha-1 blockers (doxazosin): useful in BPH + hypertension; orthostatic hypotension risk
- Central alpha-2 agonists (clonidine, methyldopa): reserved for resistant hypertension or pregnancy (methyldopa); rebound syndrome on abrupt cessation
- Direct vasodilators (hydralazine, minoxidil): reserved for refractory cases; reflex tachycardia/fluid retention require co-medication
- ARNI (sacubitril-valsartan): approved for HFrEF; emerging data on BP reduction; do not use within 36 hours of switching to/from ACEi
- Direct renin inhibitor (aliskiren): do not combine with ACEi/ARBs in diabetics (FDA warning)
D. Initial Drug Selection Strategy
| Clinical Scenario | Preferred Agent(s) |
|---|---|
| Uncomplicated hypertension | Thiazide, CCB, ACEi, or ARB |
| Black race (without DM/CKD) | Thiazide or CCB (ACEi/ARBs less effective as monotherapy) |
| HF with reduced EF | ACEi or ARB + beta-blocker + MRA + diuretic |
| Post-MI | Beta-blocker + ACEi |
| CKD with proteinuria | ACEi or ARB |
| Diabetes | ACEi or ARB (reduce diabetic nephropathy) |
| Stable angina | Beta-blocker or CCB |
| AF (rate control) | Beta-blocker or non-DHP CCB |
| Primary aldosteronism | MRA (spironolactone) |
| Benign prostatic hyperplasia | Alpha-blocker |
| Pregnancy | Labetalol, nifedipine, or methyldopa |
Rational combination therapy: Most patients with Stage 2 hypertension require ≥2 agents. Preferred combinations: ACEi (or ARB) + CCB, or ACEi (or ARB) + thiazide. Adding a CCB to a RAAS blocker is preferred over RAAS + diuretic for most patients.
8. Resistant Hypertension
Defined as BP above goal despite the optimal doses of 3 antihypertensive agents of different classes (including a diuretic), or requiring ≥4 agents to be controlled.
Approach:
- Confirm true resistance (exclude pseudoresistance: white-coat effect, poor adherence, inaccurate measurement)
- Optimize lifestyle changes
- Review for secondary causes (especially primary aldosteronism and OSA)
- Review drug interactions and interfering substances (NSAIDs, stimulants, liquorice)
- Add a 4th agent: spironolactone is most evidence-based 4th-line agent (Pathway-2 trial)
- Consider referral to a hypertension specialist
9. Special Populations
Hypertension in Pregnancy
- Preeclampsia: New-onset hypertension after 20 weeks' gestation + proteinuria (or end-organ features: platelets <100,000, creatinine >1.1 mg/dL, LFTs >2x normal, pulmonary oedema, cerebral/visual symptoms)
- Eclampsia: Above + generalised seizures
- Chronic hypertension: Present before pregnancy or <20 weeks' gestation
- Gestational hypertension: BP ≥140/90 after 20 weeks without proteinuria/end-organ features
Treatment: Treat when SBP ≥160 or DBP ≥100 mmHg
- Safe first-line: Labetalol, nifedipine (oral), methyldopa
- Avoid: ACEi and ARBs (teratogenic - fetal renal toxicity, oligohydramnios, skull hypoplasia, death); atenolol (fetal growth restriction)
- Magnesium sulphate is used for seizure prophylaxis/treatment in eclampsia
- Washington Manual of Medical Therapeutics
Elderly Patients
- Higher prevalence of isolated systolic hypertension
- Higher prevalence of orthostatic hypotension - check standing BP
- Watch for pseudohypertension (Osler's sign: stiff arteries maintain palpable pulse after cuff inflation)
- Start drugs at lower doses; titrate slowly
- Thiazides and CCBs are effective; avoid alpha-blockers as first-line (fall risk)
- Target <130/80 in most elderly, but individualise in frail patients
Racial Disparities
Black Americans have higher prevalence, earlier onset, and worse outcomes from hypertension. Thiazides and CCBs are particularly effective; many require triple therapy. ACEi/ARBs are less effective as monotherapy in this population. Disparities are largely driven by social determinants of health rather than genetics. - Harrison's, 22E (2025)
10. Hypertensive Urgency and Emergency
| Feature | Urgency | Emergency |
|---|---|---|
| BP threshold | ≥180/110-120 mmHg | Usually ≥180/110-120 mmHg |
| Target organ damage | Absent | Present (new/worsening) |
| Symptoms | Asymptomatic or mild headache | Neurological (encephalopathy, seizures), chest pain, dyspnoea, visual disturbance, oliguria |
| Management setting | Outpatient | Emergency department / ICU |
| Treatment route | Oral | IV |
| Speed of BP reduction | Gradual over hours-days | Controlled reduction over minutes-hours |
Hypertensive Urgency
- Restart discontinued medications or intensify oral regimen
- Rapid BP reduction risks precipitating target organ ischaemia (cerebral, coronary, renal)
- Schedule close outpatient follow-up within 1-3 days
- Sublingual nifedipine is contraindicated - associated with acute coronary events and ischaemic strokes
Hypertensive Emergency - Key Presentations
| Presentation | Notes |
|---|---|
| Hypertensive encephalopathy | Headache, obtundation, visual disturbance, seizures, papilloedema; posterior reversible encephalopathy syndrome (PRES) on MRI; no focal deficits |
| Acute ischaemic stroke | BP lowering is cautious - only treat if BP >220/120 (or >185/110 if thrombolysis planned) |
| Haemorrhagic stroke | Target SBP <140 mmHg in first 6 hours |
| Acute LV failure / pulmonary oedema | IV nitrates + loop diuretics + IV ACEi (enalaprilat) |
| Acute aortic dissection | Most urgent scenario: target SBP <120 mmHg rapidly; IV labetalol or esmolol + nitroprusside |
| ACS/STEMI | IV nitrates, beta-blockers, heparin |
| Eclampsia | IV labetalol or hydralazine; MgSO4 for seizures |
| Phaeochromocytoma crisis | Phentolamine (alpha-blocker) first; then beta-blocker - never start beta-blocker first (paradoxical hypertension from unopposed alpha-stimulation) |
IV agents used in hypertensive emergencies:
| Drug | Onset | Indication |
|---|---|---|
| Labetalol (IV) | 5-10 min | Most emergencies, aortic dissection, eclampsia |
| Nicardipine (IV) | 5-15 min | Most emergencies, post-operative |
| Clevidipine (IV) | 2-4 min | Perioperative, general emergencies |
| Sodium nitroprusside | Seconds | Severe emergencies, aortic dissection (+ beta-blocker) |
| Nitroglycerin (IV) | 2-5 min | ACS, acute pulmonary oedema |
| Esmolol (IV) | 1-2 min | Aortic dissection, perioperative |
| Phentolamine | 1-2 min | Phaeochromocytoma, MAOI interactions, cocaine |
| Hydralazine (IV) | 10-30 min | Eclampsia |
- Goldman-Cecil Medicine; Harrison's Principles of Internal Medicine, 22E (2025)
11. Follow-up and Monitoring
- Reassess BP at 1 month after initiating or changing therapy
- Once controlled, follow-up every 3-6 months
- Monitor for side effects and adherence at each visit
- Annual: electrolytes, creatinine, urinalysis
- Reinforce lifestyle modifications at every visit
- Consider home BP monitoring to improve adherence and optimise titration
Current Guideline Summary
The 2025 AHA/ACC/AANP et al. Guideline (PMID: 40811497) is the current U.S. standard, replacing the 2017 guideline. It is designed as a "living document" incorporating evidence up to mid-2024. The 2024 ESC Guideline (PMID: 39210715) is the European counterpart. Both emphasise accurate BP measurement, lifestyle changes, and individualised pharmacotherapy with a goal of <130/80 mmHg for most patients.
Primary sources:
- Harrison's Principles of Internal Medicine, 22nd Edition (2025) - Classification, measurement, pharmacotherapy, special populations, emergencies
- Washington Manual of Medical Therapeutics - Drug classes, lifestyle modifications, pregnancy
- Goldman-Cecil Medicine - Hypertensive urgency/emergency management
- Fuster and Hurst's The Heart, 15th Edition - BP classification, pathophysiology, CVD risk
This is a shared conversation. Sign in to Orris to start your own chat.