Ebstein anomoly radiology
Reading File
Finding Sources
Searching Images
Ebstein anomaly radiology chest X-ray echocardiogram
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a comprehensive overview of Ebstein anomaly radiology, drawn from Grainger & Allison's Diagnostic Radiology, Braunwald's Heart Disease, and supporting literature.
Ebstein Anomaly — Radiology
Anatomy & Pathology (Brief Review)
Ebstein anomaly is a congenital tricuspid valve and right ventricular defect defined by:
- Failure of delamination of tricuspid leaflets from the RV endocardium
- Apical displacement of the septal (and sometimes inferior) tricuspid leaflet from the AV junction — diagnostic threshold: >8 mm/m² or >20 mm displacement in adults
- "Atrialized" RV — the proximal RV is incorporated into the right atrium, creating a large, thin-walled chamber
- Sail-like, redundant anterior leaflet — may be fenestrated or tethered
- Dilation of the right AV junction; variable RV myopathic change
- Commonly associated with ASD/PFO, accessory pathways (WPW), pulmonary stenosis/atresia
Chest Radiograph (CXR)
Classic appearance:
| Feature | Finding |
|---|---|
| Heart size | Massive cardiomegaly ("box-shaped" or globular heart) |
| Right heart border | Markedly prominent, rounded — due to severe RA + atrialized RV enlargement |
| Pulmonary vascularity | Decreased (oligemic lung fields) due to reduced pulmonary flow ± right-to-left shunt |
| Aortic knob | Small / inconspicuous |
| Pulmonary trunk | Small shadow |
The cardiothoracic ratio ≥0.65 is associated with worse prognosis (increased mortality from biventricular failure or sudden death).
CXR Example:

AP CXR: Massive cardiomegaly with globular shape, prominent right atrial border, and decreased pulmonary vascularity — classic for Ebstein anomaly.
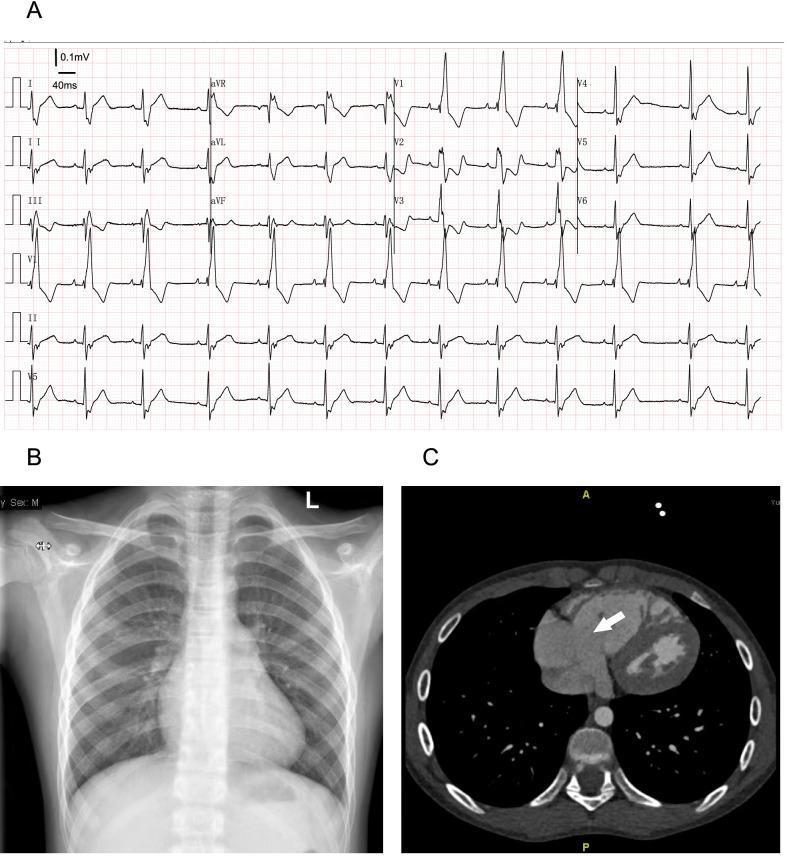
Panel A: ECG showing RBBB. Panel B: PA CXR with right heart enlargement. Panel C: Axial CT demonstrating enlarged tricuspid annulus (white arrow).
Echocardiography (Primary Modality)
Echocardiography is the first-line imaging modality and must characterize:
- Apical displacement of the septal tricuspid leaflet (>8 mm/m²) — the defining criterion
- Mobility of the anterosuperior and inferior leaflets
- Eccentric leaflet coaptation
- Tricuspid regurgitation — quantified by Doppler
- Right atrial dilation + size of the atrialized RV
- RV and LV volumes and systolic function
- Direction of flow across any PFO/ASD (right-to-left shunting causes cyanosis)
- RVOT obstruction
TEE may be needed to evaluate the anterior leaflet and its distal tethering, which can be distant from the probe.
Cardiac MRI (CMR)
CMR is used when echocardiography is insufficient and is particularly valuable for:
| Parameter | Role |
|---|---|
| Degree of TV displacement and rotation | Anatomic severity grading |
| Tricuspid regurgitation quantification | Regurgitant fraction |
| RV volumes and systolic function | Key prognostic marker |
| LV volumes (often small) | Biventricular assessment |
| Cardiac output | Often reduced |
| Qp:Qs | Quantifies intracardiac shunt |
CMR-derived RV and LV systolic dysfunction independently predict mortality and sustained VT.
CT
CT demonstrates:
- Marked enlargement of the tricuspid annulus (see Panel C above)
- Right atrial and atrialized RV dilation
- Useful for pre-operative anatomic planning and when CMR is contraindicated
Key Imaging Goals Summary
(from Grainger & Allison's Diagnostic Radiology)
- Describe apical displacement of the septal tricuspid leaflet
- Assess mobility of the anterosuperior and inferior leaflets
- Note eccentric coaptation
- Quantify tricuspid regurgitation
- Quantify RA dilation and size of the atrialized RV
- Assess RV and LV volume, function, and mass
- Quantify right-to-left shunting (Qp:Qs)
- Exclude RVOT obstruction
ECG Correlation
Though not imaging per se, the ECG often accompanies radiology workup:
- Tall, peaked "Himalayan" P waves (>5 mm) — RA enlargement
- Prolonged PR interval
- Short PR + delta wave — accessory pathway (WPW, Mahaim)
- Complete or incomplete RBBB
- RSR' in V1 — RV conduction delay
- Atrial flutter/fibrillation common
Sources: Grainger & Allison's Diagnostic Radiology; Braunwald's Heart Disease (10th ed.)
This is a shared conversation. Sign in to Orris to start your own chat.