Ebstein anomoly
Reading File
Finding Sources
Searching Images
Ebstein anomaly heart echocardiography diagram
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a comprehensive overview of Ebstein Anomaly, drawn from Braunwald's Heart Disease and Schwartz's Principles of Surgery:
Ebstein Anomaly
Definition & Anatomy
Ebstein anomaly is a rare congenital heart defect (1 in 200,000 live births; <1% of all CHD) characterized by apical displacement of the tricuspid valve leaflets — specifically the septal and posterior leaflets — from the AV junction into the right ventricle (RV). This results from failure of delamination of the tricuspid valve leaflets from the underlying RV endocardium during cardiac development.
Diagnostic criteria:
- Displacement of the septal leaflet insertion >8 mm/m² relative to the mitral valve annulus
- Maximum displacement >20 mm in adults
The anterior leaflet remains attached at the annulus but is abnormally elongated, fenestrated, and characteristically "sail-like." The RV is divided into two functional parts:
| Segment | Description |
|---|---|
| Atrialized RV | Proximal inlet portion between AV groove and displaced valve; thin, dilated, contracts paradoxically |
| Functional RV | Distal trabeculated/outlet portion; reduced effective size |
The RV is myopathic, and the tricuspid annulus and right atrium (RA) are markedly dilated.
Associated Anomalies
- ASD / PFO (most common) → right-to-left shunt, cyanosis
- Accessory pathways — WPW / Mahaim-type in ~15% → pre-excitation
- Pulmonary stenosis or atresia
- VSD, PDA, mitral valve disease
- Bicuspid aortic valve, subaortic stenosis, coarctation of the aorta
- Left ventricular non-compaction (concurrent RV myopathy)
- Ebstein-like anomaly is a common association in L-loop TGA
Pathophysiology
RV dysfunction arises from two mechanisms:
- Inflow obstruction at the atrialized ventricle → ineffective RV filling
- Tricuspid regurgitation (worsened by progressive annular dilatation) → volume overload and further ineffective filling
In severe neonatal cases, the large atrialized RV causes LV compression ("pancaked LV" on echo), impairing LV function. The absence of effective forward flow can produce functional pulmonary atresia, making the neonate ductus-dependent.
Clinical Features
Presentation is highly variable, reflecting the wide anatomic spectrum:
| Age Group | Presentation |
|---|---|
| In utero / Neonate | Hydrops, cardiomegaly, cyanosis, acidosis; may be lethal |
| Child | Cyanosis, heart failure, arrhythmia; average diagnosis in mid-teens |
| Adult | Often asymptomatic despite severe TR; exercise intolerance, fatigue, arrhythmia, paradoxical embolism |
Physical exam: jugular venous pressure is typically normal even with significant TR, due to the large, compliant RA and atrialized RV.
Diagnostic Findings
ECG:
- Peaked tall "Himalayan" P waves (>5 mm) — right atrial enlargement
- Prolonged PR interval OR short PR + delta wave (WPW)
- Incomplete or complete RBBB (RSR' in V1)
- Atrial flutter or fibrillation
Chest X-ray:
- Marked cardiomegaly — classic "box-shaped" or "wall-to-wall" heart
- Decreased pulmonary vascular markings
- Small aorta and pulmonary trunk shadow
Echocardiography (key diagnostic tool):
- Apical displacement of septal leaflet
- Atrialized RV
- TR quantification
- ASD/PFO with shunt direction
- Great Ormond Street (GOSE) score: area of RA + atrialized RV / area of RV + LA + LV
| GOSE Score | Ratio | Neonatal Mortality |
|---|---|---|
| 1 | <0.5 | 8% |
| 2 | 0.5–1.0 | 8% |
| 3 | 1.1–1.4 | 100% |
| 4 | >1.5 | 100% |
CMR: Quantifies RV/LV volumes, TR severity, cardiac output, Qp:Qs; RV/LV systolic dysfunction on CMR predicts mortality and sustained VT.
Echocardiographic Images
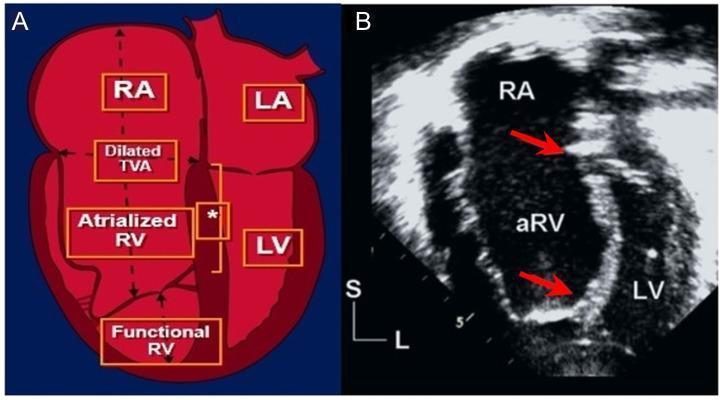
Apical 4-chamber echo in Ebstein anomaly: apical displacement of the septal tricuspid leaflet (red arrows = displacement index), atrialized RV (aRV), and true functional RV. Displacement index >8 mm/m² confirms diagnosis.
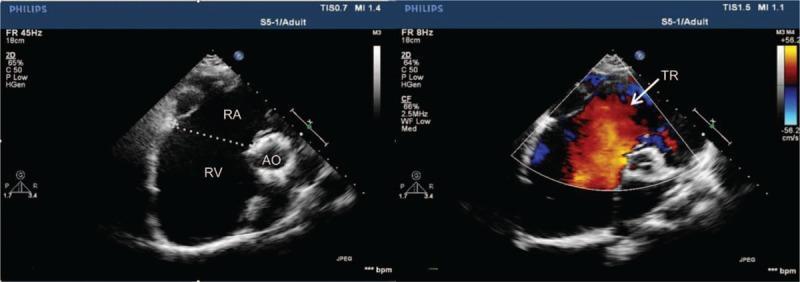
Color Doppler showing severe tricuspid regurgitation (TR jet) with markedly dilated RA and RV.
Long-term Outcomes (Unrepaired)
Natural history is driven by:
- Biventricular failure and sudden death
- Predictors of poor outcome: younger age at diagnosis, male sex, cardiothoracic ratio ≥0.65, severity of valve displacement
- Atrial tachyarrhythmia is the most common preceding event for adverse outcomes
- AVRT (due to accessory pathways) is the most common arrhythmia
- Multiple accessory pathways + AF → increased risk of sudden cardiac death
Management
Indications for surgery:
- Symptomatic heart failure (NYHA III–IV)
- Progressive cyanosis, arrhythmias, exercise intolerance
- Progressive RV enlargement or systolic dysfunction
- Paradoxical embolism or desaturation
Surgical options (Danielson procedure):
- Excision of redundant right atrial tissue
- Patch closure of ASD
- Plication of atrialized RV (obliterates the aneurysmal cavity)
- Posterior tricuspid annuloplasty
- Tricuspid valve repair (preferred if anterior leaflet is adequate) or replacement
- Electrophysiologic mapping + ablation for pre-excitation (ideally before surgery)
Neonatal Ebstein's anomaly is a distinct, high-risk entity. Severe cases may require conversion to single-ventricle physiology (Starnes procedure). Surgical outcomes in neonates have historically been poor.
Arrhythmia management: Catheter ablation is recommended before surgery for symptomatic pre-excitation or accessory pathways, as post-surgical access to right-sided pathways is limited.
Sources: Braunwald's Heart Disease, 2 Vol Set — Ch. 82 | Schwartz's Principles of Surgery 11th Ed. — Ch. 20
This is a shared conversation. Sign in to Orris to start your own chat.