Brachial plexus, ten mark laq , go
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I have all the content needed. Here is the full 10-mark long answer question response:
BRACHIAL PLEXUS - 10 Mark Long Answer
Definition and Formation
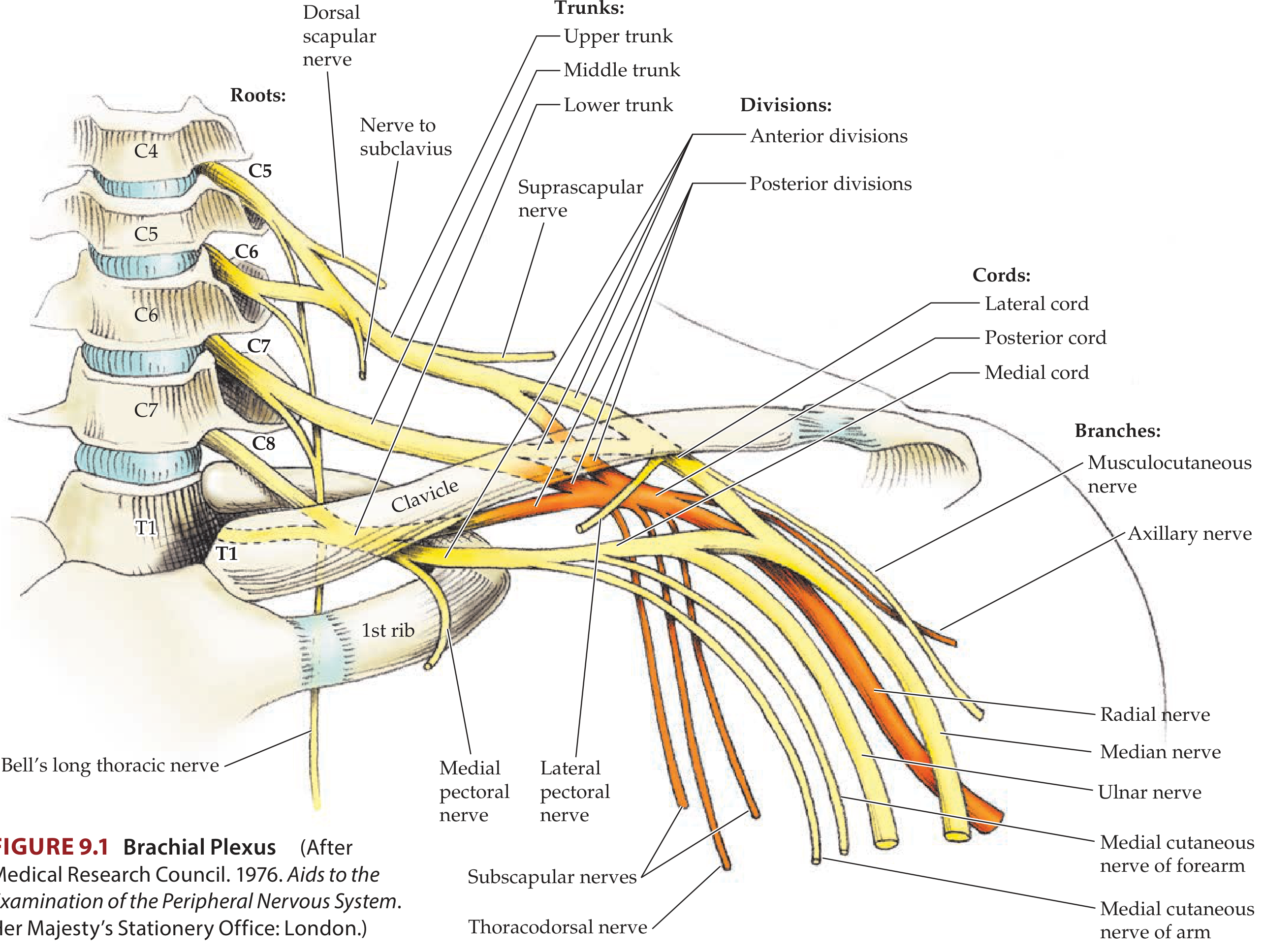
The brachial plexus is a somatic nerve plexus formed by the anterior rami (ventral rami) of C5, C6, C7, C8, and most of T1. It provides the entire motor and sensory innervation to the upper limb (except the skin of the medial arm, supplied by the intercostobrachial nerve, T2).
Mnemonic: Robert (Roots) Taylor (Trunks) Drinks (Divisions) Cold (Cords) Beer (Branches)
The plexus originates in the posterior triangle of the neck, passes over rib I between the anterior and middle scalene muscles, and enters the axilla.
Parts of the Brachial Plexus
1. ROOTS (C5-T1)
The roots are the anterior rami of C5-T1. They receive gray rami communicantes from the sympathetic trunk (carrying postganglionic sympathetic fibers). They pass between the anterior and middle scalene muscles, lying posterior to the subclavian artery.
Branches from roots:
- Dorsal scapular nerve (C5): innervates rhomboid major and minor
- Long thoracic nerve / Nerve of Bell (C5, C6, C7): innervates serratus anterior
- Contribution of C5 to the phrenic nerve
2. TRUNKS
Three trunks, located in the posterior triangle of the neck:
| Trunk | Formation | Position |
|---|---|---|
| Superior (Upper) trunk | Union of C5 + C6 roots | Superior |
| Middle trunk | Continuation of C7 root alone | Middle |
| Inferior (Lower) trunk | Union of C8 + T1 roots | Lies on rib I, posterior to subclavian artery |
Branches from trunks (only from superior trunk):
- Suprascapular nerve (C5, C6): passes through suprascapular foramen; innervates supraspinatus and infraspinatus
- Nerve to subclavius (C5, C6): innervates the subclavius muscle
3. DIVISIONS
Each trunk divides into an anterior and a posterior division (total of 6 divisions). No peripheral nerves arise directly from the divisions.
- Anterior divisions supply anterior (flexor) compartments
- Posterior divisions supply posterior (extensor) compartments
4. CORDS
Three cords, named for their relationship to the second part of the axillary artery:
| Cord | Formation | Position |
|---|---|---|
| Lateral cord | Anterior divisions of upper + middle trunks (C5-C7) | Lateral to axillary artery |
| Medial cord | Anterior division of lower trunk (C8-T1) | Medial to axillary artery |
| Posterior cord | All three posterior divisions (C5-T1) | Posterior to axillary artery |
5. BRANCHES (Terminal and Collateral)
Branches of the Lateral Cord:
- Lateral pectoral nerve (C5-C7): pectoralis major
- Musculocutaneous nerve (C5-C7): coracobrachialis, biceps brachii, brachialis; continues as lateral cutaneous nerve of forearm
- Lateral root of median nerve (C5-C7)
Branches of the Medial Cord:
- Medial pectoral nerve (C8-T1): pectoralis major and minor
- Medial cutaneous nerve of arm (C8-T1)
- Medial cutaneous nerve of forearm (C8-T1)
- Ulnar nerve (C7, C8, T1)
- Medial root of median nerve (C8-T1)
The lateral + medial roots join to form the median nerve (C5-T1). Together with musculocutaneous and ulnar nerves, they form an "M" shape over the axillary artery - a key surgical landmark.
Branches of the Posterior Cord (mnemonic: STAR or ARTS):
- Superior subscapular nerve (C5-C6): subscapularis
- Thoracodorsal nerve (C6-C8): latissimus dorsi
- Axillary nerve (C5-C6): deltoid, teres minor; sensory - regimental badge area
- Radial nerve (C5-C8, T1): all posterior compartment muscles of arm and forearm
- Inferior subscapular nerve (C5-C6): subscapularis, teres major
Relations in the Axilla
- Proximal plexus: posterior to subclavian artery in the neck
- In the axilla: cords surround the axillary artery (named lateral, medial, posterior accordingly)
Injuries to the Brachial Plexus
A. Erb's Palsy (Upper Trunk Injury - C5, C6)
Mechanism: Violent widening of the angle between neck and shoulder - birth trauma (shoulder dystocia), motorcycle accidents
Muscles affected: Deltoid, supraspinatus, infraspinatus, biceps, brachialis, brachioradialis, wrist extensors
Deformity: Classic "Waiter's tip" or "Bellman's tip" posture:
- Arm: adducted at shoulder, internally rotated
- Elbow: extended and pronated
- Wrist: flexed
Sensory loss: Lateral aspect of arm and forearm (C5, C6 dermatomes)
B. Klumpke's Palsy (Lower Trunk Injury - C8, T1)
Mechanism: Upward traction - grabbing a branch during a fall, forceps delivery pulling arm upward; also Pancoast tumor, thoracic outlet syndrome
Muscles affected: Intrinsic hand muscles (thenar, hypothenar, interossei, lumbricals) - all T1 + C8 supplied muscles
Deformity: "Claw hand" - hyperextension at MCPJs, flexion at IPJs
Sensory loss: Medial aspect of forearm and hand (ulnar border)
Additional feature: If T1 root is damaged proximal to the sympathetic trunk - Horner's syndrome (ptosis, miosis, anhidrosis, enophthalmos) due to involvement of preganglionic sympathetic fibers
C. Complete Plexus Palsy (All roots C5-T1)
Results in a completely flail, insensate upper extremity - seen in severe traction injuries or Pancoast tumor invading the entire plexus.
D. Injury to Specific Parts
| Level of Injury | Cause |
|---|---|
| Roots | Cervical spinal cord injury; violent direct pulling trauma |
| Trunks | Severe trauma to first rib |
| Divisions/Cords | Dislocation of glenohumeral joint |
Important Clinical Syndromes Related to Brachial Plexus
Thoracic Outlet Syndrome
Lower brachial plexus (C8-T1) compression between clavicle and first rib. May be exacerbated by raising and externally rotating the arm. Causes may include cervical rib. Investigations: EMG, X-ray (cervical rib). Treatment: shoulder-strengthening exercises or surgical decompression.
Pancoast Syndrome (Superior Sulcus Tumor)
Apical lung tumor (usually non-small cell carcinoma) invading lower brachial plexus. Features:
- Lower plexus signs (hand weakness, wasting)
- Horner's syndrome
- Hoarseness (recurrent laryngeal nerve involvement)
- Eventually entire plexus invasion - flail arm
Parsonage-Turner Syndrome (Brachial Neuritis / Brachial Plexitis)
Possibly inflammatory in origin. Presents with sudden severe burning shoulder/lateral neck pain, followed by weakness of plexus-innervated muscles. Self-limiting but recovery can take months.
Summary Table: Branches and Roots
| Nerve | Root Values | Key Muscles |
|---|---|---|
| Dorsal scapular | C5 | Rhomboids |
| Long thoracic (Bell's) | C5, C6, C7 | Serratus anterior |
| Suprascapular | C5, C6 | Supraspinatus, infraspinatus |
| Musculocutaneous | C5, C6, C7 | Biceps, brachialis, coracobrachialis |
| Axillary | C5, C6 | Deltoid, teres minor |
| Radial | C5-C8, T1 | All posterior compartment muscles |
| Median | C5-T1 | Thenar muscles, finger flexors |
| Ulnar | C7, C8, T1 | Intrinsic hand muscles |
Investigations for Brachial Plexus Injury
- Nerve conduction studies (NCS) - assess latency and conduction velocity
- Electromyography (EMG) - assesses muscle denervation
- MRI - visualize root avulsions and cord involvement
- X-ray/CT - look for associated fractures, cervical rib
Sources: Gray's Anatomy for Students (p. 858-867); Neuroanatomy through Clinical Cases, 3rd Ed. (p. 382)
What happened
You asked for a brachial plexus 10-mark long answer question, and I delivered it. Here's what the response covered:
- Definition & Formation - anterior rami C5-T1, origin in posterior triangle of neck
- Parts - the full RTDCB structure (Roots → Trunks → Divisions → Cords → Branches) with a detailed anatomy diagram
- All branches from each level - roots, trunks, lateral cord, medial cord, posterior cord with root values and muscles
- Injuries - Erb's palsy (C5-C6, waiter's tip), Klumpke's palsy (C8-T1, claw hand + Horner's), complete palsy
- Clinical syndromes - Thoracic outlet syndrome, Pancoast syndrome, Parsonage-Turner syndrome
- Summary table of all major nerves with root values
- Investigations - NCS, EMG, MRI, X-ray
Was there something specific you felt was missing, or did you mean something else by "what happened"?
Send the answer again please
BRACHIAL PLEXUS - 10 Mark Long Answer
Definition and Formation
The brachial plexus is a somatic nerve plexus formed by the anterior rami (ventral rami) of C5, C6, C7, C8, and most of T1. It provides the entire motor and sensory innervation to the upper limb (except the skin of the medial arm, supplied by the intercostobrachial nerve, T2).
Mnemonic: Robert (Roots) Taylor (Trunks) Drinks (Divisions) Cold (Cords) Beer (Branches)
The plexus originates in the posterior triangle of the neck, passes over rib I between the anterior and middle scalene muscles, and enters the axilla.
Parts of the Brachial Plexus
1. ROOTS (C5-T1)
The roots are the anterior rami of C5-T1. They receive gray rami communicantes from the sympathetic trunk (carrying postganglionic sympathetic fibers). They pass between the anterior and middle scalene muscles, lying posterior to the subclavian artery.
Branches from roots:
- Dorsal scapular nerve (C5): innervates rhomboid major and minor
- Long thoracic nerve / Nerve of Bell (C5, C6, C7): innervates serratus anterior
- Contribution of C5 to the phrenic nerve
2. TRUNKS
Three trunks, located in the posterior triangle of the neck:
| Trunk | Formation | Position |
|---|---|---|
| Superior (Upper) trunk | Union of C5 + C6 roots | Superior |
| Middle trunk | Continuation of C7 root alone | Middle |
| Inferior (Lower) trunk | Union of C8 + T1 roots | Lies on rib I, posterior to subclavian artery |
Branches from trunks (only from superior trunk):
- Suprascapular nerve (C5, C6): passes through suprascapular foramen; innervates supraspinatus and infraspinatus
- Nerve to subclavius (C5, C6): innervates the subclavius muscle
3. DIVISIONS
Each trunk divides into an anterior and a posterior division (total of 6 divisions). No peripheral nerves arise directly from the divisions.
- Anterior divisions supply anterior (flexor) compartments
- Posterior divisions supply posterior (extensor) compartments
4. CORDS
Three cords, named for their relationship to the second part of the axillary artery:
| Cord | Formation | Position |
|---|---|---|
| Lateral cord | Anterior divisions of upper + middle trunks (C5-C7) | Lateral to axillary artery |
| Medial cord | Anterior division of lower trunk (C8-T1) | Medial to axillary artery |
| Posterior cord | All three posterior divisions (C5-T1) | Posterior to axillary artery |
5. BRANCHES (Terminal and Collateral)
Branches of the Lateral Cord:
- Lateral pectoral nerve (C5-C7): pectoralis major
- Musculocutaneous nerve (C5-C7): coracobrachialis, biceps brachii, brachialis; continues as lateral cutaneous nerve of forearm
- Lateral root of median nerve (C5-C7)
Branches of the Medial Cord:
- Medial pectoral nerve (C8-T1): pectoralis major and minor
- Medial cutaneous nerve of arm (C8-T1)
- Medial cutaneous nerve of forearm (C8-T1)
- Ulnar nerve (C7, C8, T1)
- Medial root of median nerve (C8-T1)
The lateral + medial roots join to form the median nerve (C5-T1). Together with musculocutaneous and ulnar nerves, they form an "M" shape over the axillary artery - a key surgical landmark.
Branches of the Posterior Cord (mnemonic: STAR or ARTS):
- Superior subscapular nerve (C5-C6): subscapularis
- Thoracodorsal nerve (C6-C8): latissimus dorsi
- Axillary nerve (C5-C6): deltoid, teres minor; sensory - regimental badge area
- Radial nerve (C5-C8, T1): all posterior compartment muscles of arm and forearm
- Inferior subscapular nerve (C5-C6): subscapularis, teres major
Relations in the Axilla
- Proximal plexus: posterior to subclavian artery in the neck
- In the axilla: cords surround the axillary artery (named lateral, medial, posterior accordingly)
Injuries to the Brachial Plexus
A. Erb's Palsy (Upper Trunk Injury - C5, C6)
Mechanism: Violent widening of the angle between neck and shoulder - birth trauma (shoulder dystocia), motorcycle accidents
Muscles affected: Deltoid, supraspinatus, infraspinatus, biceps, brachialis, brachioradialis, wrist extensors
Deformity: Classic "Waiter's tip" or "Bellman's tip" posture:
- Arm: adducted at shoulder, internally rotated
- Elbow: extended and pronated
- Wrist: flexed
Sensory loss: Lateral aspect of arm and forearm (C5, C6 dermatomes)
B. Klumpke's Palsy (Lower Trunk Injury - C8, T1)
Mechanism: Upward traction - grabbing a branch during a fall, forceps delivery pulling arm upward; also Pancoast tumor, thoracic outlet syndrome
Muscles affected: Intrinsic hand muscles (thenar, hypothenar, interossei, lumbricals)
Deformity: "Claw hand" - hyperextension at MCPJs, flexion at IPJs
Sensory loss: Medial aspect of forearm and hand (ulnar border)
Additional feature: If T1 root is damaged proximal to the sympathetic trunk - Horner's syndrome (ptosis, miosis, anhidrosis, enophthalmos) due to involvement of preganglionic sympathetic fibers
C. Complete Plexus Palsy (All roots C5-T1)
Results in a completely flail, insensate upper extremity - seen in severe traction injuries or Pancoast tumor invading the entire plexus.
D. Level of Injury vs. Cause
| Level of Injury | Common Cause |
|---|---|
| Roots | Cervical spinal cord injury; violent direct pulling trauma |
| Trunks | Severe trauma to first rib |
| Divisions / Cords | Dislocation of glenohumeral joint |
Clinical Syndromes
Thoracic Outlet Syndrome
Lower brachial plexus (C8-T1) compression between clavicle and first rib. Exacerbated by raising and externally rotating the arm (may also reduce brachial pulse). Causes include cervical rib. Investigations: EMG, X-ray. Treatment: shoulder-strengthening exercises or surgical decompression.
Pancoast Syndrome (Superior Sulcus Tumor)
Apical lung tumor (usually non-small cell carcinoma) invading lower brachial plexus. Features:
- Lower plexus signs (hand weakness, wasting)
- Horner's syndrome
- Hoarseness (recurrent laryngeal nerve involvement)
- Eventually entire plexus invasion - flail arm
Parsonage-Turner Syndrome (Brachial Neuritis / Brachial Plexitis)
Possibly inflammatory in origin. Sudden severe burning shoulder/lateral neck pain followed by weakness of plexus-innervated muscles. Self-limiting but recovery can take months.
Summary Table: Major Branches
| Nerve | Root Values | Key Muscles |
|---|---|---|
| Dorsal scapular | C5 | Rhomboids |
| Long thoracic (Bell's) | C5, C6, C7 | Serratus anterior |
| Suprascapular | C5, C6 | Supraspinatus, infraspinatus |
| Musculocutaneous | C5, C6, C7 | Biceps, brachialis, coracobrachialis |
| Axillary | C5, C6 | Deltoid, teres minor |
| Radial | C5-C8, T1 | All posterior compartment muscles |
| Median | C5-T1 | Thenar muscles, finger flexors |
| Ulnar | C7, C8, T1 | Intrinsic hand muscles |
Investigations for Brachial Plexus Injury
- Nerve conduction studies (NCS) - assess latency and conduction velocity
- Electromyography (EMG) - assesses muscle denervation
- MRI - visualize root avulsions and cord involvement
- X-ray / CT - look for associated fractures, cervical rib
Sources: Gray's Anatomy for Students (p. 858-867); Neuroanatomy through Clinical Cases, 3rd Ed. (p. 382)
Instead of using grays for your answers can you use bd Chaurasia or vishram Singh
Finding Sources
Finding Sources
Unfortunately, BD Chaurasia and Vishram Singh are not available in the textbook library I have access to. The anatomy books currently in the library are:
- Gray's Anatomy for Students
- Netter's Atlas of Human Anatomy
- THIEME Atlas of Anatomy (General Anatomy and Musculoskeletal System)
- Color Atlas of Human Anatomy (Vols 1, 2, 3)
- Neuroanatomy through Clinical Cases
BD Chaurasia's Human Anatomy and Vishram Singh's Textbook of Anatomy are very popular Indian medical textbooks, but they are not part of this library's collection.
What I can do instead:
- Use Netter's Atlas + THIEME Atlas - these are also widely used and the content is clinically identical; I can rewrite the brachial plexus answer citing those
- Keep the answer as-is - the anatomical facts in the answer are the same as what BD Chaurasia teaches; only the source citation differs
- Use multiple available sources together for a richer answer
Which would you prefer?
This is a shared conversation. Sign in to Orris to start your own chat.