Distal tibia fracture nailing
Reading File
Finding Sources
Finding Sources
Searching PubMed
"distal tibia fracture" AND "intramedullary nail"
Reading File
Reading File
Searching PubMed
"distal tibia" AND "intramedullary nail" AND outcomes
Reading File
Finding Sources
Reading Article
PMID: 38997735
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive information. Let me compile the full answer.
Distal Tibia Fracture - Intramedullary Nailing
Treatment Algorithm
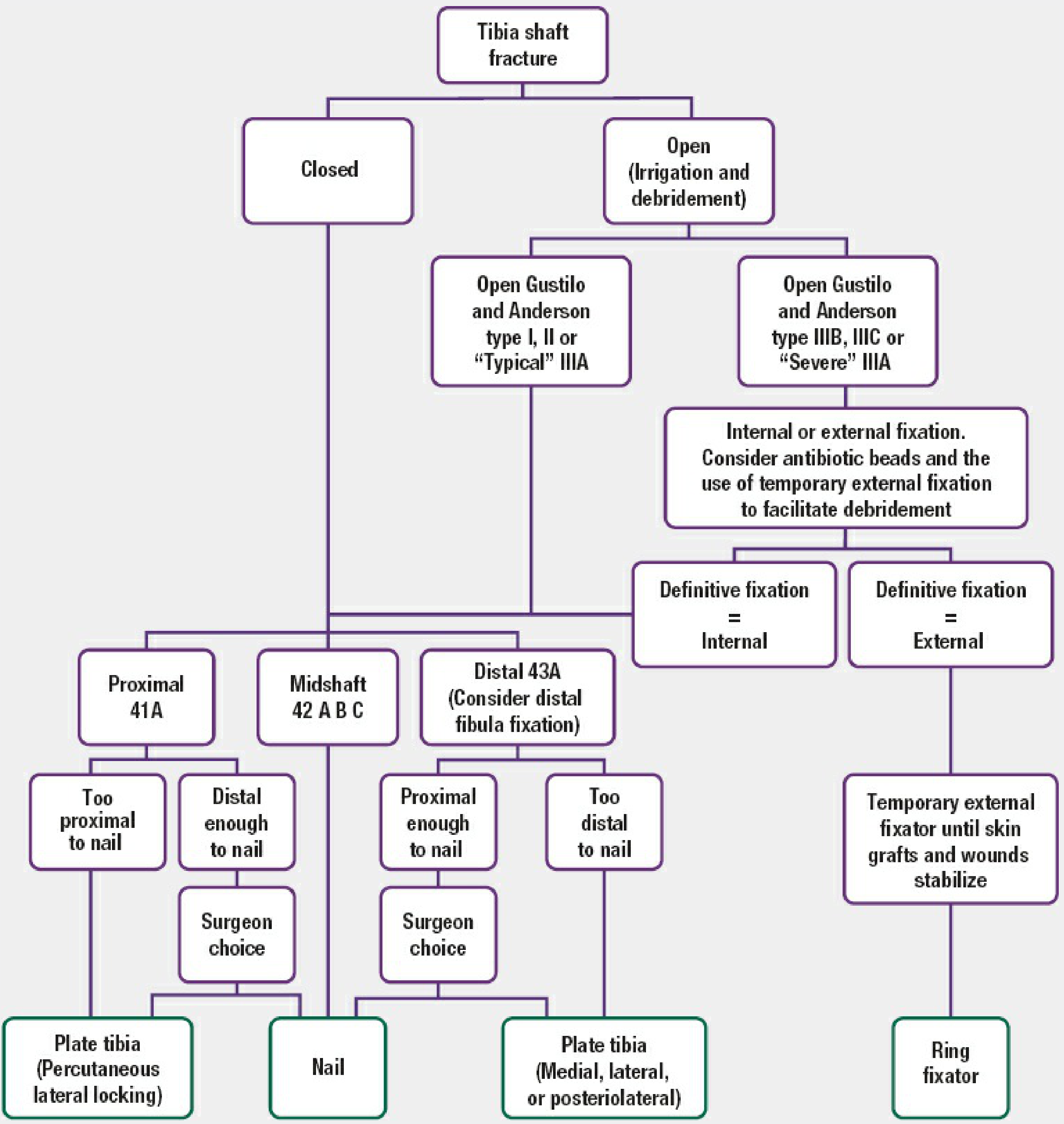
Indications and Decision-Making
Distal tibia fractures (OTA/AO 43A - extra-articular) are the primary candidates for IM nailing. The more distally the fracture extends, the harder it becomes to maintain a mechanically stable reduction.
Pre-op CT scan is mandatory for any distal fracture with radiographic concern about articular extension - to exclude a 43B1/C1 component. Failure to recognize nondisplaced articular fragments before nail insertion may result in displacement.
Contraindication to nailing: If preoperative measurements confirm that the distal locking screws cannot capture the distal tibial segment, plate fixation or a circular thin-wire frame is required instead. - Rockwood & Green's, p. 3255
Two distinct fracture mechanisms:
- Direct bending - transverse/oblique fractures, same-level fibular fractures, no intraarticular extension, more severe soft-tissue injury
- Torsional forces - spiral fractures, different-level fibular fracture, frequent intraarticular involvement of medial or posterior malleolus
Associated ankle injuries are present in ~20% of cases (pronation-eversion mechanisms, spiral fractures, proximal fibular fractures, or intact fibula should raise suspicion). - Campbell's Operative Orthopaedics, 15th Ed, p. 3355
Preoperative Planning
- Measure nail length using the tibial tubercle-medial malleolar distance (most accurate method)
- Nail diameter: measure the tibia at its narrowest point on lateral radiograph
- Use contralateral tibia radiographs for severely comminuted fractures
- The nail should be countersunk proximally with the distal end centered to slightly lateral in the distal epiphysis
- Account for potential impaction if dynamization is planned - choose length accordingly to prevent nail migration into ankle joint
- Reamed vs unreamed: Reamed nailing is preferred for fractures with minor soft-tissue injury; unreamed (8-10 mm nails) reserved for more extensive soft-tissue injury. Reaming allows larger, stronger implants. - Campbell's, p. 3356
Nail Design Considerations for Distal Fractures
- Two distal locking screws are required to prevent recurvatum deformity from rotation around a single distal screw
- Nails with more distally placed distal locking screws improve the ability to treat very distal tibial fractures
- Modern implant designs with tighter distal screw clusters have facilitated treatment without need for implant modification
- Some nails offer additional anteroposterior distal screw holes for improved distal purchase - Campbell's, p. 3356
Positioning
Option 1 - Fracture table:
- Calcaneal traction pin placed before positioning
- Patient supine, hip flexed 45°, knee flexed 90°
- Well-padded crossbar proximal to popliteal fossa
- Apply traction, confirm reduction under fluoroscopy, then release traction temporarily
- Reapply traction after entry portal is made
Option 2 - Standard radiolucent table (preferred):
- Patient supine, thigh over padded bolster
- Skilled assistant to help with fracture reduction and limb support
- A femoral distractor or two-pin external fixator can maintain reduction - Schanz pin 1 cm distal to knee (placed posteriorly to avoid nail path), second pin 1 cm proximal to ankle
- Campbell's TECHNIQUE 59.9, p. 3356-3357
The Core Challenge: Distal Fracture Malalignment
This is the most important technical problem in distal tibia nailing. The widened metaphysis allows the nail to track eccentrically, resulting in varus, valgus, or recurvatum deformity.
Prevention strategies (Rockwood & Green's Pitfalls Table):
| Pitfall | Prevention |
|---|---|
| Distal fracture malalignment | Lateral-to-center position on AP, centered on lateral with guidewire; Blocking (Poller) screws; Clamp the fracture; Temporary external fixation; Plate the coexisting distal fibula fracture first; Suprapatellar approach |
| Postoperative knee pain | Correct starting point; Bury nail proximally; Correct interlocking screw length; Blocking screws |
Reduction Techniques
Blocking (Poller) Screws
The most useful and widely cited technique for distal fractures. A screw (or K-wire/drill bit) is placed to force the reamer and nail into the correct path.
- Screw is placed on the concave side of the deformity (i.e., where you want to prevent the nail from going)
- For distal varus: place blocking screw in the lateral aspect of the distal fragment
- For distal valgus: place blocking screw medially
- Can be placed on the convex side if positioned at a distance from the fracture
- Screws can be left in place permanently to increase construct stability - particularly valuable in geriatric patients with wider tibiae and poor bone quality
- If malalignment has already occurred: remove the nail, insert blocking screws, ream a new pathway - Rockwood & Green's, p. 3221-3222
Other Reduction Adjuncts
- Percutaneous reduction clamps
- Provisional unicortical unlocked plating (unicortical screws ≤10 mm) - plate removed prior to wound closure in open fractures
- Suprapatellar (semi-extended) approach - reduces deforming pull of extensor mechanism
- Femoral distractor or temporary external fixator ("traveling traction")
- Intramedullary fracture reducer/"finger" device available in most nail sets
Fibula Fixation - Controversial but Often Useful
Fibula fixation is particularly useful for:
- Simple fibular fracture patterns
- Very distal tibial fracture patterns
Key data: In a study of 40 distal-fourth tibial fractures treated with locked IM nailing, 60% of unfixed same-level fibular fractures were malaligned, compared to 0% for intact fibulas and 0% for fibulas that were fixed. Unfixed fractures at a different level from the tibial fracture were all anatomically aligned. - Campbell's, p. 3355
Cautions:
- Malreduction of the fibula will prevent accurate tibial reduction - fix fibula first and verify alignment
- Fibular plating keeps the tibia out to length laterally but does not prevent varus collapse
- One study reported an 8-fold increased nonunion risk with combined fibula plating + tibia nailing; later studies have not confirmed this magnitude of risk
- Current position: Whether to fix the fibula in distal tibia fractures remains controversial - Rockwood & Green's, p. 3222
Locking and Dynamization
- All unstable fractures: minimum 2 screws distally and 2 proximally to maintain length and prevent rotation
- Static locking is routine
- Distal fixation: freehand "perfect circle" technique under fluoroscopy
- Consider dynamization for delayed union - but ensure adequate fracture healing is present before weight-bearing, especially in comminuted distal patterns, to prevent coronal plane malalignment
- Overall union rates of 96% have been reported after reamed nailing of distal tibial fractures - Campbell's, p. 3355
Associated Articular Injuries
- Medial malleolus fractures: Cancellous lag screws to stabilize before or after nailing
- Posterior malleolus fractures: Cancellous lag screws; open reduction if intraarticular displacement is present
- Ankle joint involvement: Open reduction required for intraarticular displacement
- Distal fibula fractures: Plate if necessary for ankle joint stability or severe displacement; distal fibular fixation is useful in very distal fractures to facilitate tibial alignment
IMN vs Plate Fixation - Evidence Summary
A 2024 meta-analysis of 20 RCTs (1,528 patients) comparing IMN to plate fixation for distal tibia fractures found: (Li et al., J Orthop Surg Res, 2024)
| Outcome | IMN | Plate |
|---|---|---|
| Surgery time | Shorter (-10.7 min) | Longer |
| Union time | Faster (-1.56 weeks) | Slower |
| Full weight-bearing | Earlier (-2.61 weeks) | Later |
| Wound infection | Lower (OR 0.44) | Higher |
| Secondary procedures | Lower (OR 0.72) | Higher |
| Malunion | Higher (OR 1.53) | Lower |
| Anterior knee pain | Higher (OR 3.94) | Lower |
| Functional scores | No significant difference | No significant difference |
Conclusion: IMN is generally preferred for distal tibia fractures given its overall advantages, but the elevated malunion rate (tied to the metaphyseal instability problem described above) and anterior knee pain require attention. Decision should be individualized. [PMID: 38997735]
Key Pearls
- CT before nailing - rule out articular extension (43A vs 43B/C)
- Two distal locking screws minimum - prevents recurvatum from rotational failure around one screw
- Blocking screws are your most powerful tool for controlling distal fragment alignment
- Plate the fibula first in same-level fractures if fibular fixation is planned - then check tibial alignment
- Suprapatellar approach reduces deforming forces and makes intraoperative fluoroscopy easier distally
- Malalignment is the Achilles heel of distal tibia nailing - weight-bearing restrictions must be followed until significant fracture healing occurs
- 96% union rate is achievable with reamed nailing using modern technique
Sources: Campbell's Operative Orthopaedics 15th Ed 2026, pp. 3354-3357; Rockwood & Green's Fractures in Adults 10th Ed 2025, pp. 3219-3225, 3255; Li et al. J Orthop Surg Res 2024 (PMID: 38997735)
This is a shared conversation. Sign in to Orris to start your own chat.