Now let me search the medical library and PubMed in parallel for comprehensive information on antibiotics for gram-negative bacteria.
Reading File
Finding Sources
Finding Sources
Searching PubMed
"gram-negative bacteria"[MeSH Terms] AND "anti-bacterial agents"[MeSH Terms]
Reading File
Reading File
Reading File
Searching PubMed
"carbapenem-resistant" AND "gram-negative" AND treatment
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
Finding Sources
Searching the Web
antibiotics gram-negative bacteria 2024 2025 new agents WHO ESKAPE pathogens
I now have comprehensive data from textbooks, PubMed, and the web. Let me compile the full answer.
Antibiotics for Gram-Negative Bacteria: A Comprehensive Review
Why Gram-Negative Bacteria Are Harder to Treat
Gram-negative bacteria (GNB) present a unique challenge because they have a double-membrane architecture: an outer membrane (OM) overlying the peptidoglycan layer, and an inner cytoplasmic membrane. This structure creates three intrinsic resistance mechanisms:
- Outer membrane permeability barrier - Antibiotics must pass through porin channels (OmpF, OmpC) to reach the cell wall. Porin mutations reduce pore size or change channel charge, excluding hydrophilic drugs like many beta-lactams.
- Efflux pumps - Active pumping (e.g., AcrAB-TolC in E. coli) reduces intracellular antibiotic concentration.
- Beta-lactamase production - Enzymes secreted into the periplasmic space hydrolyze the beta-lactam ring before it can bind penicillin-binding proteins (PBPs).
- Medical Microbiology 9e, p. 198
Antibiotic Classes Active Against Gram-Negative Bacteria
1. Beta-Lactams
The largest and most important class for GNB infections. All bind PBPs to inhibit peptidoglycan cross-linking, leading to cell lysis.
| Subclass | Key Agents | GNB Coverage |
|---|---|---|
| Penicillins + BLI | Piperacillin-tazobactam (pip-tazo) | Broad; includes Pseudomonas |
| 3rd-gen cephalosporins | Ceftriaxone, ceftazidime | Enterobacterales; ceftazidime covers Pseudomonas |
| 4th-gen cephalosporins | Cefepime | Broad; Pseudomonas, AmpC-stable |
| 5th-gen siderophore cephalosporin | Cefiderocol | Carbapenem-resistant GNB, including A. baumannii |
| Carbapenems | Imipenem, meropenem, ertapenem | Broadest beta-lactam coverage; not ertapenem for Pseudomonas |
| Monobactams | Aztreonam | Gram-negatives only; useful in penicillin allergy |
| Novel BLI combinations | Ceftazidime-avibactam, ceftolozane-tazobactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam | Carbapenem-resistant organisms, MBL producers (when combined with aztreonam) |
Resistance problem - ESBLs and carbapenemases: Simple point mutations in TEM-1 or SHV-1 penicillinases create extended-spectrum beta-lactamases (ESBLs) capable of hydrolyzing nearly all penicillins and cephalosporins. These ESBL genes are typically plasmid-borne and transfer freely between organisms like E. coli and Klebsiella. Carbapenemases (KPC, NDM, OXA-48, VIM) further extend hydrolysis to carbapenems, leaving very few options.
- Medical Microbiology 9e, p. 198-199
2. Aminoglycosides
Agents: gentamicin, tobramycin, amikacin, plazomicin, streptomycin, netilmicin
Mechanism: Irreversible inhibitors of protein synthesis at the 30S ribosome. After passive diffusion through porin channels, they are actively transported across the inner membrane by an oxygen-dependent, proton-pump-coupled process. Inside the cell they act by:
- Blocking the initiation complex of peptide formation
- Causing mRNA misreading and incorporation of incorrect amino acids
- Breaking polysomes into nonfunctional monosomes
The result is irreversible cell death (bactericidal). This oxygen-dependent uptake explains why aminoglycosides are ineffective against strict anaerobes.
GNB use: Most widely used in combination with beta-lactams for serious GNB infections (e.g., Pseudomonas aeruginosa sepsis). Amikacin is reserved for organisms resistant to gentamicin/tobramycin, as it is resistant to most plasmid-mediated aminoglycoside-modifying enzymes. Plazomicin (newest) has enhanced activity against aminoglycoside-resistant strains.
- Katzung's Basic and Clinical Pharmacology 16e, p. 1285-1287
3. Fluoroquinolones
Agents: ciprofloxacin (best GNB coverage), levofloxacin, delafloxacin
Mechanism: Inhibit DNA gyrase (topoisomerase II) and topoisomerase IV, enzymes required for DNA supercoiling and replication. Bactericidal.
GNB coverage: Ciprofloxacin has excellent activity against Enterobacterales, Pseudomonas, and most GNB rods. Levofloxacin covers similar spectrum with enhanced pneumococcal activity. Delafloxacin is a next-generation fluoroquinolone with activity against GNB including Pseudomonas.
Resistance is rising globally. In areas with high fluoroquinolone resistance, they should not be used empirically for Pseudomonas or ESBL infections without susceptibility data.
4. Polymyxins
Agents: Polymyxin B and Colistin (Polymyxin E, given as colistimethate sodium)
Mechanism: Act as cationic detergents that disrupt the lipopolysaccharide (LPS) of the outer membrane, causing membrane permeabilization and cell death.
Spectrum: Restricted to gram-negative aerobes - most Pseudomonas, Acinetobacter, and Enterobacterales are susceptible. Notably, Proteus, Serratia, Stenotrophomonas, and Burkholderia are often intrinsically resistant.
Clinical role: Polymyxins are last-resort agents for carbapenem-resistant A. baumannii and P. aeruginosa. In HAP/VAP caused by organisms susceptible only to polymyxins, inhaled colistin is added to IV colistin to improve pulmonary concentrations. Significant nephrotoxicity and neurotoxicity limit their use.
- Goodman & Gilman's Pharmacological Basis of Therapeutics; Jawetz Medical Microbiology 28e
5. Tetracyclines and Glycylcyclines
Agents: Tigecycline, eravacycline, omadacycline
Mechanism: Bind the 30S ribosome and block polypeptide elongation. Glycylcyclines (tigecycline, eravacycline) evade common tetracycline resistance mechanisms (ribosomal protection, efflux pumps) due to their bulky side chains.
GNB coverage: Broad spectrum including ESBL-producers, carbapenem-resistant organisms, and multidrug-resistant (MDR) strains. Eravacycline was shown non-inferior to meropenem for complicated intra-abdominal infections. Tigecycline has bacteriostatic activity and reduced serum levels (note: not recommended for bacteremia or hospital-acquired pneumonia as monotherapy due to low serum concentrations).
6. Summary of Mechanisms Table
Per Medical Microbiology 9e (Table 17.1):
| Drug Class | Mechanism |
|---|---|
| Beta-lactams | Bind PBPs; inhibit peptidoglycan synthesis |
| Aminoglycosides | 30S ribosome inhibition; irreversible |
| Fluoroquinolones | DNA gyrase / topoisomerase IV inhibition |
| Polymyxins | Outer membrane disruption (LPS binding) |
| Tetracyclines/Glycylcyclines | 30S ribosome; block polypeptide elongation |
| Monobactams (aztreonam) | Bind PBPs; gram-negatives only |
Clinical Decision Framework: Empiric Therapy for GNB HAP/VAP
From Fishman's Pulmonary Diseases (Fishman's), the MDR risk-stratified algorithm is shown below:
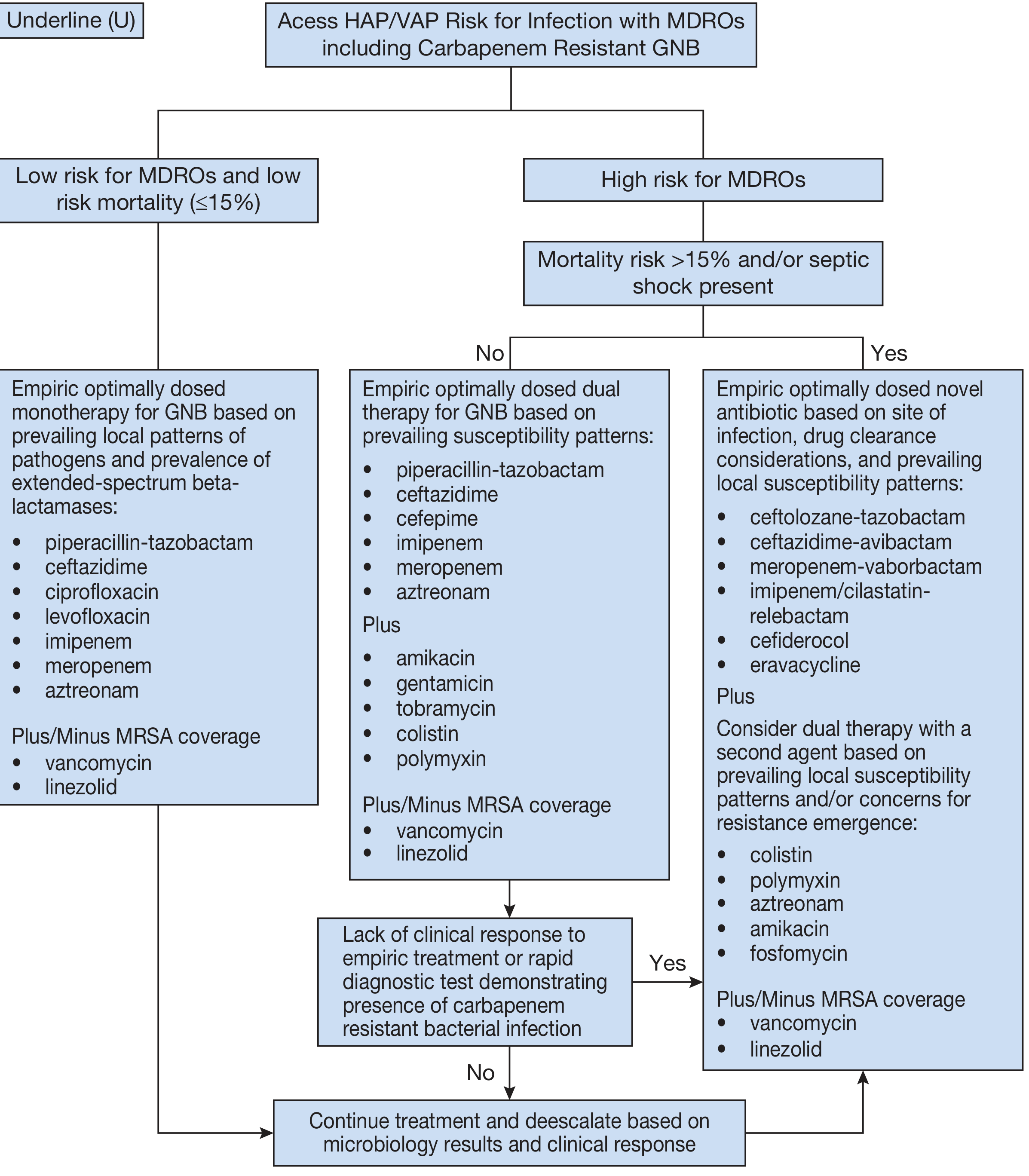
Key takeaways from this algorithm:
- Low MDRO risk, low mortality (<15%): Monotherapy with pip-tazo, ceftazidime, ciprofloxacin, levofloxacin, imipenem, meropenem, or aztreonam (+/- MRSA coverage)
- High MDRO risk, no septic shock: Dual therapy - a beta-lactam (pip-tazo, ceftazidime, cefepime, carbapenem, aztreonam) plus an aminoglycoside (amikacin, gentamicin, tobramycin), colistin, or polymyxin
- High MDRO risk with septic shock or carbapenem resistance confirmed: Novel beta-lactam/BLI combinations - ceftolozane-tazobactam, ceftazidime-avibactam, meropenem-vaborbactam, imipenem-cilastatin-relebactam, cefiderocol, eravacycline - plus consider a second agent (colistin, aztreonam, amikacin, fosfomycin)
Drugs Inactive Against Gram-Negatives (Important!)
- Vancomycin - too large to penetrate OM porins
- Daptomycin - cannot penetrate the GNB cell wall
- Bacitracin - intrinsic resistance due to failure to penetrate GNB cell
These agents are exclusively gram-positive in clinical utility.
Specific Pathogens and Preferred Agents
| Pathogen | First-line | Alternative/MDR |
|---|---|---|
| E. coli, Klebsiella (non-ESBL) | Ceftriaxone, fluoroquinolones | - |
| ESBL producers | Carbapenems | Temocillin (where available) |
| Pseudomonas aeruginosa | Pip-tazo, cefepime, ceftazidime, ciprofloxacin | Ceftolozane-tazobactam, ceftazidime-avibactam |
| Carbapenem-resistant Klebsiella (KPC) | Ceftazidime-avibactam | Meropenem-vaborbactam, imipenem-relebactam |
| MBL-producing (NDM, VIM) | Ceftazidime-avibactam + aztreonam | Cefiderocol |
| Acinetobacter baumannii (CR) | Polymyxin B or colistin ± sulbactam | Cefiderocol, eravacycline |
| Haemophilus influenzae | Amoxicillin-clavulanate, ceftriaxone | Fluoroquinolones |
| Neisseria gonorrhoeae | Ceftriaxone (IM) | - |
Key Recent Evidence from PubMed (2024-2025)
-
Ceftazidime-avibactam + aztreonam for MBL-producing CRE - A 2024 systematic review and meta-analysis (Gupta N et al., Expert Rev Anti Infect Ther) supports this combination as a viable option for carbapenem-resistant Enterobacterales with presumed metallo-beta-lactamase production.
-
Novel beta-lactam PK/PD for carbapenem-resistant GNB pneumonia - A 2024 systematic review (Rando E et al., Int J Antimicrob Agents) examined pharmacokinetics of novel beta-lactam/BLI combinations for pneumonia caused by carbapenem-resistant GNB, supporting optimized dosing strategies for ceftazidime-avibactam, ceftolozane-tazobactam, and cefiderocol.
-
7 vs. 14 days of antibiotics for GNB bloodstream infections - A landmark 2025 noninferiority meta-analysis (Lee TC et al., JAMA Netw Open) found 7 days is noninferior to 14 days for GNB BSI, supporting shorter durations to reduce resistance selection pressure.
-
Rising ceftazidime-avibactam resistance - A 2025 meta-analysis (Wang Y et al., Antimicrob Resist Infect Control) documents increasing global resistance to ceftazidime-avibactam in GNB, a worrying trend given it is a key last-resort drug.
-
Drug-resistant Acinetobacter baumannii - A 2025 systematic review (Dubey V et al., Clin Microbiol Rev) covers mortality, emerging treatments (sulbactam-durlobactam, cefiderocol), and future pharmacological targets for this WHO critical-priority pathogen.
WHO Pipeline Update (2025-2026)
As of the WHO 2025 antibacterial pipeline analysis, the clinical pipeline has shrunk from 97 agents (2023) to 90 (2025), with only 2 representing new chemical classes. WHO released new Target Product Profiles in March 2026 specifically targeting:
- Carbapenem-resistant Enterobacterales
- Carbapenem-resistant A. baumannii
- Carbapenem-resistant P. aeruginosa
The pipeline focus is heavily on gram-negatives given the urgency of the resistance crisis.
Summary
Gram-negative antibiotics span five major pharmacological strategies - cell wall disruption (beta-lactams), outer membrane disruption (polymyxins), ribosome inhibition (aminoglycosides, tetracyclines), and DNA synthesis inhibition (fluoroquinolones). The rise of ESBL, AmpC, carbapenemase, and MBL-producing organisms has compressed effective options dramatically. Novel beta-lactam/beta-lactamase inhibitor combinations (ceftazidime-avibactam, ceftolozane-tazobactam, cefiderocol) are now central to treating pan-resistant GNB, but resistance to these agents is already emerging - making antimicrobial stewardship and susceptibility-guided therapy essential.
This is a shared conversation. Sign in to Orris to start your own chat.