
902e5a10-f477-4196-bd1c-09c525cba2ed.jpeg
From robbins
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
I now have all the information needed from Robbins. Let me compile the complete answer.
Lab Diagnosis of Bleeding Disorders + Why aPTT is Prolonged in von Willebrand Disease
(Robbins & Kumar Basic Pathology)
Part 1: Lab Diagnosis of Bleeding Disorders
The key screening tests used are:
| Test | Normal Range | What it measures |
|---|---|---|
| aPTT (Activated Partial Thromboplastin Time) | 25-37 seconds | Intrinsic pathway (Factors XII, XI, IX, VIII) + common pathway (X, V, II, fibrinogen) |
| PT/INR (Prothrombin Time) | 9.4-12.5 sec / INR 0.9-1.1 | Extrinsic pathway (Factor VII) + common pathway (X, II, fibrinogen) |
| Platelet count | 150,000-400,000/µL | Quantitative platelet defect |
| Bleeding time | Reflects platelet function & primary hemostasis | |
| vWF antigen (55%-200%) | Quantity of von Willebrand factor | |
| vWF:Ristocetin cofactor assay | Functional assay for vWF activity | |
| Factor VIII activity (55%-200%) | Factor VIII level (bound to and stabilized by vWF) |
Interpretation Pattern:
| Disorder | Bleeding Time | aPTT | PT | Platelet count |
|---|---|---|---|---|
| von Willebrand disease | Prolonged | Prolonged | Normal | Normal |
| Hemophilia A (FVIII deficiency) | Normal | Prolonged | Normal | Normal |
| Hemophilia B (FIX deficiency) | Normal | Prolonged | Normal | Normal |
| Thrombocytopenia | Prolonged | Normal | Normal | Low |
| Liver disease / Warfarin | Variable | Prolonged | Prolonged | Variable |
Part 2: Why aPTT is Prolonged in von Willebrand Disease
This is the key concept, and it comes down to the dual role of vWF:
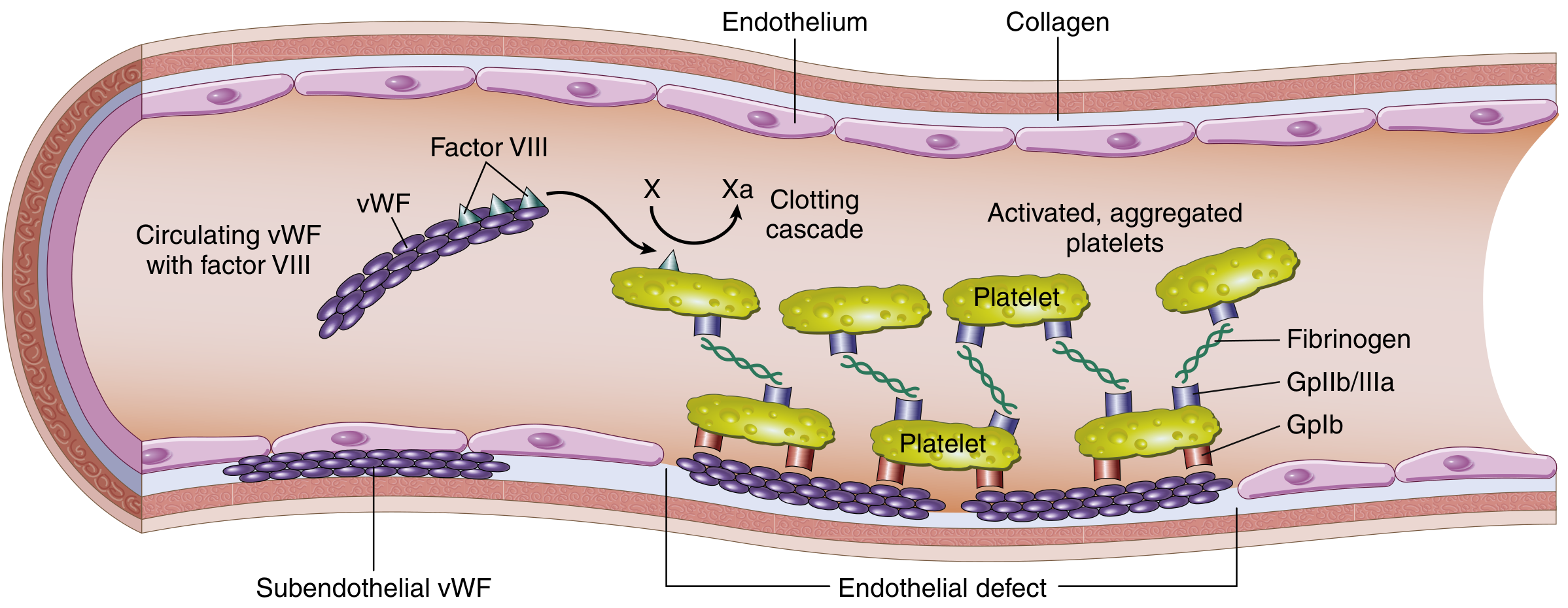
FIG. 10.31 from Robbins - Structure and function of the Factor VIII-vWF complex
The Mechanism (Step by Step):
1. vWF normally acts as a carrier/stabilizer for Factor VIII:
"vWF also stabilizes factor VIII; thus, vWF deficiency leads to a secondary deficiency of factor VIII."
- Robbins & Kumar Basic Pathology, p. 430
2. In von Willebrand disease, vWF is reduced or dysfunctional:
- Without vWF to stabilize it, Factor VIII is rapidly degraded in plasma
- This leads to a secondary reduction in Factor VIII levels
3. Factor VIII is a key component of the intrinsic (contact activation) pathway:
- Factor VIII acts as a cofactor for Factor IXa, forming the "tenase complex" that activates Factor X
- aPTT measures the intrinsic pathway (Factors XII → XI → IX → VIII → X → thrombin)
- When Factor VIII is reduced secondary to vWF deficiency, the intrinsic pathway is slowed
- Result: aPTT is prolonged
Summary in one sentence:
vWF deficiency → secondary Factor VIII deficiency → defective intrinsic coagulation pathway → prolonged aPTT
"In addition to its role in platelet adhesion, vWF also stabilizes factor VIII; thus, vWF deficiency leads to a secondary deficiency of factor VIII."
- Robbins & Kumar Basic Pathology, p. 430
Important Note on vWD Subtypes:
| Type | Defect | aPTT |
|---|---|---|
| Type I (most common) | Reduced quantity of vWF | Mildly prolonged |
| Type II | Dysfunctional vWF (qualitative defect) | Usually normal or mildly prolonged |
| Type III (homozygous, severe) | Near-complete absence of vWF | Markedly prolonged (resembles hemophilia A) |
In Type III, Factor VIII falls so severely that features resemble hemophilia - Robbins & Kumar Basic Pathology, p. 431.
The Special Test for vWD:
The Ristocetin platelet agglutination test is used specifically for vWD:
- Ristocetin enhances binding of vWF to platelet glycoprotein Ib, causing platelet agglutination
- In vWD, this agglutination is reduced or absent (abnormal ristocetin cofactor assay)
- This test serves as a functional bioassay for vWF activity
This is a shared conversation. Sign in to Orris to start your own chat.