Cystic hygroma
Reading File
Finding Sources
Finding Sources
Searching PubMed
"cystic hygroma" OR "cystic lymphangioma"
Reading File
Reading File
Reading File
Reading File
Searching Images
cystic hygroma fetal ultrasound neck
I now have comprehensive content. Let me compile the full answer.
Cystic Hygroma
Definition
A cystic hygroma is a congenital thin-walled cyst containing lymphatic fluid, arising from failure of the primitive lymphatic tree to connect to the venous system — the blind lymphatic pouch dilates to form a macrocystic lymphatic malformation (also called cystic lymphangioma, lymphatic hamartoma, or hygroma cysticum). It is multiloculated, lined by endothelium, and most commonly involves the posterior neck/jugular lymphatic sacs.
Epidemiology & Pathogenesis
- Incidence: 1:100 pregnancies in the first trimester; septated subtype in 1:285 pregnancies
- Arises from failure of the jugular lymphatic sac to drain into the venous system → lymphatic obstruction → cystic dilation
- Can occur anywhere along the lymphatic system: posterior neck (most common), axilla, mediastinum, groin, retroperitoneum
Clinical Features
Prenatal (most commonly detected):
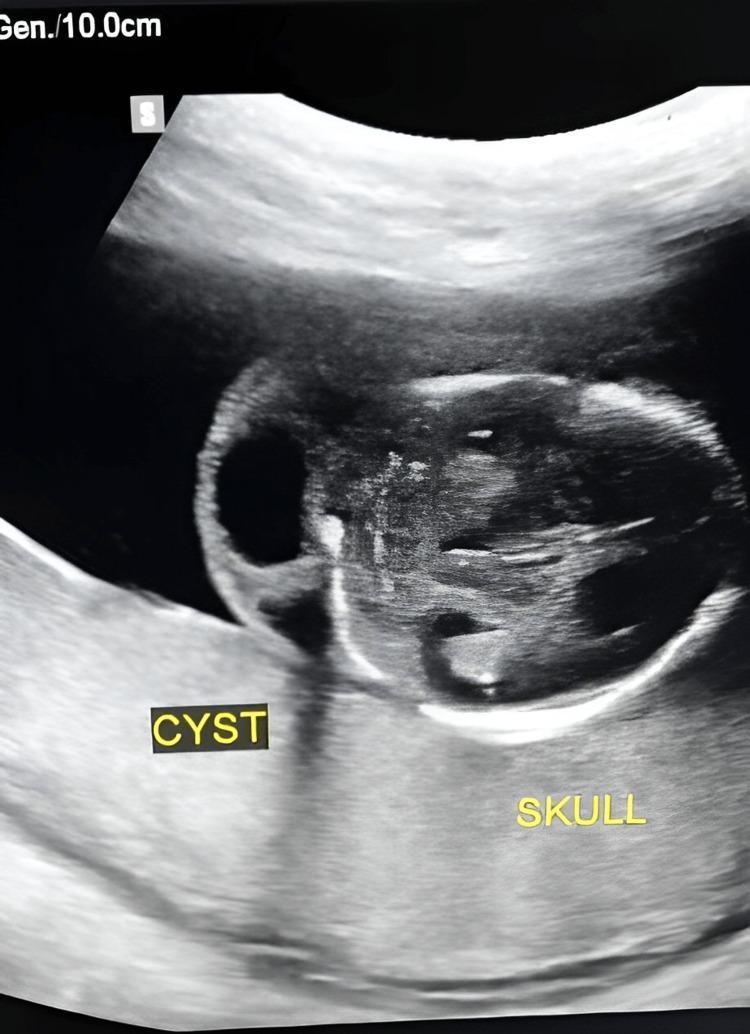
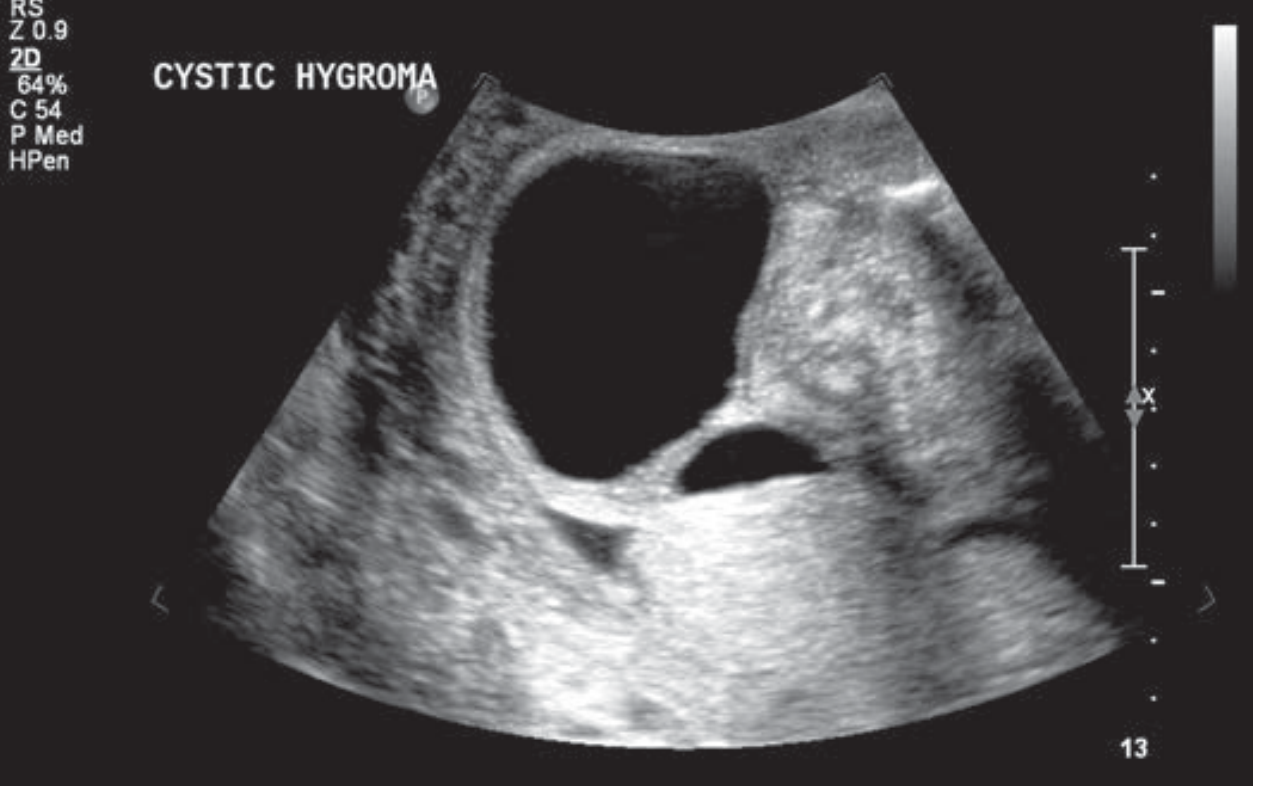
- Anechoic, fluid-filled posterior neck mass — septated or simple
- A thick midline nuchal ligament band is characteristic (separating bilateral jugular sacs)
- May engulf the fetal head cephalad, or extend caudad over the dorsum
- Associated with fetal hydrops in severe cases
Postnatal:
- Soft, translucent, cystic neck mass, often large
- Can distort the airway — potentially life-threatening
- Prone to sudden enlargement from intracystic hemorrhage or infection (becomes tender, tense, purple/yellow)
Associated Anomalies (Prenatal)
Structural anomalies in ~34% of first-trimester cases:
| Category | Specifics |
|---|---|
| Aneuploidy (50%) | Turner syndrome (45,X) — 28.3%; Trisomy 18 — 19.4%; Trisomy 13 — 9%; Triploidy — 4.5% |
| Cardiac anomalies | 72.7% of structural abnormalities — hypoplastic left/right heart, TOF, VSD, complex defects; 4.3% major CHD in euploid fetuses |
| Syndromes | Noonan syndrome, Roberts syndrome, Cornelia de Lange, others |
| Other | Skeletal abnormalities, fetal hydrops, IUFD |
Imaging
Ultrasound (Key Diagnostic Features)
- Anechoic, fluid-filled cavities in the posterior neck
- Thick or thin internal septations
- Thick midline nuchal ligament (Turner syndrome classic)
- May be multiloculated

MRI
Useful postnatally to define extent of lymphatic channels and airway relationship.
Differential Diagnosis
- Thickened nuchal translucency (non-septated)
- Neural tube defects (posterior encephalocele, cervical meningocele)
- Cystic teratoma
- Hemangioma
- Thyroglossal duct cyst / branchial cleft cyst
- Laryngocele
- Fetal hydrops
Management
Antenatal
- Detailed fetal anatomy survey to identify associated anomalies
- Fetal echocardiogram (cardiac anomalies present in majority of structural abnormalities)
- Genetic testing — amniocentesis or CVS for karyotype/chromosomal microarray
- Serial ultrasounds for growth, hydrops, polyhydramnios from esophageal compression, progression
- Assess airway relationship for birth planning
Delivery
- If large cystic neck mass compromises the airway: EXIT procedure (ex utero intrapartum treatment) — secures airway while uteroplacental circulation is maintained
Postnatal / Pediatric Surgical
- Complete surgical excision with meticulous isolation and ligation of lymphatic branches; avoid blunt/electrocautery dissection (risk of recurrence/infection)
- When complete excision is not feasible: sclerotherapy with bleomycin, doxycycline, or OK-432 (Picibanil, derived from Streptococcus pyogenes)
- Sirolimus (mTOR inhibitor) is emerging as a pharmacologic option, particularly for cervicofacial disease
Prognosis
- Highly variable — depends on karyotype, associated anomalies, and trimester at detection
- In the presence of aneuploidy or hydrops: poor prognosis, high rate of IUFD
- Euploid fetuses with isolated hygroma: better outcome but still significant risk of CHD
- Spontaneous resolution can occur (particularly with small, non-septated lesions early in pregnancy)
- A 2025 systematic review (PMID: 40389136) confirmed that perinatal outcomes are strongly stratified by chromosomal status and presence of hydrops
- A 2025 review (PMID: 40190084) highlighted the genetic link between cystic hygroma, nuchal translucency, and congenital heart disease via cardiac lymphatic abnormalities
Sources: Creasy & Resnik's Maternal-Fetal Medicine (8e); Sabiston Textbook of Surgery; Dermatology 2-Volume Set (5e); Thompson & Thompson Genetics in Medicine (9e)
This is a shared conversation. Sign in to Orris to start your own chat.