"Obstructive Sleep apnea" essay answer for PG exam with diagrams/flowcharts under 800 words
obstructive sleep apnea pathophysiology diagram
OSA diagnosis polysomnography AHI criteria management CPAP flowchart
Obstructive Sleep Apnea (OSA) - PG Exam Essay (with flowcharts/diagrams)
Obstructive sleep apnea (OSA) is a sleep-related breathing disorder characterized by recurrent episodes of partial (hypopnea) or complete (apnea) upper airway obstruction during sleep, despite persistent respiratory effort. Diagnosis is by polysomnography (PSG) or validated home sleep apnea testing.
AHI-based severity: Mild 5 to <15, Moderate 15 to <30, Severe >=30 events/hour.
(Murray and Nadel’s Textbook of Respiratory Medicine, p. 2757)
Etiopathogenesis / Pathophysiology
- Anatomical narrowing of pharyngeal airway
- Obesity, enlarged tongue/soft tissues, craniofacial abnormalities (retrognathia), longer airway
- Increased airway collapsibility (critical closing pressure, Pcrit)
- Sleep-related fall in pharyngeal dilator muscle tone
- Reduced lung volume in supine posture (less tracheal traction)
- Fluid shift and upper airway edema/inflammation
- Instability of ventilatory control in some patients
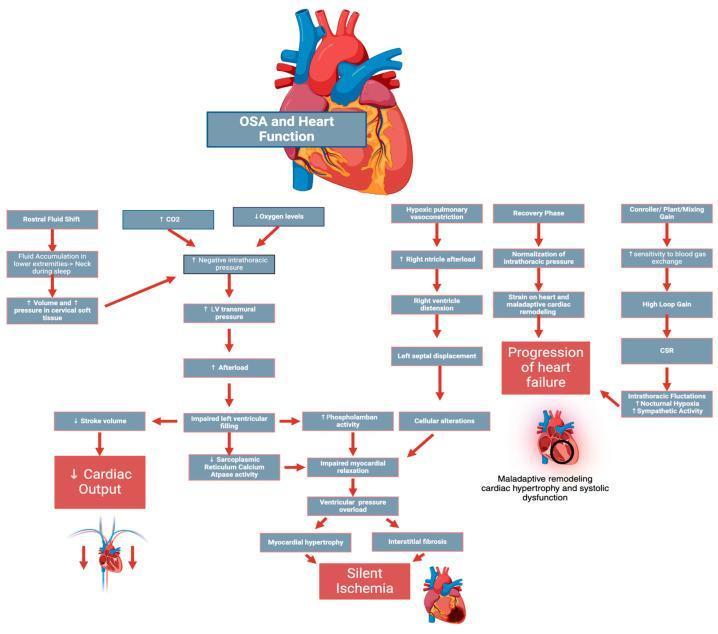
- Intermittent hypoxemia
- Hypercapnia
- Recurrent arousals and sleep fragmentation
- Sympathetic activation, oxidative stress, endothelial dysfunction
leading to cardiovascular and metabolic morbidity.
(Murray and Nadel’s Textbook of Respiratory Medicine, p. 2760)
Risk factors
- Obesity (most important modifiable factor)
- Male sex, increasing age
- Craniofacial crowding, adenotonsillar hypertrophy
- Alcohol/sedatives, smoking
- Nasal obstruction
- Endocrine/metabolic factors (e.g., hypothyroidism, acromegaly)
- Family/genetic predisposition
Clinical features
Day symptoms: excessive daytime sleepiness, unrefreshing sleep, morning headache, poor concentration, irritability, reduced work/driving performance.
Diagnostic approach (Flowchart)
Clinical suspicion (snoring + daytime sleepiness/witnessed apneas)
|
v
Risk assessment (history, exam, Epworth score, comorbidity screen)
|
v
Objective sleep test mandatory
(PSG preferred / HSAT in selected uncomplicated adults)
|
v
AHI/RDI-based severity + oxygen desaturation burden + symptom burden
|
v
Phenotype/endotype + comorbidities + patient preference
|
v
Individualized treatment plan + long-term follow-up
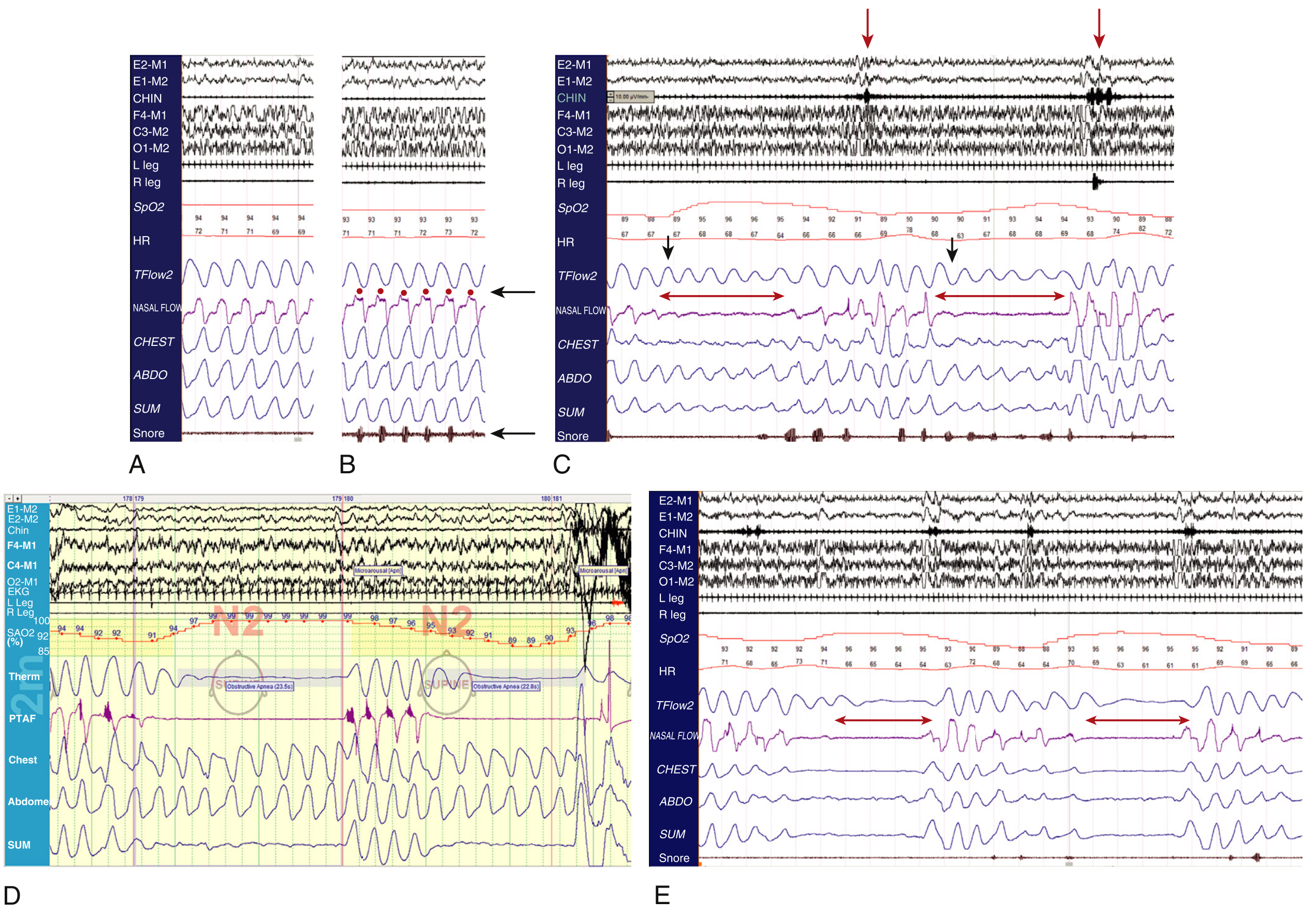
Investigations
- Gold standard: attended overnight PSG
Records airflow, respiratory effort, oxygen saturation, sleep stages, ECG, limb movements, etc. - Indices: AHI, RDI, oxygen desaturation, arousal index, sleep architecture
- HSAT: alternative in selected adults without major cardiorespiratory/neuromuscular complexity
- Ancillary: thyroid function, metabolic/cardiovascular risk evaluation, ENT evaluation where relevant
Management
1) General and behavioral
- Weight reduction (diet, exercise, bariatric approach when indicated)
- Avoid alcohol/sedatives at bedtime
- Sleep hygiene and positional therapy
- Treat nasal obstruction and contributing factors
2) Positive airway pressure (PAP)
- CPAP is first-line in moderate-severe OSA and symptomatic disease
- Reduces obstructive events, improves sleepiness and quality of life
- Improves BP and may reduce cardiovascular risk in adherent patients
3) Oral appliance therapy
- Mandibular advancement devices in mild-moderate OSA or CPAP intolerance
4) Surgery (selected patients)
- Upper airway surgery for anatomical obstruction (e.g., multilevel approaches)
- Maxillomandibular advancement in selected refractory cases
- Therapy often individualized and combination treatment may be needed
(Murray and Nadel’s Respiratory Medicine, p. 2818)
5) Follow-up
- Assess adherence, residual symptoms, machine data, side effects
- Reassess comorbidities and repeat sleep study when indicated
Complications
- Systemic hypertension, coronary artery disease, arrhythmia, heart failure, stroke
- Insulin resistance/metabolic syndrome
- Neurocognitive impairment, depression
- Increased risk of motor vehicle and occupational accidents
Prognosis
Exam-ready management flowchart
Diagnosed OSA
|
+--> Mild (AHI 5-15): lifestyle +/- positional therapy +/- oral appliance
|
+--> Moderate-Severe (AHI >=15): CPAP first-line + lifestyle
|
+--> CPAP intolerance/non-response:
reassess mask/interface, pressure titration, adherence barriers
consider oral appliance / surgery / combination therapy
|
--> periodic follow-up: symptoms + AHI control + comorbidity control
Diagrams for answer sheet / viva discussion
"Hearing Disability Certificate" essay answer for ENT PG exam india
The system is currently experiencing high demand and cannot process your request. Your request exceeds the maximum usage size allowed during peak load. For improved capacity reliability, consider switching to Provisioned Throughput.
We encountered an error while processing your request. Please try again or reach out to us for help.
Hearing Disability Certificate" essay answer for ENT PG exam india
The system is currently experiencing high demand and cannot process your request. Your request exceeds the maximum usage size allowed during peak load. For improved capacity reliability, consider switching to Provisioned Throughput.
We encountered an error while processing your request. Please try again or reach out to us for help.