Clubbing in medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
finger clubbing pathophysiology causes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have a thorough picture from multiple authoritative sources. Here is a full, well-structured answer.
Clubbing (Digital Clubbing / Hippocratic Fingers)

Definition
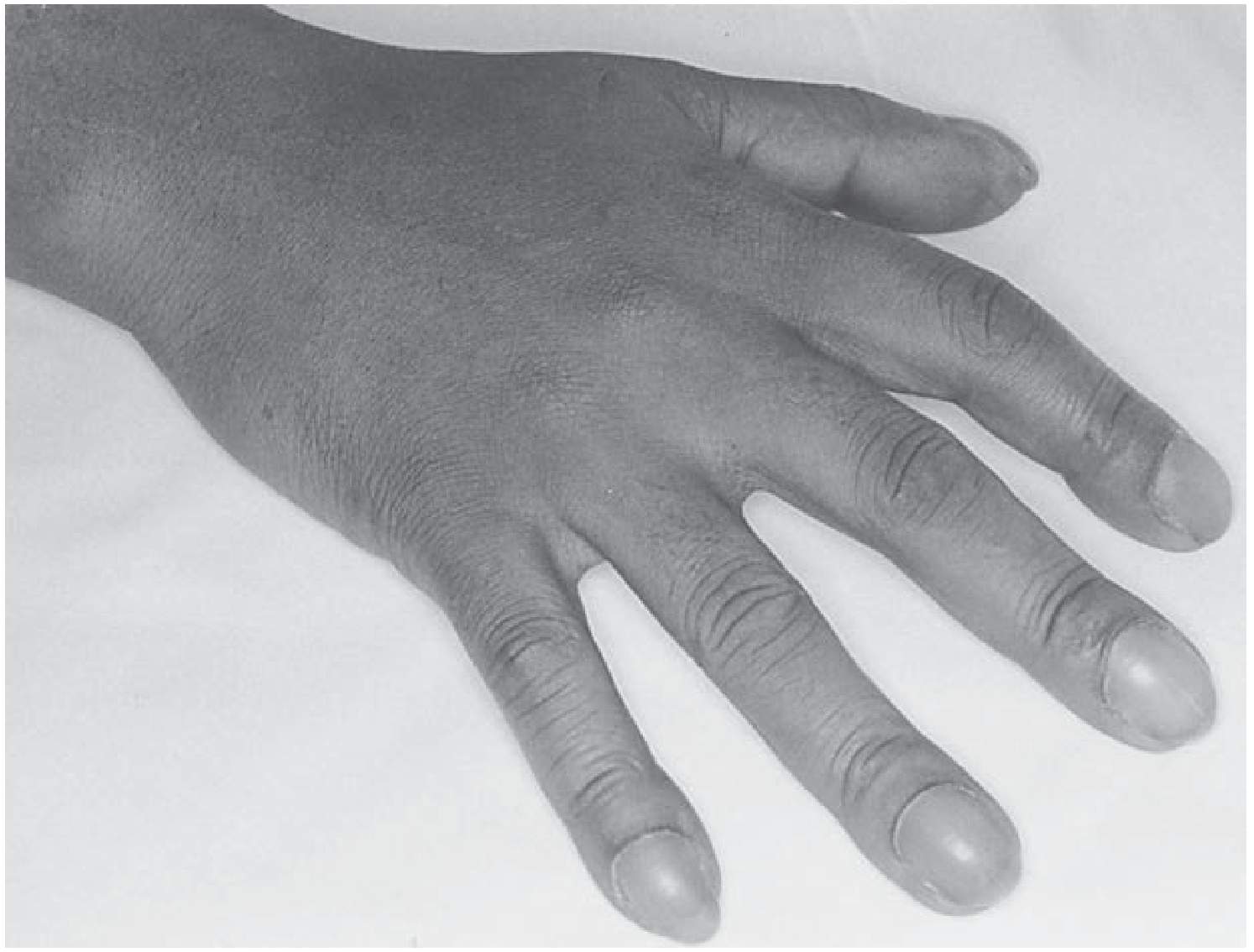
Clubbing is the selective bulbous enlargement of the distal segments of the fingers and/or toes due to proliferation of connective tissue and soft tissue on the dorsal surface, accompanied by increased sponginess of the soft tissue at the base of the nail. It has been recognized since Hippocrates, who noted its association with empyema.
- Harrison's Principles of Internal Medicine 22E
- Fishman's Pulmonary Diseases and Disorders
Clinical Features (How to Recognize It)
Four hallmarks, in rough order of sensitivity:
| Feature | Detail |
|---|---|
| Loss of Lovibond angle | Normal nail-to-cuticle angle is ~160-165°; in clubbing it becomes 180° or greater (obliterated) |
| Nail bed softening / floating nails | Perilingual erythema; nails feel spongy and "float" on the bed |
| Bulbous distal phalanx | Enlarged, sometimes warm and erythematous; may be mobile when pressure applied over the matrix |
| Nail curvature | Nails curve abnormally in both longitudinal and coronal planes |
Schamroth sign: When the dorsal surfaces of the same finger from each hand are opposed back-to-back, a normal diamond-shaped window is visible. In clubbing, this window is absent.
- Andrews' Diseases of the Skin; Murray & Nadel's Textbook of Respiratory Medicine
Pathogenesis
The exact mechanism is not fully established, but current evidence points to two overlapping processes:
-
Vasodilation and arteriovenous shunting - A humoral substance (or substances) that would normally be inactivated by the pulmonary capillaries escapes into the peripheral circulation, causing vasodilation of vessels in the fingertip and forming arteriovenous connections. This raises hydrostatic pressure in capillaries and venules, promoting fluid transudation into the interstitium. This explains clubbing in cyanotic heart disease, hepatic cirrhosis (with pulmonary AV anastomoses), and various lung diseases.
-
Angiogenic growth factors - Histochemical studies show increased VEGF (vascular endothelial growth factor), PDGF (platelet-derived growth factor), HIF-1α, and HIF-2α, along with markedly increased microvessel density in the stroma of clubbed digits. Platelet precursors (megakaryocytes) that bypass the pulmonary filter may release these growth factors directly in the digital circulation.
-
Prostaglandin pathway (hereditary form) - Mutations in HPGD (encoding NAD+-dependent 15-hydroxyprostaglandin dehydrogenase) and in the prostaglandin transporter gene SLCO2A1 have been identified in primary/hereditary clubbing, suggesting prostaglandin excess plays a role.
- Murray & Nadel; Fishman's; Andrews' Diseases of the Skin
Causes
Not Associated with Overt Disease
- Hereditary/familial clubbing (dominant trait)
- Sporadic clubbing
- Pachydermoperiostosis (primary hypertrophic osteoarthropathy)
Thoracic - Most Common Category
- Lung cancer (single most common acquired cause)
- Bronchiectasis
- Cystic fibrosis
- Lung abscess / empyema
- Idiopathic pulmonary fibrosis (IPF) / asbestosis
- Sarcoidosis
- Tuberculosis
- Mesothelioma
- Other thoracic neoplasms (esophageal cancer, lymphoma)
Important: COPD does NOT cause clubbing. Clubbing in a COPD patient should prompt a search for lung cancer.
Cardiac / Vascular
- Cyanotic congenital heart disease
- Subacute bacterial endocarditis (infective endocarditis)
- Pulmonary arteriovenous fistula / hereditary hemorrhagic telangiectasia
- Takayasu's arteritis, Behçet syndrome
- Infected aortic graft
Gastrointestinal / Hepatic
- Inflammatory bowel disease (Crohn disease, ulcerative colitis)
- Hepatic cirrhosis / biliary cirrhosis
- Hepatopulmonary syndrome
- Polyposis coli, hepatoma
Other
-
HIV infection (~36% of HIV-infected patients)
-
Thyroid acropachy
-
Hemoglobinopathies / congenital methemoglobinemia
-
Secondary hyperparathyroidism
-
Toxic exposure (arsenic, mercury, beryllium)
-
Voriconazole (drug-induced)
-
Jackhammer operators (occupational)
-
Murray & Nadel eTable 18.1; Harrison's; Andrews'
Unilateral / Asymmetric Clubbing
Clubbing is typically bilateral and symmetric. Unilateral or asymmetric clubbing points to a local cause:
- Subclavian artery aneurysm
- Brachial AV fistula
- Median nerve injury
- Local trauma
- Hemiplegia
- Ipsilateral pulmonary sulcus (Pancoast) tumor invading the brachial plexus
- Takayasu arteritis, sarcoidosis
A special pattern: in patent ductus arteriosus with reversed shunt (Eisenmenger via PDA), clubbing affects only the toes (not the fingers), because desaturated blood enters distal to the subclavian vessels.
Hypertrophic Osteoarthropathy (HOA)
Clubbing may coexist with - or progress to - HOA. This is subperiosteal formation of new cancellous bone at the distal diaphyses of long bones (radius, ulna, tibia, fibula). Features include:
- Painful, symmetric arthritis-like changes at shoulders, knees, ankles, wrists, elbows
- Periosteal new bone visible on X-ray or MRI; hot on bone scan (99mTc-MDP)
- Most strongly associated with: bronchogenic carcinoma, mesothelioma, cystic fibrosis, bronchiectasis
Current evidence suggests clubbing and HOA represent different stages of the same disease process (Rheumatology, 2-Volume Set).
Clinical Significance and Workup
- Clubbing was found in ~1% of internal medicine admissions and was associated with serious underlying disease in 40% of cases.
- New-onset clubbing always warrants a chest X-ray, and if unrevealing, a CT scan to exclude pulmonary neoplasm.
- Clubbing can develop rapidly (within ~2 weeks, e.g., new empyema) and reverse similarly (e.g., after cardiac surgery, lung transplant for CF, or treatment of lung cancer).
Summary Mnemonic: CLUBBING
| Letter | Cause |
|---|---|
| C | Cardiac (cyanotic CHD, endocarditis) |
| L | Lung cancer (most common) |
| U | Ulcerative colitis / Crohn's |
| B | Bronchiectasis / Bronchial abscess |
| B | Biliary/hepatic cirrhosis |
| I | Idiopathic / Inherited |
| N | Neoplasm (mesothelioma, etc.) |
| G | GI diseases / general infections |
Sources: Harrison's Principles of Internal Medicine 22E; Fishman's Pulmonary Diseases and Disorders; Murray & Nadel's Textbook of Respiratory Medicine; Andrews' Diseases of the Skin
This is a shared conversation. Sign in to Orris to start your own chat.