Acute osteomyelitis
Reading File
Finding Sources
Finding Sources
Searching Images
acute osteomyelitis pathology radiology
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have all the material needed for a comprehensive answer.
Acute Osteomyelitis
Definition & Classification
Acute osteomyelitis is bone infection diagnosed within 2 weeks of symptom onset. Subacute osteomyelitis exceeds 2 weeks; chronic osteomyelitis presents months after onset. — Grainger & Allison's Diagnostic Radiology
Pathophysiology
Infection reaches bone via three routes:
- Haematogenous spread — most common in children and in adult vertebral disease
- Contiguous spread — from adjacent soft-tissue infection or sinusitis
- Direct implantation — trauma, open fractures, surgical instrumentation, animal bites
Infection preferentially seeds the metaphysis due to its rich, sluggish blood supply. From there it can:
- Spread laterally through Volkmann canals → breach cortex → lift periosteum → subperiosteal abscess
- Perforate periosteum → soft-tissue abscess
- Spread to epiphysis/joint (especially in neonates and adults after physeal fusion) → septic arthritis
Age-specific vascular anatomy drives this pattern:
- Neonates: metaphyseal capillaries connect to epiphyseal plate → easy joint extension, multifocal involvement in ~50%
- Children (>1 year): transphyseal vessels atrophy, cortex thickens → subperiosteal abscesses predominate
- Adults: after physeal ossification, metaphyseal-epiphyseal anastomoses reform → joint seeding possible again, but periosteum is firmly adherent, limiting subperiosteal abscess
Bacteria in bone form biofilm, where organisms exist in planktonic, slow-growing, and dormant states. Antibiotics target only metabolically active (planktonic) bacteria, explaining treatment difficulty and the rationale for surgical débridement in established infection. — Rosen's Emergency Medicine
Epidemiology & Risk Factors
- Acute haematogenous osteomyelitis (AHO) is most common in children <5 years; 2–3× more common in boys
- Long bones (femur, tibia, humerus) account for ~80% of cases
- Risk factors: diabetes mellitus, sickle cell disease, HIV, IV drug use, chronic corticosteroids, rheumatoid arthritis, prosthetic devices, immunosuppression
Microbiology
S. aureus is the leading organism in all age groups except neonates. MRSA is now the most common cause of AHO in children.
| Age Group | Key Organisms |
|---|---|
| Neonates | Group B Streptococcus, E. coli, S. aureus, S. epidermidis |
| Infants/children | S. aureus (MRSA dominant), Group A Strep, Kingella kingae |
| Adolescents/adults | S. aureus, Gram-negative rods (diabetics/elderly) |
| IV drug users | S. aureus, Pseudomonas aeruginosa |
| Sickle cell disease | Salmonella spp., S. aureus |
| Puncture wounds (foot) | P. aeruginosa |
| Animal/human bites | Pasteurella multocida, Eikenella, oral flora |
| War injuries/MDR | MRSA, Enterobacteriaceae, Acinetobacter |
Kingella kingae is fastidious, can mimic Haemophilus, and often requires PCR for diagnosis. H. influenzae type b has essentially disappeared as a cause in vaccinated children. — Rosen's Emergency Medicine, Grainger & Allison's
Clinical Features
Children (typically ages 1–10 years):
- Pain and reluctance to use the affected limb (sudden limp, inability to bear weight)
- Localized warmth, swelling, erythema — may develop later
- Systemic: fever, chills, malaise, vomiting — usually not toxic-appearing
- Point tenderness over the infected metaphysis is the most consistent finding
Adults:
- Fever, rigors; may appear toxic in severe cases
- Fatigue, malaise, anorexia (less consistent)
- Point tenderness is the hallmark; palpable warmth and soft-tissue swelling variable
- Vertebral osteomyelitis: back pain in ~90%, tenderness over spinous process; neurological deficits in <40%; only 10% appear septic at presentation — diagnosis often delayed up to 4 months
Neonates:
- Often not severely ill; presents as failure to thrive
- Minimal systemic signs; diagnosis frequently delayed
- Multiple sites involved in ~50%; concurrent septic arthritis common
Investigations
Laboratory
- ESR and CRP are elevated in virtually all cases (ESR/CRP 98–100% in vertebral osteomyelitis)
- Leukocytosis is common but non-specific
- Blood cultures: positive in ~40% of children with AHO; tissue cultures positive in ~86% — obtain before antibiotics
- Gram stain of bone aspirate: often negative (biofilm effect)
Imaging
Plain radiographs — first-line:
- Normal in early disease; osseous changes appear only after 10–21 days (loss of ~30–50% bone mineral density)
- Useful to exclude fractures, Perthes disease, SFCE, malignancy
- Early finding: soft-tissue swelling; late: periosteal reaction, lytic lesions, cortical destruction
Ultrasound:
- Detects subperiosteal abscess as hypoechoic fluid along bone surface
- Useful to guide aspiration for culture; increased Doppler flow around soft-tissue abscesses
MRI — investigation of choice:
- High sensitivity and specificity for acute, subacute, and chronic osteomyelitis
- T1: low signal (bone marrow oedema, marrow replacement)
- T2/STIR: high signal (oedema, fluid)
- Post-gadolinium: enhancing walls of abscesses; non-enhancing pus collection
- Fat globule sign on T1 is pathognomonic for acute osteomyelitis
- Identifies physeal involvement, subperiosteal/intraosseous/soft-tissue abscesses, and septic arthritis
- For vertebral disease: MRI whole spine with and without contrast; T2-weighted sequences most diagnostic; sensitivity ~90%
CT:
- Good for cortical destruction and guided needle aspiration; less useful than MRI in children (radiation); helpful when MRI unavailable
Bone scintigraphy (³⁹mTc-MDP):
- Useful in early disease and for detecting multifocal involvement; non-specific (positive in trauma, tumour)
- Largely replaced by MRI for vertebral osteomyelitis
MRI Appearance
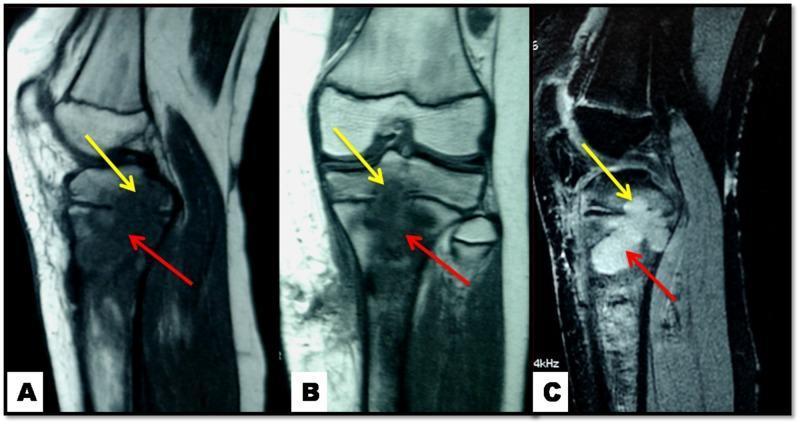
MRI of pediatric knee: T1 images (A, B) show hypointense metaphyseal lytic lesions (red arrows); T2 image (C) shows corresponding hyperintensity. Yellow arrows show transphyseal extension, demonstrating how infection can cross the physis in children.
Complications
- Chronic osteomyelitis (sequestrum, involucrum, Brodie abscess, sinus tracts)
- Septic arthritis (especially in neonates and adults)
- Bacteraemia and sepsis
- Pathological fracture through areas of bone destruction
- Growth disturbance in children if physis is involved (shortened or deformed limb)
- Vertebral: epidural abscess, spinal cord compression, paralysis (<15% of vertebral cases); paraspinal/psoas abscess, empyema
Management
Principles
Aggressive treatment of acute osteomyelitis reduces progression to chronic osteomyelitis. — Textbook of Family Medicine
1. Blood cultures before antibiotics
2. Empirical antibiotic therapy (tailor once cultures return):
| Scenario | Empirical Choice |
|---|---|
| Children (community-acquired AHO) | Anti-staphylococcal agent ± MRSA cover (clindamycin or vancomycin if MRSA prevalent) |
| MRSA suspected/confirmed | Vancomycin IV (first-line); linezolid, daptomycin as alternatives |
| Neonates | Anti-staphylococcal + cover for Group B Strep & Gram-negatives |
| IV drug user | Cover Pseudomonas: piperacillin-tazobactam or ciprofloxacin |
| Vertebral (adults) | Vancomycin + broad Gram-negative cover until cultures available |
Duration: typically 4–6 weeks total (IV followed by oral step-down when clinical improvement and falling inflammatory markers); children with uncomplicated AHO may do well with shorter courses if treated early.
3. Surgical indications:
- Failure to respond to antibiotics within 48–72 hours
- Subperiosteal or soft-tissue abscess requiring drainage
- Necrotic bone / sequestrum requiring debridement
- Septic arthritis complicating osteomyelitis
- Spinal cord compression in vertebral osteomyelitis
- Prosthetic joint involvement (complete surgical débridement essential — biofilm)
4. Orthopaedic involvement is mandatory for suspected osteomyelitis in children, neonates, and vertebral disease.
Key Differentials
- Septic arthritis, Ewing sarcoma, osteosarcoma, Langerhans cell histiocytosis, stress fracture, Perthes disease, SFCE, cellulitis
Sources: Grainger & Allison's Diagnostic Radiology; Rosen's Emergency Medicine, 10th ed.; Textbook of Family Medicine, 9th ed.; Sherris & Ryan's Medical Microbiology, 8th ed.
Intra articular shoulder steroid administration
Reading File
Finding Sources
Finding Sources
Searching Images
intra-articular shoulder injection technique anatomy
Finding Sources
Finding Sources
Reading File
Loading Image
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive, authoritative content from multiple textbooks. Here is the full clinical summary.
Intra-articular Shoulder (Glenohumeral) Steroid Injection
Indications
The glenohumeral joint injection is indicated for:
- Adhesive capsulitis (frozen shoulder) — the most common and well-supported indication; corticosteroid injection into the glenohumeral joint (combined with subacromial bursa injection) is a core non-operative treatment. Approximately 90% of frozen shoulder cases respond to physical therapy, corticosteroid injection, and NSAIDs. — Miller's Review of Orthopaedics, Goldman-Cecil Medicine
- Glenohumeral osteoarthritis — as part of a multimodal non-operative regimen including NSAIDs, activity modification, and physiotherapy — Miller's Review of Orthopaedics
- Inflammatory arthritides (rheumatoid arthritis, crystal arthropathy) involving the glenohumeral joint
- Acromioclavicular joint degeneration — as a separate injection site (not glenohumeral)
Anatomy of the Glenohumeral Joint
Key landmarks for injection:
- Coracoid process — palpable bony prominence anteriorly, inferior to the clavicle and medial to the humeral head; critical for the anterior approach
- Acromion — the posterior inferolateral corner serves as the landmark for the posterior approach
- Glenohumeral joint space — lies between the humeral head and the glenoid rim, accessible both anteriorly and posteriorly
Approaches
Two standard approaches exist. Either can be used; choice is based on operator familiarity and clinical context.
A. Anterior Approach
- Patient seated with arm at side
- Externally rotate the shoulder — this opens the joint space anteriorly
- Identify and palpate the coracoid process
- Insert the needle 1 cm inferior and 1 cm lateral to the coracoid process
- Direct the needle perpendicularly or slightly laterally into the glenohumeral joint
- A correctly placed needle should not contact bone
B. Posterior Approach (preferred by many)
- Patient seated with the arm internally rotated across the waist
- Palpate the inferoposterior aspect of the acromion with the thumb
- Place the index finger on the coracoid process anteriorly (target landmark)
- Insert the needle just below the posterior acromion, aiming toward the coracoid process
- Advance 2–3 cm deep until in the joint space
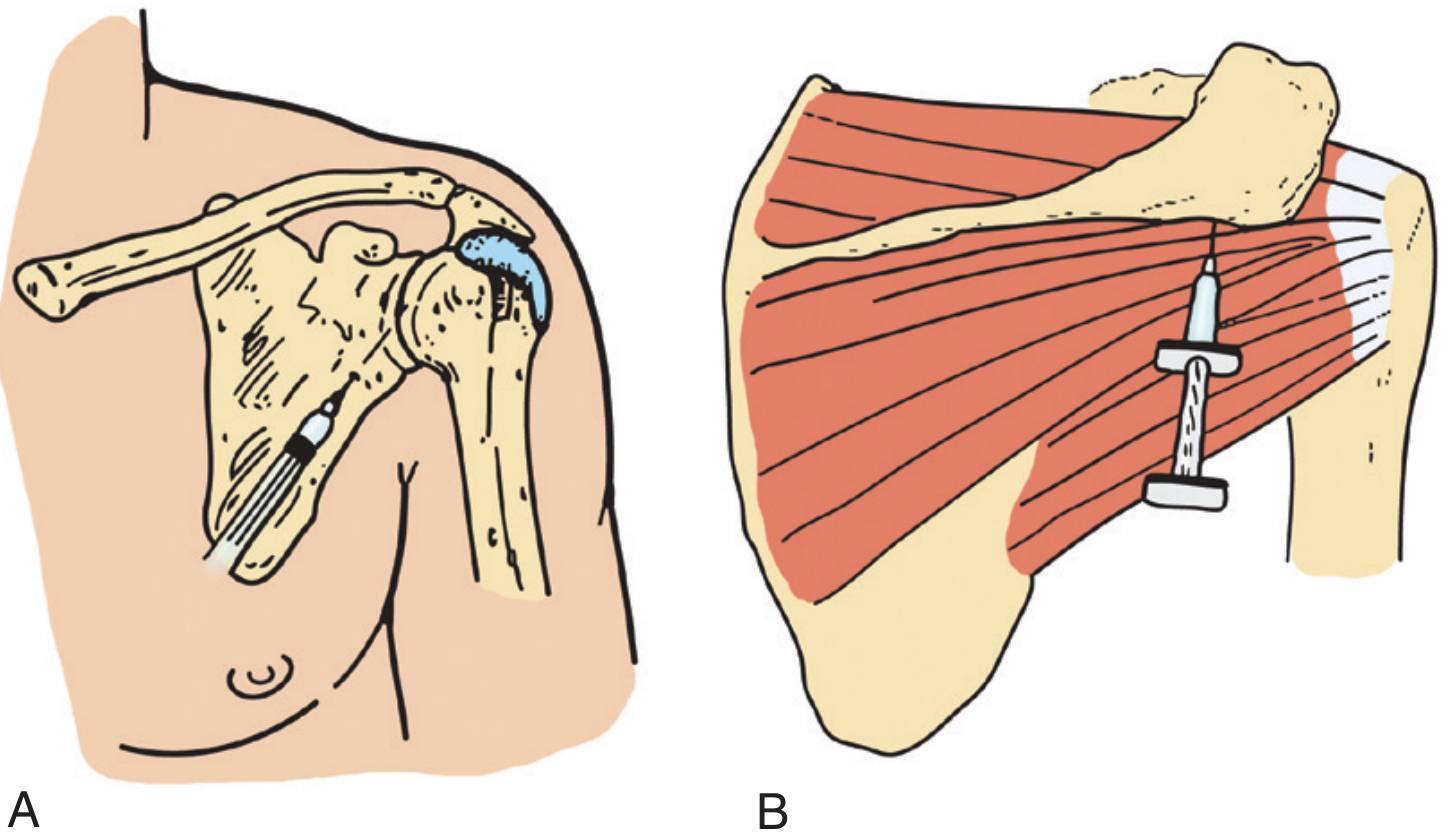
Intra-articular shoulder injection — anterior (A) and posterior (B) approaches. — Pfenninger & Fowler's Procedures for Primary Care
Drugs & Dosage
From Pfenninger & Fowler's reference table (Table 192-5):
| Agent | Details |
|---|---|
| Needle | 20-gauge, 1.5-inch |
| Local anaesthetic | 5–7 mL of 1% lidocaine |
| Corticosteroid | 20–40 mg methylprednisolone acetate (or equivalent) |
Alternative corticosteroid dosing (Goldman-Cecil Medicine):
- Methylprednisolone acetate 40 mg/mL, 1 mL injected into the glenohumeral joint and the subacromial bursa
Other commonly used agents:
- Triamcinolone acetonide — standard for large joints; 20–40 mg intra-articular
- Betamethasone — 6–12 mg for large joints (per Textbook of Family Medicine)
These can be mixed with lidocaine in the same syringe unless using hyaluronic acid (which must not be mixed with steroids or lidocaine).
Ultrasound Guidance
Ultrasound-guided injection is superior to landmark-guided ("blind") injection because it:
- Confirms real-time needle placement in the joint space
- Avoids vascular structures
- Allows observation of injectate flowing into the target space
- Enables more accurate interpretation of the clinical response (a missed blind injection may be misinterpreted as treatment failure)
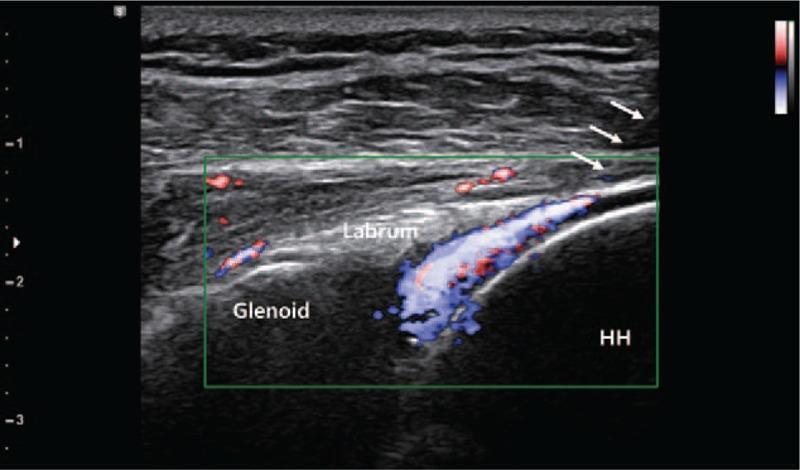
Ultrasound-guided posterior glenohumeral injection — color Doppler (blue signal) confirms delivery of injectate between glenoid and humeral head (HH), with the hyperechoic posterior labrum visible between them.
US-guided technique (step-by-step):
- Position patient comfortably; apply gel over the posterior shoulder
- Identify the glenohumeral joint with the transducer; position transducer parallel to the intended needle path
- Cleanse the skin at the needle entry point (do not move the transducer)
- Use ethyl chloride spray to superficially anaesthetise the puncture site
- Hold needle parallel to the transducer; enter skin and inject small amounts of local anaesthetic ahead of the needle tip as it advances
- Keep both the needle and target in constant view on the US screen
- Confirm intra-articular placement by observing fluid distension in the joint
- Inject the corticosteroid; withdraw needle; apply pressure and adhesive bandage
Subacromial Bursa vs. Glenohumeral Joint Injection
These are distinct injection sites, often confused:
| Feature | Glenohumeral (Intra-articular) | Subacromial Bursa |
|---|---|
| Target | Joint capsule between humeral head and glenoid | Bursa between rotator cuff and acromion |
| Indications | Adhesive capsulitis, OA, inflammatory arthritis | Rotator cuff impingement, bursitis, supraspinatus tendinitis |
| Entry (landmark) | 1 cm inf/lat to coracoid (anterior) or below acromion aiming to coracoid (posterior) | 1 cm below lateral edge of acromion through deltoid, perpendicular |
| Needle | 20G, 1.5 inch | 22–25G, 1–1.5 inch |
| Steroid dose (methylprednisolone) | 20–40 mg | 30–40 mg |
| Lidocaine | 5–7 mL | 5–7 mL |
In adhesive capsulitis, both sites may be injected as part of a comprehensive program. — Goldman-Cecil Medicine
Contraindications
- Septic arthritis / active joint infection — absolute contraindication
- Bacteraemia / systemic infection
- Adjacent skin cellulitis at the injection site
- Coagulopathy / anticoagulation (relative)
- Known allergy to the injectate
- Joint prosthesis (without specialist guidance)
- Previous failed response to multiple injections at the same site (consider alternative management)
Post-procedure Instructions
- Avoid strenuous activity for 48 hours post-injection
- Pain relief from lidocaine may be noted within minutes of injection — confirms correct placement
- Begin or continue physiotherapy (pendulum exercises, wall climbing, progressive range-of-motion and strengthening) in conjunction with injection
- Steroid effect typically peaks over several days to weeks
Complications
Possible complications of intra-articular and soft-tissue injections include:
- Septic arthritis — the most feared complication; strict aseptic technique is mandatory
- Post-injection steroid flare — transient worsening of pain 12–24 hours post-injection; managed with NSAIDs and ice
- Articular cartilage damage with repeated injections
- Skin/subcutaneous atrophy or depigmentation at the injection site (more common with superficial injections)
- Inadvertent injection into a vein or artery (rarely causes systemic harm as both lidocaine and corticosteroids are given IV for other conditions, but therapeutic effect is lost)
- Tendon weakening/rupture if injected directly into tendon rather than peritendinous space
- Temporary elevation of blood glucose in diabetic patients
- Hypothalamic-pituitary-adrenal axis suppression with frequent injections
General practice: limit to 3–4 injections per joint per year, with intervals of at least 4–6 weeks between injections.
Sources: Pfenninger & Fowler's Procedures for Primary Care, 3rd ed.; Goldman-Cecil Medicine; Miller's Review of Orthopaedics, 9th ed.; Textbook of Family Medicine, 9th ed.; Gray's Anatomy for Students
This is a shared conversation. Sign in to Orris to start your own chat.