Here is your complete, A-to-Z guide on Canine Distemper (CD). Every term in brackets is explained inline. This is written for a veterinarian in training who wants conceptual clarity on everything.
CANINE DISTEMPER (CD) — Complete Veterinary Guide
1. CLASSIFICATION & ETIOLOGY (Cause)
Canine Distemper Virus (CDV) belongs to:
| Level | Classification |
|---|
| Family | Paramyxoviridae |
| Genus | Morbillivirus |
| Species | Canine morbillivirus |
Key Viral Properties:
- Enveloped [virus has a lipid membrane coat — this makes it FRAGILE in the environment, easily killed by disinfectants]
- Single-stranded, negative-sense RNA virus [genetic material is RNA, in negative polarity = needs to be converted before it can make proteins]
- Pleomorphic [variable shape — spherical to filamentous]
- Size: 150–300 nm
- Non-segmented genome [genome is one continuous piece, unlike influenza which has segments]
- Closely related to human measles virus and rinderpest virus of cattle — all in genus Morbillivirus
Surface Proteins (critical for pathogenesis and immunity):
- H protein (Hemagglutinin) [attaches virus to host cell receptors — primary target for vaccine-induced antibodies]
- F protein (Fusion protein) [allows virus to fuse with host cell membrane and enter; also responsible for syncytia formation (merging of cells)]
- M protein (Matrix protein) [links envelope to nucleocapsid; important for viral budding out of cells]
2. EPIDEMIOLOGY (Who Gets It, Where, When)
Host Range
CDV has one of the broadest host ranges of any carnivore pathogen:
| Animal Group | Examples |
|---|
| Canidae [dog family] | Dogs, wolves, foxes, coyotes, jackals |
| Mustelidae [weasel family] | Ferrets, mink, otters, badgers, skunks |
| Procyonidae [raccoon family] | Raccoons, coatis |
| Felidae [cat family] | Large wild cats (lions, tigers, leopards) — domestic cats are NOT susceptible |
| Ursidae [bear family] | Bears |
| Marine mammals | Seals, dolphins (closely related morbilliviruses) |
| Non-human primates | Experimentally susceptible |
Key fact for exams: Domestic cats do NOT get canine distemper. If you see cat + systemic disease + neurological signs, think Feline Panleukopenia or FIP, not CD.
Age Predisposition
- Young, unvaccinated puppies (3–6 months) are most susceptible — maternal antibody (antibody passed from mother to puppy through milk/colostrum) wanes by 6–16 weeks
- Dogs of any age can be affected if unvaccinated
- Ferrets are extremely susceptible — nearly 100% fatal
Transmission
- Primary route: Aerosol / respiratory droplets [tiny droplets from coughing, sneezing, breathing]
- Direct contact with oronasal secretions [mouth/nose discharge], urine, feces, conjunctival secretions [eye discharge]
- Transplacental transmission [mother to fetus through placenta] — can cause abortion, stillbirths, or neonatal CD
- No tick or mosquito transmission — direct contact only
- Fomites [contaminated objects] play a minor role — virus is fragile in environment
- Shedding starts ~7 days after infection, before clinical signs appear
Environmental Survival
- Destroyed at 50–60°C in 30 minutes
- Sensitive to UV light, desiccation (drying), and common disinfectants (bleach 1:30, quaternary ammonium compounds)
- Survives only a few hours at room temperature outside the host
- Can survive weeks at freezing temperatures (0–4°C)
3. PATHOGENESIS — Step by Step (How the Virus Causes Disease)
This is the most important section to understand conceptually.
EXPOSURE (inhaled virus)
↓
Virus lands in UPPER RESPIRATORY TRACT
↓
Replicates in EPITHELIAL CELLS of tonsils and bronchial lymph nodes (Day 1–4)
↓
FIRST VIREMIA [virus enters bloodstream for the first time] (Day 4–6)
Infects monocytes and lymphocytes [white blood cells — immune cells]
↓
Spreads to ALL LYMPHOID ORGANS:
Spleen, lymph nodes, thymus, bone marrow, gut-associated lymphoid tissue (GALT)
↓
LYMPHOPENIA [drop in lymphocytes = severe immunosuppression]
This is why secondary bacterial infections are common in CD
↓
SECOND VIREMIA [virus re-enters blood in large quantities] (Day 8–14)
↓
Virus spreads to EPITHELIAL TISSUES and NERVOUS SYSTEM:
→ Respiratory epithelium [lungs, trachea]
→ GI epithelium [stomach, intestines]
→ Urinary epithelium [bladder, kidneys]
→ Skin
→ Eyes (uvea, retina, optic nerve)
→ CNS [central nervous system = brain and spinal cord]
↓
OUTCOME depends on IMMUNE RESPONSE:
Immune Response vs. Outcome Table
| Immune Response | Outcome |
|---|
| Strong humoral (antibody) response by day 9–14 | Virus cleared — dog recovers, no neurological signs |
| Moderate immune response | Virus cleared from visceral organs but persists in CNS and skin → Late neurological disease, hyperkeratosis |
| Poor immune response | Overwhelming systemic infection → Death |
Why does CDV cause nervous system disease? The nervous system acts as an immune-privileged site [area where the immune system has limited access]. The virus hides there even after the body has cleared it elsewhere. Additionally, CDV directly infects oligodendrocytes [cells that make myelin — the insulating sheath around nerves], causing demyelination [loss of myelin = like stripping the insulation from an electrical wire — nerve signals fail].
4. CLINICAL SIGNS — Complete System by System
CDV is called the "great mimicker" because it can look like many other diseases. Signs appear in phases.
Phase 1 — Initial / Prodromal Stage (Days 3–6 post-infection)
- Fever (biphasic — two fever spikes): First spike at days 3–4, drops, then rises again at days 11–14
- Serous (watery) ocular discharge
- Nasal discharge (serous initially)
- Anorexia (not eating)
- Lethargy / depression
- Mild cough
Biphasic fever is an early suspicious sign for CD — not pathognomonic alone but clinically very suggestive.
Phase 2 — Respiratory Phase
- Mucopurulent (thick, pus-like) nasal discharge [progresses from watery to yellow-green as secondary bacterial infection sets in]
- Mucopurulent ocular discharge → conjunctivitis [inflammation of eye lining]
- Dry to moist cough
- Dyspnea (difficulty breathing) — interstitial pneumonia [inflammation of lung tissue between air sacs]
- Crackles/wheezes on lung auscultation [listening with stethoscope]
Phase 3 — Gastrointestinal Phase
- Vomiting
- Diarrhea (may be bloody — hemorrhagic)
- Anorexia, weight loss, dehydration
Phase 4 — Skin / Cutaneous Signs
- Pustular (pus-filled) skin rash — especially on abdomen/inner thighs
- Hyperkeratosis of nasal planum and footpads [thickening and hardening of the nose leather and paw pads — the famous "hard pad disease"]
⭐ PATHOGNOMONIC SIGN #1: "Hard Pad Disease" — Hyperkeratosis (extreme hardening/thickening) of the nasal planum and footpads. When you see a dog with rock-hard, cracked nasal planum and footpads + other systemic signs, think CDV FIRST.
Phase 5 — Ophthalmic (Eye) Signs
- Conjunctivitis [eye lining inflammation]
- Keratoconjunctivitis sicca (KCS / dry eye) [reduced tear production]
- Uveitis [inflammation inside the eye]
- Optic neuritis [inflammation of optic nerve → sudden blindness]
- Chorioretinitis [inflammation of retina — on fundic exam shows gray-tan foci]
⭐ Chorioretinal lesions (gray "punched-out" lesions on the retina) on fundic examination are highly suspicious for CDV.
Phase 6 — Neurological Signs (CDV Encephalomyelitis)
This is the most serious phase and can occur during acute systemic disease OR weeks/months later (post-infectious).
Types of CDV Neurological Disease:
A. Acute Encephalomyelitis [brain + spinal cord inflammation] in Young Dogs
- Myoclonus [rhythmic, repetitive, involuntary muscle twitching — "chewing gum fits"]
- Seizures
- Ataxia [loss of coordination/balance — wobbly gait]
- Paresis / paralysis [partial or complete loss of limb movement]
- Hypermetria [exaggerated, overstepping gait seen with cerebellar disease]
- Head tilt, nystagmus [abnormal rapid eye movement]
- Behavioral changes — aggression, pacing, circling
⭐ PATHOGNOMONIC SIGN #2: Myoclonus (Flexor Spasm / "Chewing Gum Fits") — Rhythmic, repetitive muscle jerking that continues even during sleep. This is nearly pathognomonic for CDV. It occurs because CDV infects the brainstem and spinal cord neurons.
B. Old Dog Encephalitis (ODE) — Rare
- Occurs in adult/older dogs with previous CDV exposure or vaccination
- Slowly progressive neurological deterioration
- Cognitive decline, blindness, seizures
- No systemic signs — neurological only
C. Post-Vaccinal Encephalitis — Very Rare
- Occurs 1–2 weeks after modified live virus (MLV) vaccination in very young (<4 weeks) or immunocompromised dogs
- The vaccine virus replicates in the CNS
Phase 7 — Dental Enamel Hypoplasia ["enamel defect"]
- If CDV infects puppies during tooth development (3–7 weeks), it destroys ameloblasts [cells that form tooth enamel]
- Results in pitted, brown-stained teeth with incomplete enamel → permanent lesion visible in adult dogs
- Important retrospective clue: "This adult dog had CDV as a puppy"
5. INCLUSION BODIES — Histopathology [Microscopic Findings]
One of the most important diagnostic features of CDV:
- Eosinophilic intracytoplasmic and intranuclear inclusion bodies [pink-staining blobs found inside the cell body AND inside the nucleus]
- Found in:
- Epithelial cells of respiratory, urinary, and GI tracts
- Neurons and glial cells [brain support cells]
- Leukocytes (lymphocytes, monocytes) in blood smears — detectable early in infection
CDV is one of the FEW viruses that produces BOTH intracytoplasmic AND intranuclear inclusion bodies. Most viruses produce only one type. This is diagnostically very useful.
Classically called "Lentz bodies" (intranuclear in neurons) and "Sinigaglia bodies" (intracytoplasmic in epithelial cells).
6. DIAGNOSIS — How to Confirm CDV
A. Clinical Diagnosis (Field Diagnosis)
Suspect CDV in an unvaccinated young dog with:
- Biphasic fever
- Mucopurulent oculonasal discharge
- Respiratory + GI signs
- Myoclonus
- Hard pad disease
B. Laboratory Diagnosis
| Test | Sample | What It Detects | Notes |
|---|
| RT-PCR (Reverse Transcriptase PCR) [gold-standard molecular test] | Conjunctival swab, nasal swab, urine, CSF, blood | Viral RNA | Most sensitive and specific |
| Immunofluorescence (IFA/IFT) [antibody-based staining of cells] | Conjunctival smear, buffy coat [white blood cell layer] | Viral antigen in cells | Early diagnosis, quick |
| ELISA / Rapid antigen test | Nasal/conjunctival swab, urine | Viral antigen | In-clinic test, less sensitive |
| Serology (virus neutralization, IgM) | Serum | Antibody titers | Paired samples (acute + convalescent) for 4× rise in titer; IgM = acute infection |
| CSF analysis [cerebrospinal fluid analysis] | CSF tap | Increased protein, lymphocytes; CDV PCR | For neurological cases |
| Histopathology [microscopic tissue examination] | Tissue biopsy (brain, lung, bladder) | Inclusion bodies, demyelination | Post-mortem definitive diagnosis |
| Buffy coat smear | EDTA blood | Intracytoplasmic inclusion bodies in leukocytes | Simple, early, not always positive |
C. Hematology / Blood Work Findings
- Lymphopenia [low lymphocytes] — early and consistent finding
- Thrombocytopenia [low platelets] — common
- Mild non-regenerative anemia
- Elevated liver enzymes if hepatic involvement
- Elevated CSF protein and cells if neurological
D. Imaging
- Thoracic radiographs: Interstitial to alveolar pattern [diffuse lung haziness] — indicates viral pneumonia
- MRI of brain: Demyelinating lesions in white matter [areas of myelin loss show as bright spots on T2-weighted sequences]
7. DIFFERENTIAL DIAGNOSIS — How to Tell CDV Apart From Other Diseases
This is a critical clinical skill:
CDV vs. Canine Infectious Respiratory Disease Complex (CIRDC / "Kennel Cough")
| Feature | CDV | Kennel Cough |
|---|
| Systemic signs | YES — multisystemic | Minimal — mainly cough |
| Neurological signs | Common | Absent |
| GI signs | Common | Absent |
| Nasal discharge | Mucopurulent | Mild serous |
| Hard pad | YES | NO |
| Fever | Biphasic, high | Mild or absent |
| History | Unvaccinated | Often vaccinated, shelter/kennel |
| Key organism | CDV | Bordetella, CIV, CPI, Mycoplasma |
CDV vs. Parvovirus (CPV)
| Feature | CDV | Parvovirus |
|---|
| Primary system | Multi-system (resp + neuro + GI) | Primarily GI + bone marrow |
| Respiratory signs | YES | Absent |
| Neurological signs | YES | Absent |
| Hemorrhagic diarrhea | Possible | Classic — profuse, bloody, foul |
| Leukopenia type | Lymphopenia | Profound leukopenia (all WBCs) |
| Age | <1 year mainly | <1 year |
| Myoclonus | YES | NO |
| Vaccine | MLV combo | MLV combo |
CDV vs. Rabies (Neurological Phase)
| Feature | CDV | Rabies |
|---|
| Systemic signs before neuro | YES | Sometimes prodromal only |
| Myoclonus | YES — characteristic | NO |
| Hydrophobia/aggression | NO (atypical) | YES — classical |
| Ascending paralysis | Sometimes | YES (dumb form) |
| Hard pad | YES | NO |
| Inclusion bodies | Intranuclear + intracytoplasmic | Negri bodies (intracytoplasmic, neurons) |
| Zoonotic risk | NO | YES |
Critical differential: Rabies must always be on your list for any dog with neurological signs + behavior change. CDV myoclonus (rhythmic, repetitive) is different from the random seizures/aggression of rabies.
CDV vs. Toxoplasmosis (CNS form)
| Feature | CDV | Toxoplasmosis |
|---|
| Cause | Virus | Toxoplasma gondii (protozoan parasite) |
| Respiratory | YES | YES |
| Myoclonus | YES | Possible but less characteristic |
| Diagnosis | PCR, antigen test | Serology (IgM/IgG), PCR |
| Treatment available? | No specific antiviral | YES — clindamycin, trimethoprim-sulfa |
CDV vs. GME (Granulomatous Meningoencephalitis) [immune-mediated brain inflammation]
| Feature | CDV | GME |
|---|
| Age | Young, unvaccinated | Young to middle-aged |
| Systemic signs | YES | Minimal |
| Vaccine status | Unvaccinated | Usually vaccinated |
| CSF | Lymphocytic pleocytosis, CDV PCR positive | Lymphocytic pleocytosis, infectious PCRs negative |
| Treatment | Supportive | Immunosuppressive (steroids) |
8. PATHOGNOMONIC SIGNS SUMMARY ⭐
These are the signs that point specifically to CDV:
| Sign | Description |
|---|
| Myoclonus | Repetitive, rhythmic muscle jerking — continues during sleep — nearly pathognomonic |
| Hyperkeratosis of nasal planum + footpads ("Hard Pad Disease") | Rock-hard, cracked paw pads and nose leather |
| Enamel hypoplasia [incomplete tooth enamel] | Brown-pitted teeth — retrospective marker of puppy CDV infection |
| Intranuclear + Intracytoplasmic inclusion bodies | Both locations — seen on histology |
| Chorioretinal lesions | Gray "punched-out" lesions on fundic exam |
| Biphasic fever + multisystemic signs in unvaccinated puppy | Clinical combination highly specific |
9. TREATMENT — There Is No Specific Antiviral
CDV has no approved antiviral drug — treatment is entirely supportive and symptomatic.
Supportive Care
- IV fluid therapy [intravenous fluids] — correct dehydration, maintain electrolyte balance
- Nutritional support — force feeding, feeding tube if not eating
- Antiemetics [drugs to stop vomiting]: Maropitant (Cerenia), metoclopramide
- Antidiarrheals / GI protectants: Kaolin-pectin, sucralfate
Antibiotics (for Secondary Bacterial Infections)
- Broad-spectrum: Amoxicillin-clavulanate, Enrofloxacin, Trimethoprim-sulfa
- Essential because CDV causes immunosuppression → secondary pneumonia, pyoderma, enteritis
Neurological Management
- Phenobarbital or potassium bromide — for seizure control
- Methocarbamol [muscle relaxant] — for myoclonus (temporary relief, not curative)
- Dexamethasone [corticosteroid] — controversial; may reduce CNS inflammation but can worsen immunosuppression
- Vitamin supplementation (B vitamins) — neurological support
Experimental / Emerging Treatments
- Ribavirin — showed in-vitro [laboratory] activity but clinical use limited due to toxicity
- Human IV immunoglobulin — experimental in severe cases
- Interferon — some reports in Japan using feline interferon omega (Virbagen Omega)
Prognosis
| Stage | Prognosis |
|---|
| Respiratory/GI only | Guarded to fair — 50% recovery with intensive care |
| Neurological signs present | Guarded to poor |
| Severe myoclonus + demyelination | Poor — persistent neurological deficits even if survives |
| Ferrets | Nearly always fatal |
Key rule: Once severe neurological signs (myoclonus, ataxia, seizures) are present for more than 2–3 weeks, the prognosis is very poor and humane euthanasia should be discussed with the owner.
10. VACCINATION — Prevention
Vaccine Types
- Modified Live Virus (MLV) vaccine [attenuated = weakened live virus] — gold standard; provides best long-lasting immunity
- Recombinant canarypox-vectored CDV vaccine [CDV gene inserted into canarypox virus] — safer in immunocompromised animals, ferrets, and exotic carnivores; does not replicate in mammals
Core Vaccine — DHPP or DA2PP
CDV vaccine is a core vaccine (all dogs must receive it regardless of lifestyle):
- D = Distemper
- H or A2 = Hepatitis (Adenovirus type 2)
- P = Parvovirus
- P = Parainfluenza (sometimes included)
Schedule
| Age | Vaccination |
|---|
| 6–8 weeks | First MLV puppy vaccine |
| 10–12 weeks | Booster |
| 14–16 weeks | Final puppy series booster |
| 1 year later | Adult booster |
| Every 3 years | Adult revaccination (WSAVA guidelines) |
Why start at 6–8 weeks? Maternal antibodies (MDA) [antibodies passed from mother to puppy] interfere with vaccine response. They begin waning at 6 weeks. The series covers the "window of susceptibility" — when MDA is too low to protect but vaccine response may be blocked. This is the most dangerous period for CDV infection.
Vaccination Failures — Why Can a Vaccinated Dog Get CDV?
- Maternal antibody interference — puppy vaccinated too early, MDA blocks vaccine
- Incomplete series — missed boosters
- Improper storage — MLV vaccine must be kept at 2–7°C; inactivated by heat, UV light, or freezing
- Immunosuppression at time of vaccination
- Rare vaccine strain mismatch — CDV has genetically diverse strains globally
11. PATHOLOGY — Post-Mortem Findings
Gross Pathology [what you see with the naked eye]
- Lungs: Consolidation [solidified, firm tissue], red-gray discoloration — interstitial pneumonia
- Brain: Softening (malacia) [tissue necrosis], grayish-yellow areas of demyelination
- Nasal planum + footpads: Hyperkeratosis — thickened, cracked
- Lymph nodes: Atrophy [shrinkage due to lymphocyte depletion]
- Thymus: Atrophy in young dogs — "thymic atrophy"
- Teeth: Enamel hypoplasia (if infection occurred during tooth development)
- Eyes: Chorioretinal scars
Histopathology [microscopic findings]
- Lung: Interstitial pneumonia; syncytia [giant multinucleated cells — formed by F protein-mediated cell fusion]; inclusion bodies in bronchial epithelium
- Brain: Perivascular cuffing [accumulation of lymphocytes around blood vessels — indicates inflammation]; demyelination; intranuclear and intracytoplasmic inclusion bodies in neurons and glial cells
- Lymphoid tissue: Lymphocyte depletion, necrosis
- Bladder epithelium: Inclusion bodies — useful diagnostic sample
- Inclusion bodies: Eosinophilic, found in both nucleus and cytoplasm of multiple cell types
12. PUBLIC HEALTH & ZOONOTIC POTENTIAL
- CDV is NOT zoonotic [does not infect humans under natural conditions]
- However, it is closely related to measles virus — historically may have jumped from ancestral morbillivirus to humans thousands of years ago
- No risk to human handlers, owners, or veterinary staff from infected dogs
- Risk to other animals: Ferrets, wild carnivores, big cats must be protected from exposure by infected dogs
13. IMPORTANT CLIENT QUESTIONS (What Owners Ask)
Here are the most common, important questions clients ask — and how to answer them:
Q1: "My dog is vaccinated — can he still get distemper?"
Yes, rarely. Vaccination greatly reduces risk but is not 100% guaranteed, especially if the puppy series was incomplete, if the vaccine was stored incorrectly, or if the dog was immunosuppressed at the time of vaccination. However, vaccinated dogs that do get CDV tend to have much milder disease.
Q2: "Is distemper contagious to my other dogs or my cats?"
Yes, it is highly contagious to other unvaccinated dogs and to ferrets. However, domestic cats are NOT susceptible to CDV. Isolate the sick dog immediately from other dogs.
Q3: "My puppy has a twitching leg that doesn't stop even when sleeping — what is that?"
That is myoclonus — a classic sign of CDV nervous system involvement. It is caused by the virus damaging the brainstem and spinal cord. Unfortunately, once myoclonus develops, it is often permanent even if the dog survives.
Q4: "Can distemper be cured?"
There is no specific antiviral drug for distemper. Treatment is supportive — fluids, antibiotics for secondary infections, seizure medications. Some dogs recover from the respiratory and GI forms, but severe neurological cases carry a poor prognosis.
Q5: "Is distemper the same as rabies?"
No. Both affect the nervous system but they are completely different diseases caused by different viruses. Rabies is caused by a Lyssavirus, is always fatal once symptoms appear, and is zoonotic (can infect humans). Distemper is caused by CDV, is not zoonotic, and some dogs do recover.
Q6: "My puppy survived distemper — will the twitching ever go away?"
Myoclonus from CDV is usually permanent — the neuronal damage does not fully repair. Some mild cases may improve slightly over months, but complete resolution is uncommon. The dog can often still have acceptable quality of life depending on severity.
Q7: "My puppy has distemper — should I euthanize?"
This depends on the severity. If signs are limited to respiratory and GI systems and the dog is responsive to treatment, recovery is possible with intensive care. If the dog has severe, progressive neurological signs (uncontrolled seizures, inability to walk, loss of consciousness), euthanasia may be the most humane option and should be honestly discussed.
Q8: "When should puppies be vaccinated?"
Starting at 6–8 weeks, then every 3–4 weeks until 16 weeks old. This series is critical because of the maternal antibody window. Missing even one booster leaves a puppy vulnerable during the highest-risk period.
Q9: "My puppy's teeth are brown and pitted — why?"
If the dog had CDV infection as a puppy during the period of tooth development (3–7 weeks of age), the virus destroys enamel-forming cells (ameloblasts), leading to permanent enamel hypoplasia — brown, pitted, weak teeth. This is a permanent retrospective marker of early CDV infection.
Q10: "Can wild animals spread distemper to my dog?"
Yes. Raccoons, foxes, coyotes, and other wild carnivores can all carry and shed CDV. Dogs that roam outdoors, especially near wildlife, are at risk. This is another reason to keep vaccination current.
14. QUICK CONCEPT SUMMARY TABLE
| Feature | CDV Detail |
|---|
| Virus type | Enveloped, ssRNA, negative-sense, Morbillivirus |
| Most susceptible | Unvaccinated puppies 3–6 months |
| Transmission | Aerosol / direct contact |
| Environmental survival | Hours at room temperature; weeks at freezing |
| Pathognomonic sign | Myoclonus + Hard pad disease |
| Lymphopenia | Early, consistent, causes immunosuppression |
| Inclusion bodies | Both intranuclear AND intracytoplasmic |
| Most useful early test | RT-PCR (conjunctival/nasal swab) |
| Treatment | Supportive only — no specific antiviral |
| Core vaccine | DHPP / DA2PP — MLV or recombinant |
| Zoonotic? | NO |
| Domestic cats susceptible? | NO |
| Ferret prognosis? | Nearly always fatal |
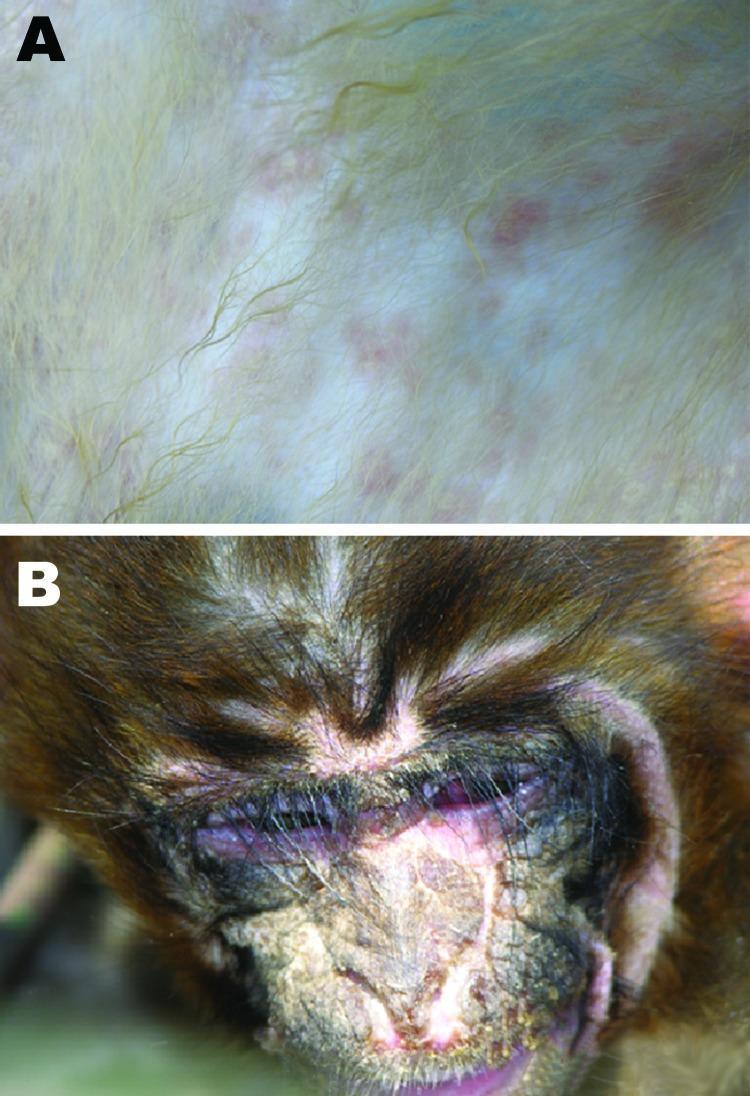
Clinical Image — CDV manifestations (maculopapular skin rash, suppurative conjunctivitis, nasal crusting):
Panel A: Maculopapular skin rash — discrete rosy to purple macules under the fur. Panel B: Severe suppurative conjunctivitis with thick purulent discharge matting the eyelids, periorbital swelling, and ulcerated/crusting lesions on the nasal bridge — classic CDV epithelial tropism.
This covers every major aspect of Canine Distemper from molecular virology to client communication. If you want, I can go deeper into any specific section — neurological pathology, vaccine immunology, or CSF analysis interpretation — just ask.