Now I have enough to write a comprehensive, authoritative answer. The library confirms CDV's classification as a Morbillivirus (same genus as measles), and I have clinical images. Let me now deliver the full, detailed explanation from my veterinary knowledge base.
CANINE DISTEMPER (CD) — Complete Veterinary Guide
1. ETIOLOGY (Cause / Wajah)
Canine Distemper Virus (CDV) is a single-stranded, negative-sense RNA virus belonging to:
- Family: Paramyxoviridae
- Genus: Morbillivirus (same genus as human measles/rubeola virus, rinderpest virus of cattle, and phocine distemper virus of seals)
- Structure: Enveloped, pleomorphic (irregular shape), ~150–300 nm in diameter
- Genome: Non-segmented, ~15.7 kb
- Key surface proteins:
- H protein (Hemagglutinin) — attaches to host cell receptor (SLAM/CD150 on immune cells; nectin-4 on epithelial cells)
- F protein (Fusion protein) — fuses viral envelope with host cell membrane, enabling cell entry
- M protein (Matrix protein) — essential for viral assembly and budding
Important concept: CDV is antigenically related to measles virus. Dogs that survived distemper historically had some cross-protection against measles, and early measles vaccines were used experimentally in dogs. This cross-reactivity is diagnostically important.
Only ONE serotype exists, but multiple genotypes (lineages) are recognized globally: America-1, America-2, Europe-1 (wildlife), Arctic, Asia-1, etc. Vaccine strains belong primarily to America-1.
2. EPIDEMIOLOGY (Phelaav / Phailnay ka tareeqa)
Host Range
CDV has one of the broadest host ranges of any viral pathogen:
- Canidae: Dogs, wolves, foxes, coyotes, jackals (most susceptible)
- Mustelidae: Ferrets (highly susceptible, used as experimental model), minks, otters, badgers, weasels
- Procyonidae: Raccoons, coatis
- Ursidae: Bears
- Hyenidae: Hyenas
- Felidae: Large wild cats (lions, tigers, leopards) — domestic cats are resistant
- Non-human primates: Some species susceptible
Key point: Domestic cats do NOT get clinical distemper. If you see a "cat distemper" case — that is Feline Panleukopenia (caused by Feline Parvovirus), a completely different disease. Do not confuse.
Transmission
- Primary route: Aerosol / respiratory droplets (most common)
- Oronasal contact with secretions: nasal discharge, ocular discharge, urine, feces, saliva
- Transplacental (vertical) transmission — can cause stillbirths, neonatal deaths, abortion
- NOT transmitted by vectors (no arthropod involvement)
- Fomites: Virus survives poorly in the environment. Inactivated within hours at room temperature, rapidly destroyed by heat, drying, and common disinfectants (bleach 1:30, quaternary ammonium, UV light)
Susceptibility
- Most susceptible: Unvaccinated puppies 3–6 months of age (when maternal antibody [MDA] wanes)
- Maternal antibody (MDA) provides protection from ~6–16 weeks; timing of vaccination must account for MDA interference
- No breed predisposition, though unvaccinated dogs of any age are at risk
- Morbidity: High in unvaccinated populations (up to 100% exposure under certain conditions)
- Mortality: Variable — 50% in dogs, near 100% in ferrets and black-footed ferrets
Seasonality
- No strict seasonality, but outbreaks often occur in autumn/winter when wildlife populations are stressed and in contact with domestic dogs
3. PATHOGENESIS (Bimari kaise lagti hai — step by step)
This is the most important conceptual section. Understanding pathogenesis explains every clinical sign.
Step 1 — Entry (Day 0–4)
- Virus enters via oronasal route through inhalation of infected aerosols
- Initial replication occurs in macrophages (a type of white blood cell / phagocyte) and dendritic cells (antigen-presenting immune cells) in the upper respiratory tract
- Virus spreads to tonsils and bronchial/retropharyngeal lymph nodes (lymph nodes near the throat)
Step 2 — Primary Viremia (Day 2–4)
- Viremia (virus circulating in blood) develops as CDV spreads via lymphatics and blood
- Virus infects lymphoid organs throughout the body: spleen, thymus, lymph nodes, bone marrow, Peyer's patches (lymphoid tissue in the intestine)
- Critical consequence: CDV destroys lymphocytes (T cells and B cells) → profound immunosuppression (immune system crash)
- This immunosuppression is WHY secondary bacterial infections are so common in distemper
Step 3 — Immune Response Check (Day 6–9)
Two outcomes possible at this stage:
| Immune Response | Outcome |
|---|
| Strong — Virus cleared before Day 9 | Subclinical or mild infection, full recovery |
| Weak/Absent — Virus not cleared | Continued spread, systemic disease |
Step 4 — Secondary Viremia (Day 8–14)
- In dogs with weak immunity, virus spreads from lymphoid tissue to epithelial cells of:
- Respiratory tract (bronchi, bronchioles)
- GI tract (intestinal epithelium)
- Urogenital tract (kidney tubules, bladder)
- Skin (footpads, nose)
- Eyes (conjunctiva, uvea)
- CNS (brain, spinal cord)
- Teeth (enamel-forming cells — ameloblasts)
Step 5 — Tissue Damage
- Virus directly destroys epithelial and nerve cells
- Immune-mediated damage also contributes significantly, especially in the CNS — demyelination (destruction of myelin sheath around nerve fibers) is partly caused by the immune system attacking CDV-infected oligodendrocytes (myelin-producing cells)
4. CLINICAL SIGNS (Symptoms)
CDV causes a multisystemic disease with signs in multiple organ systems. The classic presentation is described in phases:
Phase 1 — Acute Febrile Phase (Days 3–8)
- Biphasic fever ⭐ (PATHOGNOMONIC CLUE):
- First spike: 39.5–41°C (103–106°F) at Day 3–4
- Fever drops, then rises again ~Day 11–14 when secondary viremia begins
- Anorexia (loss of appetite)
- Lethargy, depression
- Mild serous (watery) nasal and ocular discharge
Phase 2 — Respiratory Signs
- Mucopurulent (thick, green/yellow, pus-containing) nasal discharge — due to secondary bacterial infection (because immune system is crashed)
- Mucopurulent conjunctivitis (eye discharge)
- Coughing — often moist/productive
- Dyspnea (difficulty breathing)
- Interstitial pneumonia (lung inflammation involving the spaces around air sacs)
- Bronchopneumonia (common due to secondary bacteria: Bordetella bronchiseptica, Pasteurella, streptococci)
Phase 3 — Gastrointestinal Signs
- Vomiting
- Diarrhea (may be hemorrhagic/bloody in severe cases)
- Dehydration
- Weight loss
Phase 4 — Dermatological Signs
- Hyperkeratosis of footpads ⭐⭐ (PATHOGNOMONIC — "Hard Pad Disease"):
- Footpads become extremely hard, thickened, and hyperkeratotic (excessive keratin production)
- Also affects the nasal planum (the "nose tip")
- This is THE most recognizable gross sign of CDV in a live dog
- Vesicular/pustular skin rash (blistering rash on abdomen, inner thighs) — early sign, often missed
- Secondary pyoderma (bacterial skin infection)
Phase 5 — Ocular Signs
- Keratoconjunctivitis sicca (KCS / dry eye — reduced tear production)
- Uveitis (inflammation inside the eye)
- Chorioretinitis (inflammation of the choroid and retina)
- "Sunken gray lesions" on the retina / retinal degeneration — visible on funduscopic exam ⭐
- Optic neuritis → blindness
- Corneal ulcers
Phase 6 — Neurological Signs (Worst prognosis)
Neurological signs may occur simultaneously with systemic signs, or weeks to months AFTER apparent recovery. Three forms:
A. Polioencephalomyelitis (Gray matter disease — in young puppies)
- Seizures ("chewing gum fits" — rhythmic jaw movements) ⭐⭐ PATHOGNOMONIC for CD in puppies
- Myoclonus (involuntary rhythmic muscle twitching/jerking) ⭐⭐ — the MOST pathognomonic neurological sign
- Hyperesthesia (extreme sensitivity to touch/sound/light)
- Cerebellar ataxia (wobbling, incoordination)
- Head tilt, nystagmus (abnormal eye movement)
- Paresis/paralysis (weakness/loss of movement)
B. Leukoencephalomyelitis (White matter demyelinating disease — in older dogs)
- Progressive ataxia (incoordination worsening over weeks)
- Paresis progressing to paralysis
- Behavioral changes
- Vestibular signs
C. Old Dog Encephalitis (ODE)
- Rare, chronic, progressive encephalitis (brain inflammation) in middle-aged to older, previously vaccinated dogs
- Associated with persistent virus in the CNS
- Signs: progressive behavioral changes, vision loss, pacing, compulsive circling, dementia-like signs
- Poorly responsive to treatment
Phase 7 — Dental Signs (in surviving puppies)
- Enamel hypoplasia ⭐ — pitting, discoloration, erosion of tooth enamel
- Caused by CDV destroying ameloblasts (enamel-forming cells) during tooth development
- Seen in dogs that survived CDV infection as puppies
- Permanent, irreversible — used as a historical marker of distemper infection
5. PATHOGNOMONIC SIGNS SUMMARY ⭐⭐
| Sign | Significance |
|---|
| Myoclonus (rhythmic muscle twitching, especially limbs) | Most pathognomonic neurological sign of CD |
| Hard pad disease (footpad & nasal hyperkeratosis) | Most recognizable gross sign |
| "Chewing gum fits" (rhythmic jaw seizures in puppies) | Highly specific for CD |
| Biphasic fever | Early clue during acute phase |
| Enamel hypoplasia in permanent teeth | Historical marker in recovered dogs |
| Sunken gray retinal lesions (funduscopy) | Ocular pathognomonic finding |
6. PATHOLOGY (What you find at necropsy/biopsy)
Gross Lesions
- Lungs: Interstitial pneumonia, consolidation, gray-pink coloration, failure to collapse
- Lymph nodes/Spleen/Thymus: Atrophy (shrinkage) — due to lymphocyte destruction
- Footpads/Nose: Hard, rough, hyperkeratotic
- Skin: Vesicles/pustules on ventrum
- Brain: Gross lesions often absent; sometimes softening/discoloration of white matter
Histopathology (Microscopic findings)
- Intranuclear AND intracytoplasmic inclusion bodies ⭐⭐ (Lentz inclusion bodies):
- Found in epithelial cells of respiratory tract, urinary bladder, conjunctiva, bile ducts
- Also found in neurons and glial cells of the CNS
- Eosinophilic (pink-staining) inclusions on H&E stain
- These are aggregates of viral nucleocapsids (packaged viral genetic material)
- Demyelination of white matter in the CNS — loss of myelin, vacuolation (empty spaces in nerve tissue)
- Perivascular cuffing (accumulation of lymphocytes around blood vessels in the brain) — indicates immune-mediated inflammation
- Syncytia (multinucleated giant cells) in respiratory and lymphoid tissues — formed when CDV fuses multiple cells together
7. DIAGNOSIS (Teşhis / Pehchaan)
Clinical Diagnosis
- Young unvaccinated dog + multisystemic signs + myoclonus + hard pad + mucopurulent discharge = presumptive CDV
Laboratory Diagnosis
A. Hematology (Blood count)
- Lymphopenia (low lymphocyte count) — early, consistent finding due to CDV destroying lymphocytes ⭐
- Leukopenia (low white blood cell count) in acute phase
- Later: neutrophilia (high neutrophils) due to secondary bacterial infection
B. Inclusion Body Detection
- Conjunctival/nasal smear, buffy coat smear, CSF smear:
- Stain with H&E or Giemsa
- Look for intracytoplasmic eosinophilic inclusion bodies in lymphocytes/epithelial cells
- Sensitivity: low (~30–50%), but highly specific when found
C. Serology
- Serum neutralization (SN) test — gold standard for antibody detection
- ELISA for CDV antibodies
- Important limitation: Vaccinated dogs also have antibodies → cannot differentiate vaccine response from natural infection by serology alone
D. PCR (Polymerase Chain Reaction) ⭐ Best test
- Most sensitive and specific test
- Can be run on:
- Conjunctival/nasal swabs
- Blood (buffy coat)
- Urine
- CSF (cerebrospinal fluid)
- Tissue samples post-mortem
- Real-time RT-PCR (because CDV has RNA genome, you need reverse transcriptase first to convert RNA → DNA)
E. Immunofluorescence (IFA) / Immunohistochemistry (IHC)
- Antigen detection in tissue sections
- Gold standard for post-mortem confirmation
- Fluorescent antibodies bind to CDV antigen in tissue
F. Virus Isolation
- Most definitive, but slow and expensive
- Requires specialized cell culture (Vero cells)
- Rarely done in clinical practice
G. CSF Analysis (for neurological cases)
- Elevated protein (>25 mg/dL)
- Pleocytosis (increased cells — mainly mononuclear) — lymphocytic inflammation
- CDV-specific antibodies in CSF > serum → indicates intrathecal (within the CNS) antibody production → active CNS infection
Rapid in-clinic test
- Lateral flow assay (LFA) / rapid antigen test — available for CDV antigen detection (similar to COVID rapid test concept)
- Detects CDV antigen in ocular/nasal secretions or blood
- Sensitivity varies, useful as a screening tool
8. DIFFERENTIAL DIAGNOSIS (Farq karna — How to differentiate from similar diseases)
This is critical for the clinician:
| Disease | Similarities with CD | Key Differences |
|---|
| Canine Infectious Tracheobronchitis (Kennel Cough) | Cough, nasal discharge | No systemic signs, no neuro signs, no hard pad; Bordetella bronchiseptica ± CPI/CAV-2 etiology; self-limiting |
| Canine Parvovirus (CPV) | Fever, anorexia, vomiting, bloody diarrhea, leukopenia | No respiratory signs, no neuro signs, no hard pad; severe hemorrhagic gastroenteritis; fecal antigen ELISA positive |
| Canine Infectious Hepatitis (CAV-1) | Fever, lethargy, vomiting, ocular signs | "Blue eye" (corneal edema = hallmark); elevated liver enzymes; no hard pad, no myoclonus; intranuclear inclusions in hepatocytes |
| Leptospirosis | Fever, lethargy, vomiting, renal signs | Icterus (jaundice); acute kidney/liver failure; no respiratory signs; serology positive; antibiotic responsive |
| Toxoplasmosis | Neurological signs, pneumonia, ocular signs | Can mimic CD closely; often concurrent with CD (CD causes immunosuppression → allows Toxoplasma reactivation); serology/PCR differentiates |
| Rabies | Neurological signs, behavioral changes, paralysis | Progressive, fatal; no respiratory/GI signs; exposure history; no inclusion bodies in distemper sites; Negri bodies in neurons |
| GME (Granulomatous Meningoencephalitis) | Neurological signs | Immune-mediated, no systemic signs, no inclusion bodies, MRI more definitive |
| Thiamine deficiency | Neurological signs, ataxia | Dietary history; no multisystemic signs; responds to thiamine supplementation |
| Lead poisoning | Seizures, vomiting | Exposure history; blood lead levels elevated; basophilic stippling on blood smear |
9. TREATMENT (Ilaaj)
IMPORTANT: There is NO specific antiviral drug approved for CDV. Treatment is entirely supportive and symptomatic.
A. Supportive Care (Most important)
- IV fluid therapy (isotonic crystalloids like Ringer's lactate or Normal Saline) — to correct dehydration and maintain perfusion
- Nutritional support — force feeding or nasoesophageal tube feeding if not eating
- Antipyretics (fever reducers) — use with caution; only if fever is severely high (>40.5°C / 105°F)
- Antiemetics — Maropitant (Cerenia) for vomiting
- Antidiarrheals — probiotics, kaolin-pectin
B. Antibiotics (For secondary infections)
- NOT for the virus itself — CDV is a virus, antibiotics don't kill viruses
- Essential because CDV immunosuppression leads to life-threatening secondary bacterial pneumonia/sepsis
- Amoxicillin-clavulanate, Trimethoprim-sulfa (TMS), Doxycycline (especially if Bordetella co-infection)
- In hospitalized, severe cases: broad-spectrum IV antibiotics (ampicillin-sulbactam, enrofloxacin)
C. Ocular Care
- Artificial tears / lubricating eye drops for KCS
- Topical antibiotics (tobramycin, ciprofloxacin eye drops) for conjunctivitis
- Atropine if uveitis present (to dilate pupil and reduce pain)
D. Neurological Management
- Anticonvulsants for seizures:
- Phenobarbital — drug of choice for seizure control in dogs
- Potassium bromide — add-on therapy for refractory seizures
- Myoclonus: No effective treatment; may persist for life even after recovery
- Procainamide has been tried but results are inconsistent
- Dexamethasone (corticosteroids): Controversial — may reduce CNS inflammation, but also suppresses immune function further; used cautiously in acute demyelinating disease
- Ribavirin: Antiviral, some in vitro (lab) activity against CDV, but poor CNS penetration; not practically used
E. Prognosis
| Clinical Form | Prognosis |
|---|
| Respiratory/GI only | Fair to good with treatment |
| Neurological signs at presentation | Guarded to poor |
| Myoclonus, progressive neuro deficits | Poor; euthanasia often recommended |
| Old Dog Encephalitis | Poor; slowly progressive |
| Recovery with neurological residuals | Variable; deficits often permanent |
10. PREVENTION & VACCINATION
Core Vaccine
- CDV vaccine is a CORE vaccine (recommended for ALL dogs regardless of lifestyle)
- Modified Live Virus (MLV) vaccine — most effective type
- Combined in DA2PPv or DHPPv vaccines:
- D = Distemper
- A2/H = Adenovirus type 2 / Hepatitis
- P = Parvovirus
- P = Parainfluenza
Puppy Vaccination Schedule
| Age | Vaccine |
|---|
| 6–8 weeks | First DA2PPv |
| 10–12 weeks | Second DA2PPv |
| 14–16 weeks | Third DA2PPv |
| 12–16 months | Booster |
| Then every 3 years | Adult booster (based on WSAVA guidelines) |
Why start at 6–8 weeks? Maternal antibodies (MDA) from the mother's colostrum (first milk) protect the puppy early in life but also block vaccine response (MDA interferes with MLV). As MDA wanes, the window opens for vaccination. The series ensures at least one dose "takes" after MDA drops below protective levels — this is called the "window of susceptibility" (gap between MDA falling and vaccination taking effect — dangerous period).
Vaccination Failure Causes
- MDA interference (most common)
- Improper storage (cold chain broken — MLV vaccines must be refrigerated, reconstituted just before use)
- Concurrent immunosuppressive disease at time of vaccination
- Vaccination during incubation period
Disinfection
- CDV is easily killed by:
- Bleach (sodium hypochlorite) 1:30 dilution
- Quaternary ammonium compounds
- Aldehydes (glutaraldehyde, formaldehyde)
- Phenol-based disinfectants
- Heat, UV light, drying
- Survival in environment: hours to days (shorter than parvovirus)
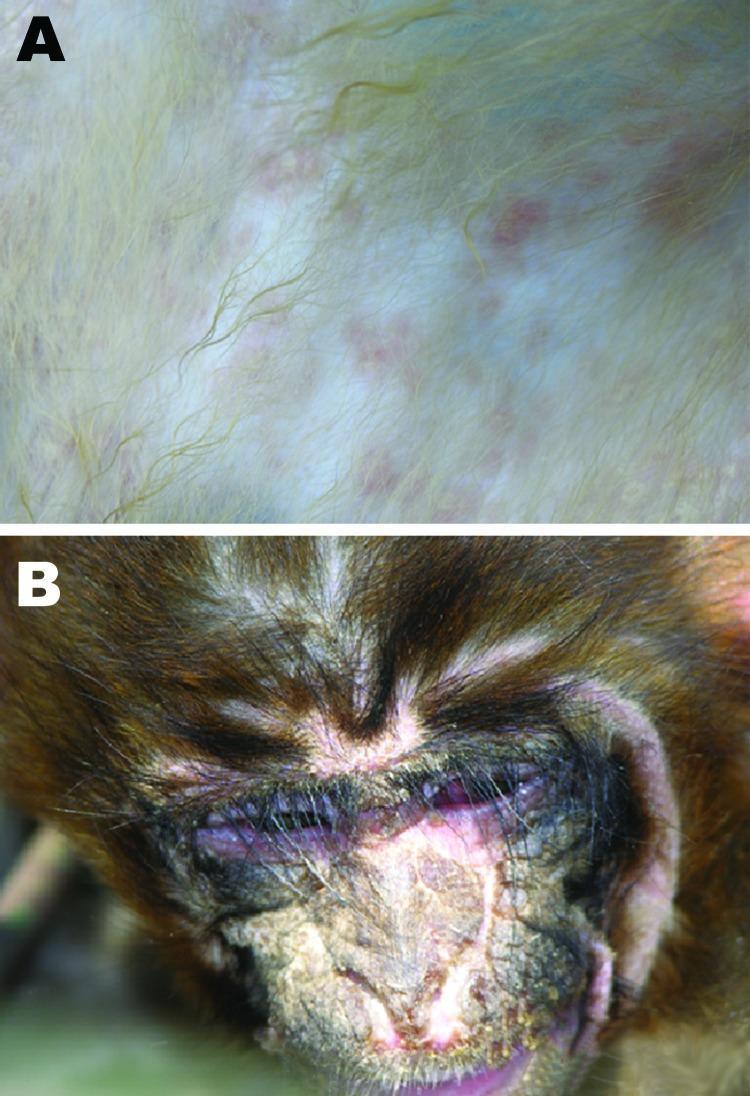
11. CLINICAL IMAGE — CDV Signs in a Morbillivirus Model
CDV (Morbillivirus) infection showing: (A) maculopapular rash on skin — erythematous macules 2–4mm diameter, reflecting epithelial tropism; (B) severe suppurative conjunctivitis with purulent exudate, periorbital inflammation, and nasal crusting — classic presentation of advanced CDV.
12. PUBLIC HEALTH / ZOONOTIC POTENTIAL
- CDV is NOT zoonotic — dogs CANNOT transmit distemper to humans
- However, CDV has been proposed as a co-factor in Paget's Disease of Bone in humans (controversial theory — CDV-like inclusions found in osteoclasts of Paget's patients — confirmed in our textbook sources)
- Ferret handlers should be aware that unvaccinated ferrets are highly susceptible and can serve as amplifying hosts
13. IMPORTANT CLIENT QUESTIONS (Jo owners puchtay hain)
Q1: "Mera kutta vaccinated hai, phir bhi distemper ho sakta hai?"
Yes, possible but rare. Vaccine failure can occur due to:
- MLV vaccine stored incorrectly (heat/light damaged)
- Vaccination during incubation period
- Dog was immunosuppressed at time of vaccination
- MDA interference in puppies
Q2: "Kya distemper contagious hai mere doosre kutton ke liye?"
Extremely yes. Isolate immediately. Disinfect premises. Vaccinate all unvaccinated dogs in contact (though this won't protect if already exposed within 3–5 days).
Q3: "Kya myoclonus (muscle twitching) theek ho jayega?"
Honest answer: Myoclonus is usually permanent. The underlying brain damage often doesn't reverse. Some dogs learn to live with mild myoclonus, but severe cases have poor quality of life.
Q4: "Kya meri billi ko bhi ho sakta hai?"
Domestic cats are resistant to CDV. No treatment needed for cats in the same household. (Wild felids like lions are susceptible.)
Q5: "Kitna expensive hai treatment?"
CDV hospitalization for 7–14 days with IV fluids, antibiotics, anticonvulsants can be significant. Honest cost counseling is essential. For severe neurological cases, discuss euthanasia humanely.
Q6: "Recovery ke baad dog theek ho jayega?"
Depends on form. Respiratory/GI: mostly full recovery. Neurological: permanent deficits likely. Hard pad resolves partially. Enamel hypoplasia in teeth is permanent.
Q7: "Kya iska koi antiviral treatment hai?"
No specific antiviral approved for clinical use. Treatment is supportive only.
Q8: "Ghar mein next dog kab la sakte hain agar ek mar gaya distemper se?"
Wait minimum 2–4 weeks (CDV survives briefly in environment, unlike parvovirus which survives months). Thoroughly disinfect premises. Ensure new puppy is fully vaccinated before introducing.
14. QUICK MEMORY SUMMARY TABLE
| Feature | Detail |
|---|
| Virus | RNA, Morbillivirus, enveloped |
| Most susceptible | Unvaccinated puppies 3–6 months |
| Transmission | Aerosol/respiratory (primary) |
| Systems affected | Respiratory, GI, Skin, Eyes, CNS, Teeth |
| Pathognomonic | Myoclonus + Hard pad + Chewing gum fits |
| Key lab finding | Lymphopenia + inclusion bodies |
| Best diagnostic test | RT-PCR |
| Treatment | Supportive — no specific antiviral |
| Prevention | Core MLV vaccine (DA2PPv) |
| Prognosis | Good (resp/GI); Poor (neurological) |
| Zoonotic? | NO |
15. CONCEPTUAL MNEMONICS
"DERN" — CDV clinical signs:
- Discharge (mucopurulent nasal + ocular)
- Encephalitis / neurological
- Respiratory pneumonia
- Nails/footpads (hard pad)
CDV = Canines + Demyelination + Virus (RNA)
Myoclonus = CDV's neurological fingerprint — no other common canine disease causes the same rhythmic, involuntary muscle twitching that persists even at rest.
Yeh tha Canine Distemper ka complete, comprehensive overview — virology se lekar prevention tak, pathognomonic signs se lekar differential diagnosis tak. Agar kisi specific section ko aur gehraai se samajhna ho (e.g., CSF analysis interpretation, vaccine immunology, neurological classification in detail, or koi aur specific case scenario), batao — woh bhi detail mein explain kar sakta hun.