Why does thyroglossal cyst moves with protruding tongue and degluttation
Reading File
Finding Sources
Searching the Web
thyroglossal cyst moves with tongue protrusion deglutition mechanism embryology
Reading File
Reading File
Reading File
Loading Image
Here is a thorough explanation backed by multiple textbooks.
Why a Thyroglossal Cyst Moves with Tongue Protrusion and Deglutition
The answer lies entirely in embryology and the resulting fibrous attachments.
Embryological Basis
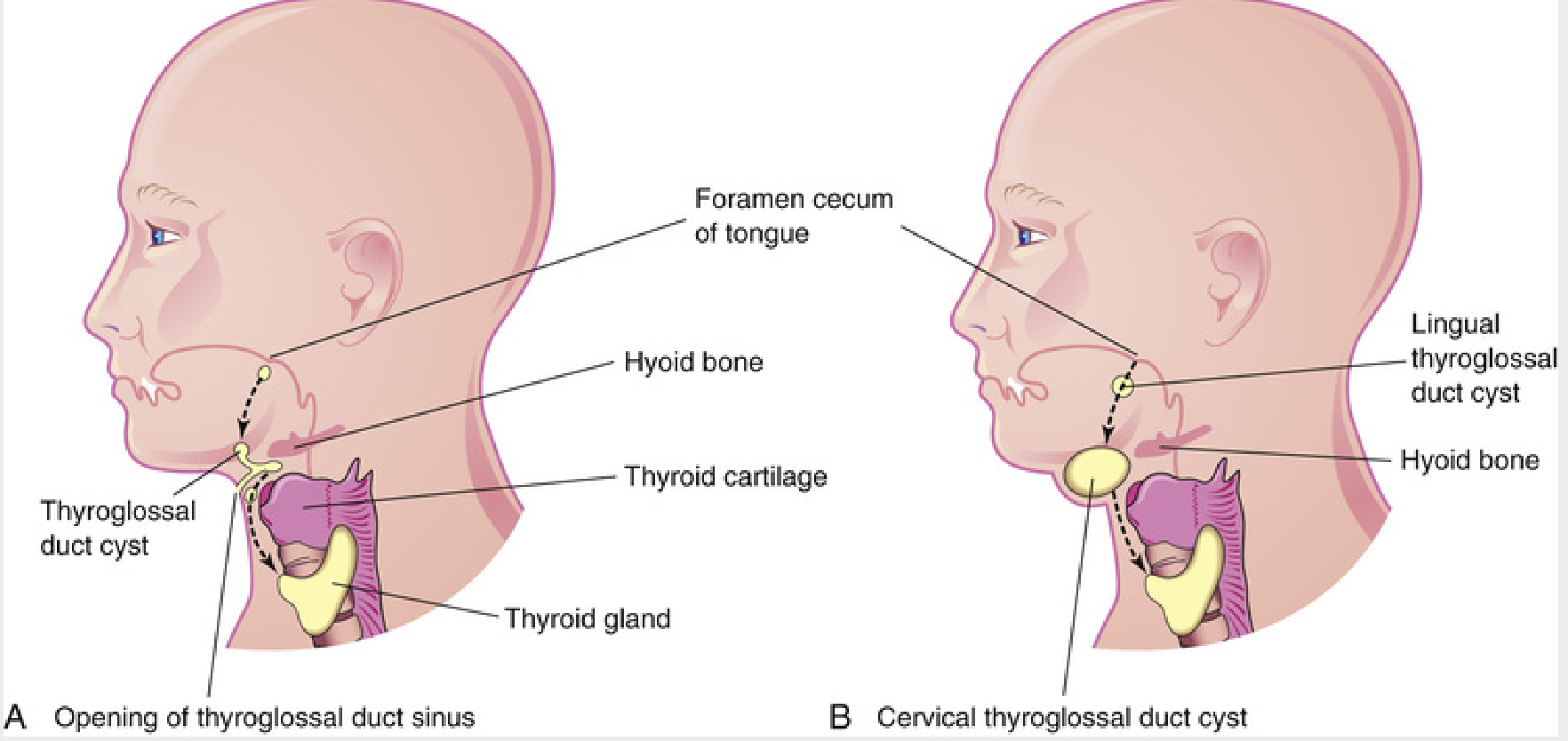
During the 4th week of development, the thyroid gland begins as an endodermal thickening at the foramen cecum - a pit at the junction of the anterior two-thirds and posterior one-third of the tongue. The gland then descends in the midline, passing through or just anterior to the hyoid bone, and reaches its final position in the anterior neck by the 7th week. The channel it travels through is called the thyroglossal duct.
Normally, this duct obliterates completely. If any segment persists, it can accumulate secretions and form a thyroglossal duct cyst - anywhere along the path from the foramen cecum to the thyroid isthmus.
Mechanism of Movement
There are two distinct mechanical reasons:
1. Movement with Tongue Protrusion
The thyroglossal duct remnant maintains its fibrous connection all the way up to the foramen cecum at the base of the tongue. This creates a fibrous cord running from the tongue base, through (or around) the hyoid bone, down to the cyst.
When the tongue is protruded forward and downward, the hyoglossus and genioglossus muscles pull the tongue out. This traction travels down the fibrous remnant of the thyroglossal duct, mechanically tugging the cyst upward and anteriorly.
As stated directly in Cummings Otolaryngology:
"Because of the attachments to the base of the tongue, thyroglossal duct remnants will move superiorly in the neck when the tongue is protruded."
This movement is highly characteristic and clinically pathognomonic - it distinguishes thyroglossal cysts from other midline neck masses (such as dermoid cysts, lymph nodes, or lipomas) that do NOT have this tongue connection.
2. Movement with Deglutition (Swallowing)
During swallowing, the hyoid bone is pulled upward and forward by the suprahyoid muscles (mylohyoid, geniohyoid, digastric, stylohyoid). Because the thyroglossal duct passes through the body of the hyoid bone (or is tethered to it), the cyst is mechanically dragged upward along with the hyoid.
This is why the thyroid gland itself also moves with swallowing - both the thyroid and any thyroglossal remnant are tethered to structures (pretracheal fascia and hyoid, respectively) that elevate during the pharyngeal phase of swallowing.
Key Anatomical Points
| Structure | Relevance |
|---|---|
| Foramen cecum (tongue base) | Superior attachment of thyroglossal duct |
| Hyoid bone (middle third) | The duct passes through or is closely adherent to it |
| Thyroid isthmus | Inferior end of descent path |
| Pretracheal fascia | Invests the cyst inferiorly, ties it to laryngeal structures |
This is also why the Sistrunk procedure (the definitive surgery for thyroglossal cysts) mandates removal of the middle third of the hyoid bone along with the cyst and a cuff of tongue muscle - simply excising the cyst alone leaves the duct remnant attached to the hyoid, leading to near-certain recurrence.
Clinical Pearl
These two movements together - upward with tongue protrusion AND upward with swallowing - are the two pathognomonic features of a thyroglossal cyst. S. Das's Manual on Clinical Surgery states plainly that these are the defining clinical signs of this condition. No other anterior midline neck mass shares both features:
- A dermoid cyst moves with swallowing but does not move with tongue protrusion (no tongue attachment)
- A submental lymph node moves with neither
- The thyroid gland moves with swallowing but not with tongue protrusion
Sources: Cummings Otolaryngology Head & Neck Surgery; Langman's Medical Embryology; S. Das Manual on Clinical Surgery (13th ed.); Sabiston Textbook of Surgery
Rose position for tonsillectomy
Finding Sources
Searching the Web
Rose position tonsillectomy patient positioning details neck extension
Finding Sources
Reading Web Page
https://www.theentresident.com/ent-notes-lectures/rose-posit…
Finding Sources
Finding Sources
Reading File
I have sufficient information from the web extraction. Let me now compile the complete answer.
Rose Position for Tonsillectomy
What is the Rose Position?
The Rose position is a supine surgical positioning technique used primarily for tonsillectomy and other oropharyngeal surgeries. The head is extended at the atlanto-occipital joint, placing the oral cavity and oropharynx in an optimal line of sight for the operating surgeon.
It is named after a staff nurse named Rose who reportedly suggested this position to the operating surgeon - an interesting piece of surgical history.
How is the Position Achieved?
The steps to set up the Rose position are:
- The patient is placed supine on the operating table
- A sandbag or shoulder roll is placed under the shoulder blades (not under the head)
- This causes the chest to elevate slightly, which in turn allows the head to fall backward - extending the neck
- The head hangs slightly off or at the edge of the headrest, extended at the atlanto-occipital joint
- The head is kept in the midline (no lateral rotation)
- For patients with kyphosis or a stiff neck, the headpiece of the table is raised so the head ring supports the head rather than letting it hang freely
The net result is: neck hyperextension + head in midline + slight backward tilt.
Why is this Position Used?
| Purpose | Explanation |
|---|---|
| Optimal oropharyngeal exposure | Extension opens the oral axis, bringing the tonsils into direct line of view through a mouth gag |
| Blood drainage away from airway | With the head lower than the pharynx, blood pools posteriorly and can drain down rather than into the trachea |
| Easier placement of Boyle-Davis mouth gag | The extended neck allows the gag to be opened and suspended from a Mayo stand without obstruction |
| Better surgical access | Surgeon sits at the head end; the extended neck shortens the working distance to the tonsils |
Surgeries Where Rose's Position is Used
- Tonsillectomy (most common indication)
- Adenoidectomy
- Uvulopalatopharyngoplasty (UPPP) for obstructive sleep apnea
- Cleft palate repair
- Pharyngoplasty
- Oropharyngeal tumor resection
- Base of tongue surgeries
- Foreign body removal from oropharynx
Contraindications
These are important exam points:
| Contraindication | Reason |
|---|---|
| Down syndrome | Atlantoaxial instability - hyperextension risks spinal cord compression (high-yield MCQ) |
| Atlantoaxial dislocation | Risk of cord injury with neck hyperextension |
| Cervical spine trauma/injury | Extension could worsen injury |
| Rheumatoid arthritis with cervical involvement | C1-C2 instability is common |
| Severe kyphosis or rigid spine | Cannot safely achieve the position |
| Unstable cervical spine from any cause | Absolute contraindication |
Equipment Used in This Position
- Boyle-Davis mouth gag - used to open the mouth and keep it open; suspended from a Mayo stand once the neck is extended in Rose's position
- Draffin bipod / Mayo stand - supports the Boyle-Davis gag
- Sandbag or shoulder roll - placed under shoulder blades to achieve the extension
Key Exam Points Summary
- Position: Supine + neck hyperextended at atlanto-occipital joint
- Sandbag placed under shoulders, not the head
- Head hangs in midline, extended backward
- Most important contraindication: Down syndrome (atlantoaxial instability)
- Named after a nurse named Rose, not a surgeon
- The extension allows the Boyle-Davis gag to be properly suspended and used
Tonsilar and adenoid enlargement grading
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.